
Abstract
Objective: The influence of impaired renal function on the pharmacokinetics of single and multiple doses of cerivastatin was evaluated in this non-randomized, non-blinded, 7-day, multiple-dose study.
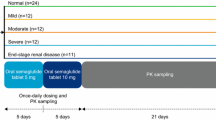
Methods: Thirty-five adults between the ages of 21 years and 75 years with normal renal function (CLCR >90 ml/min/1.73 m2, n=9), or patients with either mild (CLCR 61 ml/min/1.73 m2 to ≤90 ml/min/1.73 m2, n=9), moderate (CLCR 30 ml/min/1.73 m2 to ≤60 ml/min/1.73 m2, n=8), or severe (CLCR <30 ml/min/1.73 m2, but not on dialysis, n=9) renal impairment were given cerivastatin 0.3 mg daily each evening for 7 days. The steady-state pharmacokinetics of cerivastatin, including the area under the concentration–time curve (AUC)0–24, peak plasma concentration (Cmax), time to reach Cmax (tmax) and elimination half-life (t1/2), were determined on day 1 and day 7. The logarithm of the pharmacokinetic variables was analyzed using analysis of variance (ANOVA). Safety assessments included physical examination, fundoscopy, vital signs, electrocardiogram (ECG), adverse events, and laboratory safety indices.
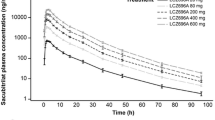
Results: The day-1 AUC in patients with mild renal impairment was similar to that of patients with normal function (19.6 μg/h/l vs 19.2 μg/h/l, respectively). However, the AUC for cerivastatin patients with moderate or severe renal impairment was 40–60% higher (30.8 μg/h/l and 29.0 μg/h/l, respectively). Cmax values for patients with normal, mild, moderate, and severe renal impairment were 3.3, 3.4, 4.6, and 5.2 μg/l, respectively. This modest increase in plasma cerivastatin levels is nearly equivalent to a 0.4-mg daily dose, which has been recently approved in the United States. The mean t1/2 of cerivastatin was less than 4.5 h in all patients, indicating that renal dysfunction did not promote cerivastatin accumulation. This observation was confirmed by the finding that the cerivastatin plasma levels on day 1 and day 7 were similar in all patient groups. Furthermore, the mean AUC and Cmax values for both demethylated and hydroxylated cerivastatin were similar in the patients with the most severe renal dysfunction to the corresponding values in healthy subjects. Cerivastatin was well tolerated in all patients irrespective of renal function. Adverse events were observed in 37% of the subjects; nearly all were mild and generally of short duration, and most resolved without intervention. Incidence of adverse events was similar across all three renal groups and the control group. There were no clinically significant laboratory changes other than those consistent with renal disease.
Conclusion: This study demonstrates that dosage adjustment of the daily 0.3-mg cerivastatin dose in patients with significant renal impairment is likely unnecessary.
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Received: 2 August 1999 / Accepted in revised form: 12 January 2000
Rights and permissions
About this article
Cite this article
Mazzu, A., Lettieri, J., Kelly, E. et al. Influence of renal function on the pharmacokinetics of cerivastatin in normocholesterolemic adults. E J Clin Pharmacol 56, 69–74 (2000). https://doi.org/10.1007/s002280050723
Issue Date:
DOI: https://doi.org/10.1007/s002280050723