Pursuing Sustainability for Healthcare through Digital Platforms



1
Department of Economics and Statistics, University of Salerno, 84084 Fisciano, Italy
2
Department of Management & Innovation Systems, University of Salerno, 84084 Fisciano, Italy
*
Author to whom correspondence should be addressed.
Sustainability 2019, 11(1), 165; https://doi.org/10.3390/su11010165
Submission received: 28 November 2018
/
Revised: 18 December 2018
/
Accepted: 21 December 2018
/
Published: 29 December 2018
(This article belongs to the Special Issue Sustainability for Healthcare)
Abstract
:Sustainability, as well as the sustainable use of resources and related issues, has inspired a long-lasting and lively debate among scholars of different disciplines. Due to under-investigation of several of the sustainability-related challenges, this paper aims to better understand the system dynamics that, supported by some digital enablers (e.g., digital technologies and platforms), boost the sustainability of complex service systems such as healthcare. To this end, the theoretical meta-model of interaction types, which inspired the prototype digital platform dedicated to the online delivery of health-related services, is presented. Moreover, some healthcare usage scenarios, based on the prototype’s functions, are analysed and discussed. This allows understanding of how important the role of technologies and, in particular, digital platforms, are in empowering actors and in making them willing to interact, and share their own resources in continually new ways. This paves the way for ongoing value co-creation, which is essential for healthcare system sustainability.
1. Introduction
Moving on from the seminal assumptions of the Brundtland report [1], sustainability has gained momentum over the years, attracting the attention of scholars belonging to different disciplines [2]. This has also led sustainability research to go beyond the initial mere environmental perspective to also approach the social and economic domains. Even though the notion of sustainability is broadly whispered and accepted, the ways it has been explored and conceptualized remains vague and somewhat blurred [3,4]. Thus, being multifaceted concepts, sustainability and sustainable development cannot be approached in a similar and integrated way. Therefore, they call for balancing socio-ecological and socio-technical systems, which their several inner interactions make inherently complex [5]. Thus, sustainability has to face complex issues arising from the intricate and often unbalanced human-based and social interactions that affect decision-making at social, economic and environmental levels. To challenge these issues, a multi-disciplinary approach is required [6,7].
This study, aiming to investigate sustainability in complex service systems such as healthcare, has been based on the foundational premises of system thinking [8,9] and the Viable System Approach (VSA) [10], which go beyond the traditional reductionist approaches [11]. In fact, healthcare is one of the most critical service domains, whose complexity mainly arises from the fact that it has to deal with people’s health and wellbeing. It follows that a number of related issues should be addressed, such as, among others, health services effectiveness, cost efficiency [12], and, at the same time, the ability to offer high quality and personalized services [13]. Therefore, the main aim of this study is to better understand if and how structural relationships can enhance the interactions between the actors that populate healthcare systems (e.g., health providers, patients, families, institutions, etc.), boosting the sharing of resources—mainly information—and in so doing, nourishing the long-lasting sustainability of the whole system. In this direction, the pivotal role of information and communication technologies (ICTs), and of the most recent digital platforms, in enhancing or constraining the interactions and the subsequent resource sharing among a number of different actors will be investigated using the interaction type meta-model [14]. However, it is worth noting that even though organizational, managerial and economic research has often approached the influence of ICTs on health service efficiency [15] and, partially, on its effectiveness, the literature still calls for a better understanding of its potential in adding sustainability to complex service systems. Therefore, this study aims to contribute towards bridging this gap, analyzing the potential of a digital platform for reconciling effectiveness, efficiency and sustainability targets in a real health service context [12,16,17]. To achieve this goal, healthcare systems should shift from a mere efficiency and effectiveness orientation, towards a more holistic and harmonized vision [16,17], aiming to add sustainability to the whole system. This analysis was aimed at understanding if and how digital platforms can trigger long-lasting interactions among the different actors who populate the complex and dynamic healthcare service system [18]. In this way, the mainstream definition of healthcare system was advanced, conceptualizing it as a set of activities mainly intended to promote, restore and maintain health [19].
The remainder of the paper is organized as follows. The next section reviews the theoretical background on which the proposed approach to health sustainability has been developed. Then, the theoretical meta-model of interaction types, on which the digital prototype has been designed, is described. Then follows the presentation and the discussion of the digital platform prototype and its role in adding sustainability to healthcare systems. Finally, implications and future research paths are proposed.
2. Theoretical Background
2.1. A Systemic Approach to Healthcare Sustainability
In recent years, service research devoted greater attention to sustainability, conceptualizing it in several and, sometimes, different ways [12,20,21]. Dealing with this fragmentation and recognizing the inner complexity of sustainability, scholars [22,23,24,25] called for further approaches that are able to grasp the dynamic relationships that inherently characterize it [26]. In this direction, system thinking [8,9] and the VSA [10,11], built upon the Viable System Model of Stafford Beer [27], represent two suitable approaches for advancing the traditional definition of sustainability, moving it towards an integrated and system approach. These theoretical frameworks consider it as a complex network of components, relationships and active interactions, occurring over a specific period of time [28], between different actors, aimed at reaching shared goals.
Focusing on relations and interactions, it is worth noting that these concepts are closely linked to one of the essential elements of system thinking, the structure–system dichotomy [10,11], built upon a dual approach (static and dynamic) to the observation of the extant reality. Drawing on these two concepts, Golinelli and Gatti [28] defined the former as a logical or physical connection between the components of a structure and the latter as the activation of a structural relation, which occurs when resources, data, or both, are exchanged between different actors, willing to share their knowledge in order to achieve a common goal. It follows that interactions reflect those dynamic behaviours that can change a structure into a system.
Shifting the focus to the VSA, it represents a suitable interpretative lens for better understanding the importance of sustainability for the viability of complex service systems [29]. Thus, healthcare systems are well suited to the mainstream definition of service systems, according to which they are dynamic configurations of resources (people, technology, organizations and shared information), which create and deliver, through service, value for both providers and customers [30]. Moreover, healthcare can be further considered to be a complex and adaptive service system, being a value co-creation configuration of people, technology, internal and external service systems connected by value propositions and shared information, for example language, laws, measures and [29,30,31]. Thus, healthcare complexity mainly lies upon the interrelations of several different and sometimes opposite economic, functional, emotional and ethical needs and expectations [32]. Drawing on the aforementioned healthcare complexity, Saviano et al. [33] empathized the need for coupling and balancing its traditional targets of efficiency and effectiveness with sustainability, in order to boost the viability of the whole health service system. It follows that the traditional principles at the core of business practices, based on a problem-solving oriented approach, are still aimed at solving just one short-term priority after another, without a strategic orientation and a clear sense of direction [19]. Therefore, a new approach to the different interests and goals is needed, as well as to the number of intricate and non-linear interactions occurring between individuals, organizations and institutions, which populate the healthcare service system and which often generate unexpected outcomes [34]. In fact, even though healthcare remains mostly focused on mere operational efficiency, trying to be compliant with the expectations of political and institutional supra-systems, a new orientation is rising. This is aimed at also meeting service effectiveness, and therefore, at changing the role of patients as well as at combining resources in a more sustainable way. This new orientation calls for a radical change in service providers’ mind-set, who should be focused on better satisfying patients, moving from the traditional doctor-patient relationship toward a provider–client relationship [13,35]. Two essential concepts at the core of the health provider–client relationship, as well as of the recent healthcare general reformation, are the empowerment of patients and the patient-centered approach to care [36]. These two concepts are based on the exploitation of the patients’ ability to always improve their self-reliance and competence with disease [37], making them able to actively participate in health service provision. This has led beyond the enduring information asymmetry that traditionally affects physician–patient relationships. More in details, information asymmetry is mainly due to patients’ dependence on the providers of care [38], which constrains the mutual and future-oriented use of resources needed for healthcare sustainable development. This is at the core of sustainable development for healthcare. In fact, being a dissonant interpretation of schemes and categorical values [33], information asymmetry, together with patients and health professionals’ inability or unwillingness to share their personal resources (information), might prevent the (co)creation of value for the whole healthcare service system [39], leading, in turn, to the destruction of it. Thus, the sustainability of healthcare service systems can benefit by the actors’ willingness to align their strategies and, at the same time, to always adjust and adapt themselves and their behaviour to the contextual changes [40]. In this direction, the recent advancements of ICTs and the rising implementation of digital platforms has further boosted the empowerment of patients and the progressive overcoming of the aforementioned information asymmetry, enhancing the interaction between health professionals, patients and other people (e.g., families, peers, citizens, institutions, etc.).
2.2. The Role of ICTs and Digital Platforms for Healthcare Sustainability
Following a well-established service research path [29,30,41], there seem to be two essential elements of a healthcare service system; people and technology [27]. People (health providers, patients, families, peers, etc.) represent the main source of variety, intended as a unique individual combination of quantitative and qualitative dimensions in which psychological, emotional, cognitive and cultural elements affect the processes occurring in a specific system. Technologies and, in particular, digital platforms, represent what can really boost the interactions among people, offering more effective information management [42]. Even though organizational and managerial research has deeply investigated technologies’ influence on health service quality in terms of process efficiency [15], the literature still calls for a better understanding of their influence on effectiveness, intended as a result of people interactions and their contribution to the co-production of personalized health services and their sustainability. Thus, the personalization of health-related services lies not only upon the ability to fit medical conditions to patients, but also on further dimensions such as their age, mental and social conditions, personal traits, preferences, family circumstances and financial capacity [43]. Therefore, even if this customization generally leads to costs’ increasing [44,45], digital technologies seem to be even more able to face and constrain it. This is mainly due to their ability to renew and offer a more efficient organization of the processes lying at the core of health service delivery [46]. At the same time, ICTs and digital platforms are also able to improve the effectiveness and the quality of provided services. This makes them even more patient-centered due to the real and the ongoing active participation of empowered patients, who can now access, mainly via digital devices, a huge amount of information that nourishes their ability to self-manage their disease. It is worth noting that technologies and, in particular, digital platforms, can act as interactions’ enablers, activating specific and dynamic relationships between different actors, who can mutually share their resources to always create new ones and, in so doing, ensure the long-term sustainability of the whole healthcare system. In particular, digital platforms have boosted the access to resources (mainly information) and to more reliable source of knowledge; therefore, patients, as well as other people, can individually improve their understanding and awareness of medical issues and, in so doing, be involved in the whole health service provision [47]. Finally, digital platforms are also able to increase resources’ accessibility and the emergence of more sustainable multi-actor interactions, based on resource sharing, cooperation and networking [48]. In summary, the implementation of health digital platforms can help face the complexity of this service domain, balancing efficiency (or doing things in the right way), effectiveness (or the right things that must be done) and sustainability (or the effort towards the establishment of the right relationships with other systems) [49], as well as adding long-term sustainability to healthcare.
3. The Interaction Type as a Bridge between Relationship and Interaction: A Proposed Model
The meta-model presented in this section has been built upon the conceptualization of the interaction type, here intended as a bridging concept able to facilitate the shifting from the structural concept of “relationship” toward the systemic concept of “interaction” [14]. Thus, assuming a system approach, the interactions occurring between different actors let them share and combine resources in order to (co)create value that nourishes the sustainability of a whole service system, balancing it with both efficiency and effectiveness targets.
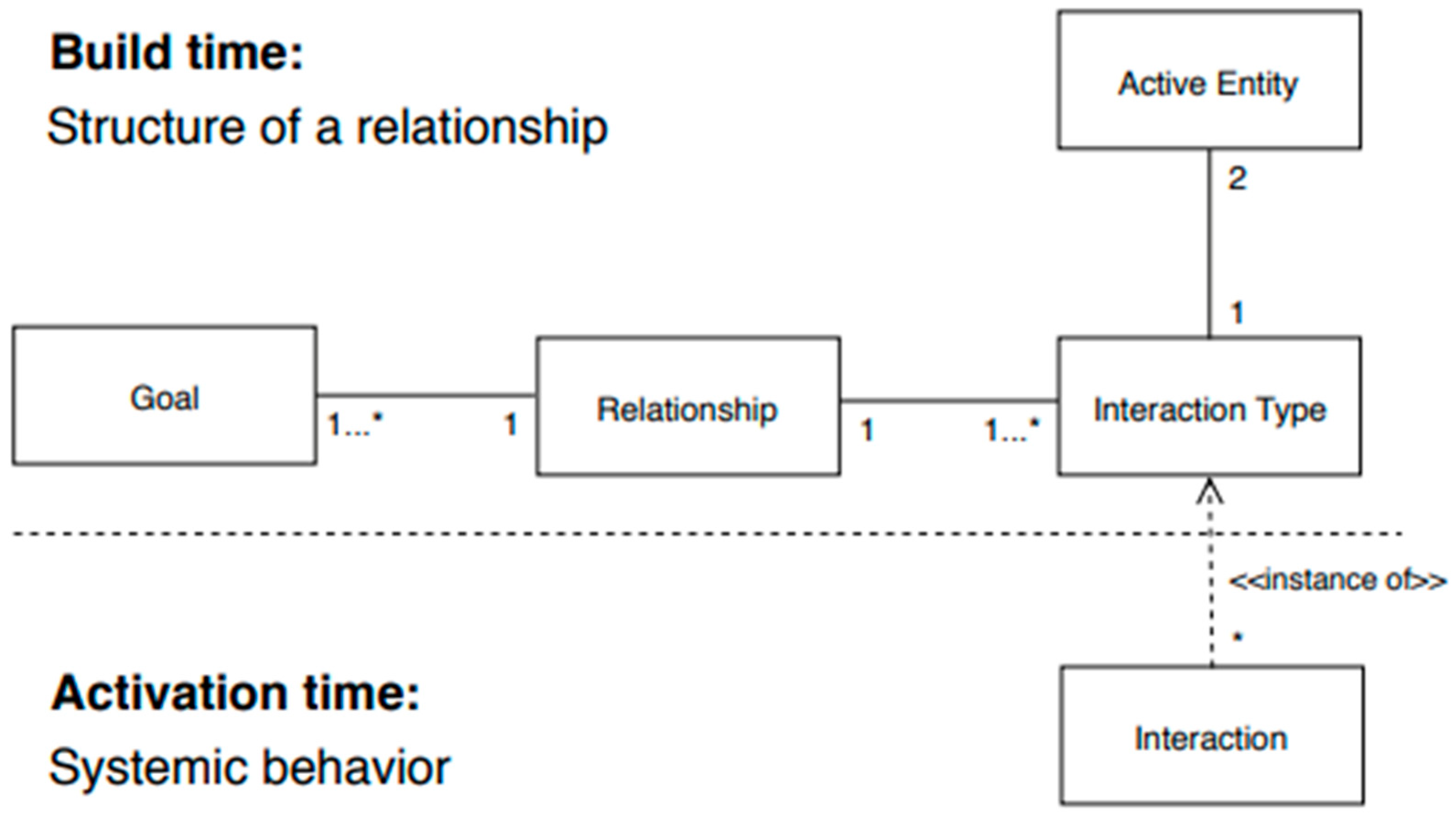
The interaction type meta-model is here intended as the theoretical foundations on which specific digital applications can be designed. Thus, it has inspired the development of a digital platform prototype which will be presented in the following section (see Par. 4.), designed for facilitating online interactions and, therefore, the provision of personalized services in a healthcare setting. To better depict the inner nature of the meta-model, a class diagram has been designed (see Figure 1) using unified modelling language (UML) [50]. Thus, Figure 1 shows the foundational concepts of the interaction type meta-model as well as the logical connections existing between them. In particular, the following concepts are represented as classes in the diagram:
- Goal—something that individuals or organization try to do or to achieve;
- Active entity—an organization, an individual or even an automated component able to assume a specific behaviour when interacting with other active entities;
- Relationship—a logical or physical connection between the components of a structure or those relationships; thus, relationships, facilitating communication, make it possible to boost the interaction between active entities;
- Interaction—a concrete action involving at least two active entities and aiming to reach a specific and shared goal;
- Interaction type—the structural element that shapes a specific kind of interaction and which qualifies one or more interactions, offering them an external shape or configuration.
Looking at the logical connections between concepts, as depicted in Figure 1, the multiplicity symbols 1, 2, and *, placed near the endpoint of each link, allow the diagram to be read as follows. A relationship exists between 2 active entities if there is at least 1 interaction type that connects them. Furthermore, a relationship comprises one or more interaction types (1..*) and has one or more goals. For example, the relationship existing between a doctor and a patient, based on this latter illness, can have several different interaction types, such as, for example, appointment booking, medical examination, clinical analysis, vaccination, etc. The dynamic aspects of a relationship are taken into account by the notion of interaction; in this model, an interaction is a particular occurrence of an interaction type (an instance of) and can be observed many times (*) with the behavioural pattern stated by the interaction type.
The interaction type can assume a simple or an aggregate form, where a simple interaction type can be defined as a message flowing from one entity to another. An interaction type is recognized through a unique identifier or code, the itName. In detail, a simple interaction type depicts the structure of an atomic interaction (e.g., messages exchange) occurring between two active entities, which is noted as follows:
where constraints either enable the activation of this specific interaction type or do not. To better understand the inner nature of a simple interaction type, it can be useful to shape an expressive example, such as when a patient books an appointment with a doctor. Therefore, the simple interaction type that describes the structure of the “potential interaction” occurring in that case between a patient and a doctor is:
itName = {activeEntity1, activeEntity2, goal, messageStructure, constraints}
| appointment booking = {patient, doctor, to get an appointment, |
| “message for the appointment request”, |
| “to be in touch”}. |
It worth noting that an interaction happens just when a specific interaction type, which links a patient and a doctor together, is activated. Two expressive examples of interactions fitting with the “appointment booking” interaction type follow:
| i1 = {mr. Brown, dr. White, to get an appointment, |
| “I have a stomach ache, please book me an appointment” |
| “mr. Brown and dr. White are in touch”}, |
| i2 = {mr. Brown, dr. White, to get an appointment, |
| “I feel sick, please book me an appointment” |
| “mr. Brown and dr. White are in touch”}. |
It is also possible to shape a set of interaction types, which group the related active entities and define the actions that can occur between them, in order to better focus each specific interaction. To describe the structure of complex behaviours, the meta-model used the notion of aggregate interaction type, which is a set of two or more simple or aggregate interaction types and which is formalized as follows:
where the notation goal represents the goal of the whole set of interactions in setOfInteractionTypes and constraints either enable or not, the activation of all the interaction types belonging to the selected set. To better understand the nature and the functioning of aggregate interaction types, a real example of it, named “medical examination”, follows:
| aitName = {activeEntity1, activeEntity2, goal, setOfInteractionTypes, constraints} |
| medical examination = {patient, doctor, to solve a health problem, |
| {appointment booking, take a physical, medical report, payment} |
| select all}. |
The constraint “select all” implies that all the interaction types belonging to the setOfInteractionTypes named “medical examination” need to be activated. It worth noting that the higher-level goal, named “to solve a health problem”, is achieved only when all the other (sub)goals of the setOfInteractionTypes are accomplished. Thus, the (sub)goal of the interaction type “appointment booking” have to be necessarily and preliminary accomplished to continue the interaction between a patient and a doctor. Therefore, as the following example shows, other interaction types can be added to the patient–doctor relationship, such as:
| follow up = {patient, doctor, to monitor the patient health status, |
| “information about the progress of the therapeutic plan” |
| “to be in touch”}. |
This implies that a strong interaction type implies a strong link between patient and doctor.
4. Designing and Implementing A Digital Platform for Healthcare Services Sustainability: A Prototype
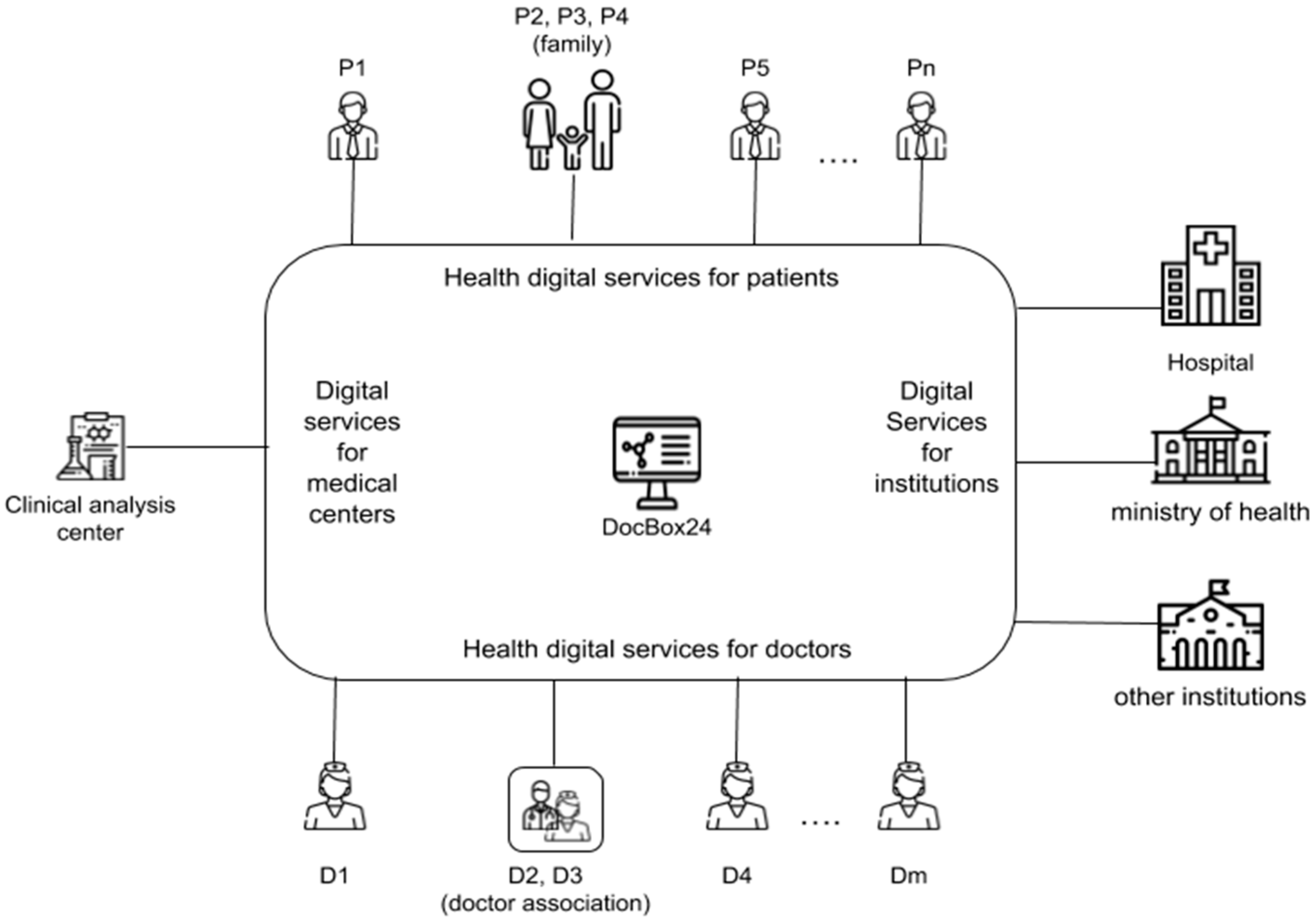
Drawing on the interaction type meta-model, a prototype digital platform, DocBox24, has been developed to better understand the way a digital application can boost the interactions usually occurring between doctors, patients and all the other actors that populate healthcare systems (e.g., hospitals, private clinics, clinical analysis centres, Ministry of Health, other health institutions, etc.).
Being built upon the results of a long-term research project, DocBox24 main functions are:
- connecting physicians who work as freelancers with patients in a single application context;
- offering a complete set of digital services (e.g., booking, visit/report, follow up, etc.);
- provide an authorized access to health-related data to patients, physicians, public institutions and private health organizations;
- maintaining a single database, which can be used for predictive analysis through machine learning algorithms;
- integrating the existing or future digital, and even wearable, devices for data recording and analysis.
As stated, DocBox24, being designed on the logical foundations of the interaction-type meta-model described in the previous section, aims to facilitate actors’ interactions and, therefore, mutual information-sharing, fundamental for offering updated and personalized health service and for improving health-related processes, is ongoing. In this direction, Figure 2 depicts the top-level architecture of DocBox24 in order to offer a better understanding of the possible interactions that the digital platform can enable between different actors or active entities.
The interaction types that the digital platform can activate are summarized in the following tables. In particular, Table 1 describes some aggregate interaction types, while Table 2 describes some other simple interaction types. However, both of them are simply representative of the involvement of some active entities in a specific relationship. At this level of analysis, only the description of the relationships occurring between three actors or active entities: individuals, health service providers and institutions, has been provided. In particular, the first three interaction types described in Table 2 can occur when the aggregate “medical examination”—described in Table 1—is activated.
The simple interaction type “appointment booking” and “medical report” already appear as components of “medical examination”. The interaction type “symptoms” is, indeed, a component of “take a physical”, which belongs to “medical examination”. It is worth noting that this example allows one to grasp the recursive nature of interaction types. Furthermore, the interaction type “information sharing” involves two active entities (e.g., two different patients), while the latter one depicts the periodical data transmission from doctor to the Department of Health.
Being DocBox24 a mediator of interactions and an enabler of health digital services, the traditional relationship:
active entity 1—active entity 2, must be reinterpreted—as follows—as a couple of relationships:
- -
- active entity 1—healthcare digital platform;
- -
- healthcare digital platform—active entity 2.
When the communication between active entity 1 and active entity 2 is bidirectional, more than two interaction-types can be involved. This situation happens, for example, when the structure and the goal of the traditional interaction type “appointment booking”, occurring between patient and doctor, is broken into the following sequence:
- patient-DocBox24, for appointment booking, initiator: patient
- DocBox24-doctor, for appointment request, initiator: DocBox24
- doctor-DocBox24, for appointment scheduling, initiator: doctor
- DocBox24-patient, to confirm the appointment, initiator: DocBox24
Even if the huge amount of possible interaction types leads one to consider the interactions occurring between the active entities complex, the digital platform offers a concrete solution to it, boosting:
- (a)
- asynchronous interactions, which no longer need the simultaneous presence of all the active entities who participate in the interaction;
- (b)
- the ongoing improvement of the interaction, for example in terms of interactions’ number reduction, process efficiency and effectiveness, service cost reduction and similar;
- (c)
- (d)
- the provision of new services, such as the cloud management of an electronic health record (EHR), based on ubiquitous, always available, but protected access;
- (e)
- the data collection and the subsequent statistical analysis and data mining.
An example of the DocBox24 function intended to improve the analysis of processes, based on the reduction of the number of interactions, follows. At time t0, the role “doctor” activates an interaction with DocBox24, aiming to publish an appointments’ timetable based on a temporal frame, for example a month:
| publish timetable = {doctor, DocBox24, |
| to publish the timetable for appointments in the next period, |
| “timetable” |
| “the doctor is registered in DocBox24 and can access its services”}. |
For each period of time t1 with t1 > t0, a free time slot is available in the doctor timetable, while the single interaction type that a patient has to activate is:
| appointment booking = {patient, DocBox24, |
| “select a free slot in the doctor timetable” |
| “the patient is connected to DocBox24”}. |
Table 3 provides an overview of the interactions that DocBox24 can activate between the active entities typical of a specific interaction type. In particular, it describes how two active entities—the doctor and the patient—can manage a patient’s EHR. The patient can completely manage his or her EHR, while the doctor can modify just the sections of his or her competence.
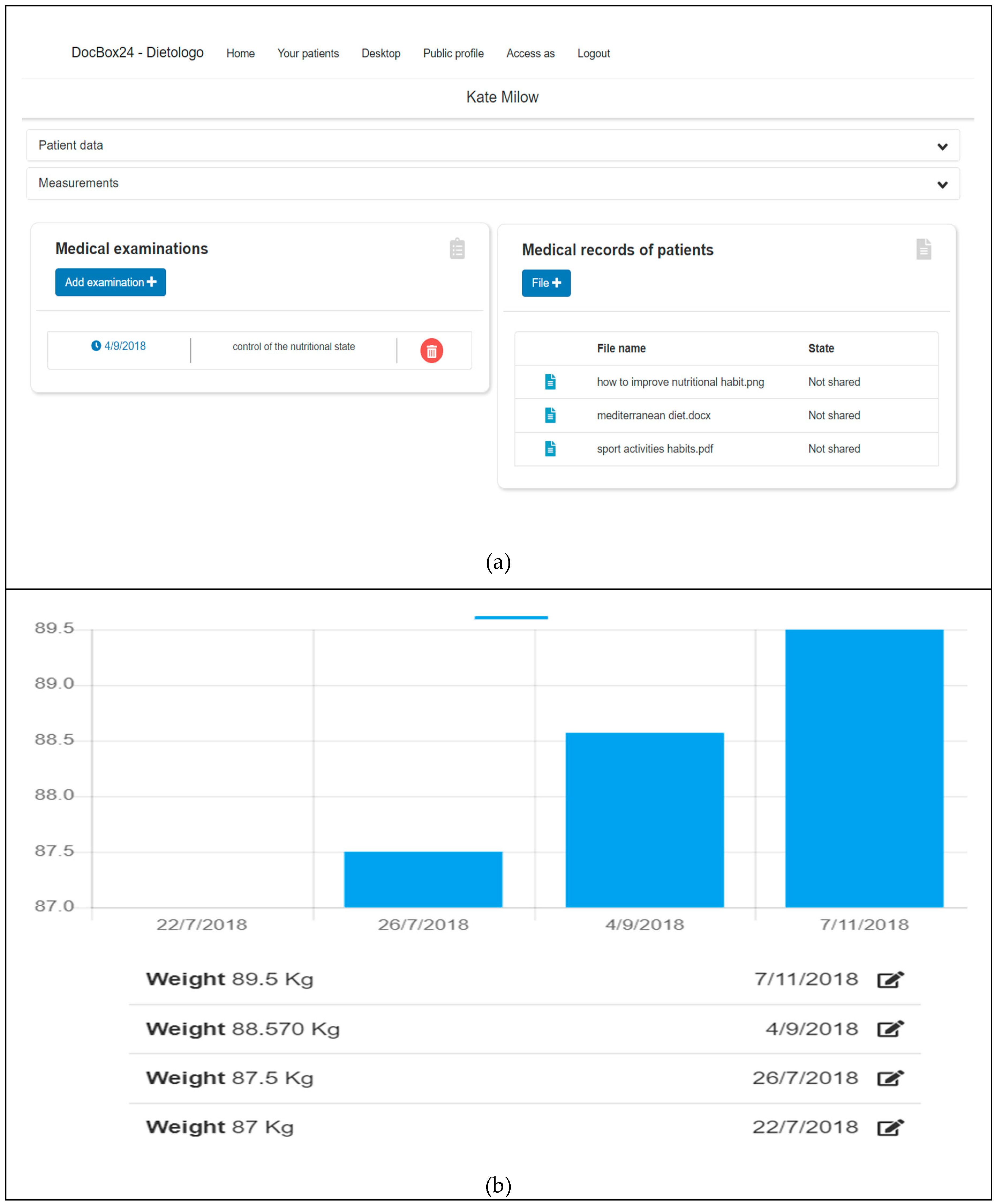
A graphic description of the implementation of the interaction type “Electronic Health Record2” (see Figure 3) follows, which delves into the doctors’ view of a patient’s EHR and is made up of three main sections. The first dedicated to the recording of patients’ personal data, the second to the measurements of their vital parameters and, finally, the third to the attachment and recording of medical examination and patients’ files in the EHR. In particular, Figure 3a,b provides an example of a nutritionist examination, depicting a graphical representation of a hypothetical patient’s (Kate Milow) weight measurement trend.
5. Discussions
DocBox24, the prototype digital platform presented in the previous section, offers some concrete examples of the way multi-actor interactions can add sustainability to a healthcare service system. Due to the fact that the platform is built upon the interaction type meta-model, it can lead to better understanding of the way structural relationships are activated when actors’ resources (data, information and knowledge) [51,52] are exchanged through mutual interactions that contribute to changing a structure into a system. Moreover, the dynamic nature of the interaction types at the core of the analyzed platform underlines the way a digital infrastructure can enhance the generativity [53] and, therefore, the involvement of different actors in the co-production of the health service, making it as fitting as possible with ever-changing social expectations and needs [54]. In this direction, the digital platform can be considered an interactions’ enabler, being able to activate specific and dynamic relationships between different actors belonging to the healthcare service system (e.g., physicians, patients, families, health service providers, institutions, etc.). In so doing, the platform also supports the sharing of resources, enhancing their accessibility [55] and, therefore, the actors’ ability to retrieve more reliable sources of knowledge.
As interactions’ enablers [56], digital platforms, such as DocBox24, are able to facilitate the aforementioned interactions and, consequently, an ongoing and mutual resource exchange, which triggers those mechanisms and processes that contribute to sustainability in healthcare systems, which are patients and other actors’ empowerment, the reduction of information asymmetries and the co-production of even more personalized health-related services. In detail, the platform supports the empowerment of patients, allowing them access to a growing and detailed amount of health-related information, which increases their knowledge about their specific disease, as well as other possible health-related issues. This implies that patients and the actors belonging to their personal network can improve their self-reliance and competence with disease, which makes them willing to participate in the provision of even more personalised health-related services. In particular, the prototypal digital platform boosts the involvement of a number of actors, who—performing as active entities—can cooperate and activate those network interactions [48] essential for the ongoing improvement of health services. These interactions are also nourished by actors’ participation, as well as by their continually updated understanding and awareness about medical issues [47]. In fact, offering a shared and open access to resources (e.g., information and knowledge), based for example on the implementation of EHR and on the open access to a growing amount of health-related information and data, the digital platform helps gradually counteract the information asymmetry that traditionally affects doctor–patient relationships [38]. Thus, due to their growing awareness and knowledge, health actors others than physicians can act, mainly through the platform’s functions, as real contributors to the co-production of more personalized health services as well as to the co-creation of value for themselves and others [57]. In fact, actors can share their own resources through those service-for-service exchanges that pave the way for ongoing value co-creation [56,58], which in turn, nourishes the viability and, therefore, the long-run sustainability of the health service system. Therefore, the implementation of such a digital platform can add sustainability to this specific service domain, balancing the traditional need for efficiency, reducing the time and costs of health-related processes, with the lively need for an ongoing improvement of service effectiveness. In this direction, the implementation of the prototypal platform contributes towards services becoming more efficient and to reducing the waiting times and almost all space constraints through the digitalization of health services. Moreover, service digitalization implies the possibility of better managing other significant health issues, such as service’s costs, waste reduction and similar [59], without downgrading the quality of the provided service, but rather making it as effective as possible. This is also possible thanks to patients and other actors’ contribution in terms of customization, ongoing improvement and in offering complementary services (e.g., physiological support, social services, educational service, etc.). It follows that DocBox24, facilitating the access to resources, triggers patients and other actors’ ability in self-managing diseases and a plethora of more general medical problems.
In summary, assuming a systemic approach to sustainability, the prototype platform, enhancing multi-actors interactions and, therefore, boosting an enduring process of resource sharing and the subsequent circular creation of new and high order resources, can trigger that ongoing co-creation of value fundamental to ensure the long-term sustainability of the whole healthcare system.
This contributes towards making the actors’ relationships stronger and longer lasting, as well as promoting an even more conscious use of material and immaterial resources (e.g., financial resources, drugs and medications, medical devices, information, etc.).
6. Conclusions
Assuming a systemic approach, this paper supports a deeper understanding of those multi-actors’ interactions at the core of health service provision, trying to balance different and sometimes opposite targets, such as the need for efficiency, effectiveness and sustainability, shaping a general, mutual and long-lasting vision of healthcare sustainability [27,33].
Moving from the main assumptions of the VSA conceptual framework, this analysis offers better comprehension of the effects that the numerous and complex interactions can have on the viability and, in the long-term, on the sustainability of the healthcare system. Thus, this study contributes to advancing the systemic approach to the sustainability of healthcare systems, underlining how digital platforms, acting as multifaceted intermediaries of interactions, can boost the exchange of resources among the different actors or the active entities that populate this service system. In so doing, digital platforms nourish those value co-creation patterns essential for the enduring improvement of health outcomes and, therefore, for actors’ long-lasting well-being, which is the sine qua non for the sustainability of healthcare service systems. In this specific service context, this is mainly due to the ability of digital platforms in facilitating patient and other actors’ engagement in resource integration [60], empowering them also providing friendly and easy-to-understand health-related information [61].
In terms of managerial implication, the potential of such digital platforms calls for a change in public and private healthcare management, which should promote a smarter and wider use of these tools in order to stimulate a dynamic and multi-actor dialect, aiming to combine the healthcare need for efficiency, effectiveness and sustainability. Moreover, acting as an interactions’ enabler, digital platforms enhance resource sharing and, consequently, they can perform as data manifold, a role that should be further investigated, focusing on the implementation of big data techniques and data mining procedures in healthcare, as well as other service contexts. This will help grasp those inner trends rising from the ICTs’ mediated interactions, which generate a huge amount of data. Finally, further research should investigate the influence that actors-generated big data sources can have on the value co-creation process that adds sustainability to complex service systems.
Author Contributions
Conceptualization, G.N.; Methodology, S.C. and G.N.; Software, F.D.N.; Formal Analysis, F.D.N.; Investigation, G.N., S.C., and M.F.; Resources, G.N.; Writing-Original Draft Preparation, S.C.; Writing-Review & Editing: M.F.; Visualization, S.C., M.F., F.D.N., G.N.; Supervision, G.N.
Funding
This research received no external funding.
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflict of interest.”
References
- Brundtland, G. Our Common Future: Report of the 1987 World Commission on Environment and Development; United Nations: Oslo, Norway, 1987; pp. 1–59. [Google Scholar]
- Komiyama, H.; Takeuchi, K. Sustainability science: Building a new discipline. Sustain. Sci. 2006, 1, 1–6. [Google Scholar] [CrossRef]
- Pearce, D.W.; Markandya, A.; Barbier, E.B. Blueprint for a Green Economy; Earthscan: London, UK, 1989. [Google Scholar]
- Burger, P. Why any substantial definition of sustainability must fail–and why this is a good, not a bad story. In Proceedings of the 12th Annual International Sustainable Development Research Conference, Hong Kong, China, 6–8 April 2006. [Google Scholar]
- Armitage, D.R.; Plummer, R.; Berkes, F.; Arthur, R.I.; Charles, A.T.; Davidson-Hunt, I.J.; McConney, P. Adaptive co-management for social–ecological complexity. Front. Ecol. Environ. 2009, 7, 95–102. [Google Scholar] [CrossRef]
- Byrne, D. Complexity Theory and the Social Sciences: An Introduction; Routledge: London, UK, 2002. [Google Scholar]
- Barth, M.; Michelsen, G. Learning for change: An educational contribution to sustainability science. Sustain. Sci. 2013, 8, 103–119. [Google Scholar] [CrossRef]
- Bogdanov, A.A. Theory of Organization, or Tektology, 1996 ed.; Dudley P. Centre for: Castlegate, UK, 1913. [Google Scholar]
- Von Bertalanffy, L. General System Theory; Wiley: New York, NY, USA, 1968. [Google Scholar]
- Golinelli, G.M. Viable Systems Approach (VSA): Governing Business Dynamics; Cedam: Padova, Italy, 2010. [Google Scholar]
- Barile, S.; Saviano, M. Foundations of Systems Thinking: The Structure-System Paradigm. In Various Authors, Contributions to Theoretical and Practical Advances in Management. A Viable Systems Approach (VSA). ASVSA, Associazione per la Ricerca sui Sistemi Vitali; International Printing: Avellino, Italy, 2011; pp. 1–24. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2044579 (accessed on 21 December 2018).
- Saviano, M.; Barile, S.; Spohrer, J.C.; Caputo, F. A service research contribution to the global challenge of sustainability. J. Serv. Theory Pract. 2017, 27, 951–976. [Google Scholar] [CrossRef]
- Palumbo, R. The Bright Side and the Dark Side of Patient Empowerment: Co-Creation and Co-Destruction of Value in the Healthcare Environment; Springer: London, UK, 2017. [Google Scholar]
- Nota, G.; Aiello, R. The interaction type approach to relationships management. J. Ambient Intell. Hum. Comput. 2017, 1–15. [Google Scholar] [CrossRef]
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Shekelle, P.G. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Ann. Internal Med. 2006, 144, 742–752. [Google Scholar] [CrossRef]
- Seiffert, M.E.B.; Loch, C. Systemic thinking in environmental management: Support for sustainable development. J. Clean. Prod. 2005, 13, 1197–1202. [Google Scholar] [CrossRef]
- Valente, T.W. Network interventions. Science 2012, 337, 49–53. [Google Scholar] [CrossRef]
- Begun, J.W.; Zimmerman, B.; Dooley, K. Health care organizations as complex adaptive systems. Adv. Health Care Organ. Theory 2003, 253, 288. [Google Scholar]
- World Health Organization (WHO). The World Health Report 2000. Health Systems: Improving Performance; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Navarro-Espigares, J.L.; Martín-Segura, J.A.; Hernández-Torres, E. The role of the service sector in regional economic resilience. Serv. Ind. J. 2012, 32, 571–590. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, I.; Serafeim, G. The Consequences of Mandatory Corporate Sustainability Reporting; Harvard Business School Research, Working Paper No. 11-100; Harvard Business School Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Christopher, W.F. Holistic Management: Managing What Matters for Company Success; John Wiley & Sons: New York, NY, USA, 2007; Volume 46. [Google Scholar]
- Espinosa, A.; Porter, T. Sustainability, complexity and learning: Insights from complex systems approaches. Learn. Organ. 2011, 18, 54–72. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M. Complexity and sustainability in management: Insights from a systems perspective. In Social Dynamics in a Systems Perspective; Springer: Cham, Switzerland, 2018; pp. 39–63. [Google Scholar]
- Fiksel, J. Sustainability and resilience: Toward a systems approach. Sustain. Sci. Pract. Policy 2006, 2, 14–21. [Google Scholar] [CrossRef]
- Beer, S. Brain of the Firm: A Development in Management Cybernetics; Herder and Herder: New York, NY, USA, 1972. [Google Scholar]
- Aquino, R.P.; Barile, S.; Grasso, A.; Saviano, M. Envisioning smart and sustainable healthcare: 3D Printing technologies for personalized medication. Futures 2018. [Google Scholar] [CrossRef]
- Golinelli, G.M.; Gatti, M. The Firm as a Viable System. Symphonya Emerg. Issue Mang 2001, 2, 38–63. [Google Scholar] [CrossRef]
- Barile, S.; Lusch, R.; Reynoso, J.; Saviano, M.; Spohrer, J. Systems, networks, and ecosystems in service research. J. Serv. Manag. 2016, 27, 652–674. [Google Scholar] [CrossRef]
- IFM, IBM. Succeeding Through Service Innovation: A Service Perspective for Education, Research, Business and Government; University of Cambridge Institute for Manufacturing: Cambridge, UK, 2008. [Google Scholar]
- Reynoso, J.; Barile, S.; Saviano, M.; Spohrer, J. Service Systems, Networks, and Ecosystems: Connecting the Dots Concisely from a Systems Perspective1; The SAGE Handbook of Service-Dominant Logic; SAGE: Thousand Oaks, CA, USA, 2018; p. 241. [Google Scholar]
- Polese, F.; Capunzo, M. The determinants of translational medicine success—A managerial contribution. Transl. Med. 2013, 6, 29. [Google Scholar]
- Saviano, M.; Bassano, C.; Calabrese, M. A VSA-SS approach to healthcare service systems the triple target of efficiency, effectiveness and sustainability. Serv. Sci. 2010, 2, 41–61. [Google Scholar] [CrossRef]
- Lipsitz, L.A. Understanding health care as a complex system: The foundation for unintended consequences. JAMA 2012, 308, 243–244. [Google Scholar] [CrossRef]
- Oudshoorn, A. Client-Provider Relationships in a Community Health Clinic for People Experiencing Homelessness: A Critical Ethnography. Ph.D. Thesis, University of Western Ontario, London, ON, Canada, 2011; p. 107. [Google Scholar]
- Rathert, C.; Wyrwich, M.D.; Boren, S.A. Patient-centered care and outcomes: A systematic review of the literature. Med. Care Res. Rev. 2013, 70, 351–379. [Google Scholar] [CrossRef]
- Prigge, J.K.; Dietz, B.; Homburg, C.; Hoyer, W.D.; Burton, J.L. Patient empowerment: A cross-disease exploration of antecedents and consequences. Int. J. Res. Mark. 2015, 32, 375–386. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M.; Polese, F. Information asymmetry and co-creation in health care services. AMJ 2014, 22, 205–217. [Google Scholar] [CrossRef]
- Naaranoja, M.; Uden, L. Why Co-creation of Value May Not Work? In International Conference on Knowledge Management in Organizations; Springer: Cham, Switzerland, 2014; pp. 362–372. [Google Scholar]
- Polese, F.; Mele, C.; Gummesson, E. Value co-creation as a complex adaptive process. J. Serv. Theory Pract. 2017, 27, 926–929. [Google Scholar] [CrossRef]
- Carlsson, L.; Berkes, F. Co-management: Concepts and methodological implications. J. Environ. Manag. 2005, 75, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Caputo, F.; Buhnova, B.; Walletzký, L. Investigating the role of smartness for sustainability: Insights from the Smart Grid domain. Sustain. Sci. 2018, 1–11. [Google Scholar] [CrossRef]
- Berry, L.L.; Bendapudi, N. Health care: A fertile field for service research. J. Serv. Res. 2007, 10, 111–122. [Google Scholar] [CrossRef]
- Holmes, M.V.; Shah, T.; Vickery, C.; Smeeth, L.; Hingorani, A.D.; Casas, J.P. Fulfilling the promise of personalized medicine? Systematic review and field synopsis of pharmacogenetic studies. PLoS ONE 2009, 4, e7960. [Google Scholar] [CrossRef] [PubMed]
- Walczak, M. Models of the emergence and diffusion of mass customization. Procedia Soc. Behav. Sci. 2014, 110, 812–821. [Google Scholar]
- Skinner, R.I. The value of information technology in healthcare/reply. Front. Health Serv. Manag. 2003, 19, 3–15. [Google Scholar] [CrossRef]
- Realpe, A.; Wallace, L.M. What Is Co-Production; The Health Foundation: London, UK, 2010; pp. 1–11. [Google Scholar]
- Grunwald, A. Technology Assessment and Policy Advice in the Field of Sustainable Development. In Technology, Society and Sustainability; Springer: Cham, Switzerland, 2017; pp. 203–221. [Google Scholar]
- Spohrer, J.; Maglio, P.P.; Bailey, J.; Gruhl, D. Steps toward a science of service systems. Computer 2007, 40. [Google Scholar] [CrossRef]
- Rumbaugh, J.; Jacobson, I.; Booch, G. Unified Modeling Language Reference Manual; Pearson Higher Education: New York, NY, USA, 2004. [Google Scholar]
- Barile, S.; Polese, F. Smart service systems and viable service systems: Applying systems theory to service science. Serv. Sci. 2010, 2, 21–40. [Google Scholar] [CrossRef]
- Breidbach, C.F.; Maglio, P.P. Technology-enabled value co-creation: An empirical analysis of actors, resources, and practices. Ind. Mark. Manag. 2016, 56, 73–85. [Google Scholar] [CrossRef]
- Lusch, R.F.; Nambisan, S. Service innovation: A service-dominant logic perspective. MIS Q. 2015, 39, 155–176. [Google Scholar] [CrossRef]
- Yoo, Y.; Boland, R.J., Jr.; Lyytinen, K.; Majchrzak, A. Organizing for innovation in the digitized world. Organ. Sci. 2012, 23, 1398–1408. [Google Scholar] [CrossRef]
- Beirão da Veiga, L.; Brezzi, F.; Marini, L.D.; Russo, A. Virtual element method for general second-order elliptic problems on polygonal meshes. Math. Models Meth. Appl. Sci. 2016, 26, 729–750. [Google Scholar] [CrossRef]
- Barrett, M.; Davidson, E.; Prabhu, J.; Vargo, S.L. Service innovation in the digital age: Key contributions and future directions. MIS Q. 2015, 39, 135–154. [Google Scholar] [CrossRef]
- Patrício, L.; de Pinho, N.F.; Teixeira, J.G.; Fisk, R.P. Service Design for Value Networks: Enabling Value Cocreation Interactions in Healthcare. Serv. Sci. 2018, 10, 76–97. [Google Scholar] [CrossRef]
- Vargo, S.L.; Maglio, P.P.; Akaka, M.A. On value and value co-creation: A service systems and service logic perspective. Eur. Mang. J. 2008, 26, 145–152. [Google Scholar] [CrossRef]
- Kongstvedt, P.R. (Ed.) The Managed Health Care Handbook; Jones & Bartlett Learning: London, UK, 2001. [Google Scholar]
- Storbacka, K.; Brodie, R.J.; Böhmann, T.; Maglio, P.P.; Nenonen, S. Actor engagement as a micro foundation for value co-creation. J. Bus. Res. 2016, 69, 3008–3017. [Google Scholar] [CrossRef]
- Palumbo, R.; Cosimato, S.; Tommasetti, A. Dream or reality? A recipe for sustainable and innovative health care ecosystems. TQM J. 2017, 29, 847–862. [Google Scholar] [CrossRef]
Figure 1.
Structure and behaviour of a relationship (unified modelling language (UML) class diagram).
Figure 1.
Structure and behaviour of a relationship (unified modelling language (UML) class diagram).

Figure 2.
The top-level architecture of DocBox24.

Figure 3.
(a) Implementation of the interaction type “Electronic Health Record2” (data that a doctor manages) and (b) visualization of a trend of measures.
Figure 3.
(a) Implementation of the interaction type “Electronic Health Record2” (data that a doctor manages) and (b) visualization of a trend of measures.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Examples of health-related aggregate interaction types.
| Aggregate Interaction Types | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Set of Interaction Types | Constraint | Initiator |
| patient-doctor | medical examination | solve a health problem | appointment booking take a physical medical report payment | select all | patient |
| patient-analysis centre | clinical analysis | to get clinical examination | appointment booking payment clinical examination clinical report | select all | patient |
| hospital-family | vaccination | vaccination campaign | call for vaccination make a vaccine | a family member is responsible for the hospital-family relationship, select all | hospital |
| doctor1-doctor2 | consultation | to get an appointment for a further specialist examination | appointment booking clinical history clinical examination clinical report | select all | doctor 1 |
Table 2.
Simple interaction types for structuring the aggregate “medical examination” and information sharing between patients.
Table 2.
Simple interaction types for structuring the aggregate “medical examination” and information sharing between patients.
| Simple Interaction Types | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Message | Constraint | Initiator |
| patient-doctor | appointment booking | to get an appointment | message for appointment request | to be in touch | patient |
| patient-doctor | symptoms | to describe the health status | message for the description of symptoms | to be in touch | patient |
| patient-doctor | medical report | to produce a medical report for the patient | message that describes the health problem and the therapeutic plan | to be in touch | doctor |
| patien1-patient2 | information sharing | provide mutual assistance to face everyday diseases problems | message with experience sharing | patien1 and patient2 wish to share information | patient1 or patient2 |
| doctor-Department of Health | data transmission | sending data about the provided treatments | data sending | select all | doctor |
Table 3.
Simple interaction types for the management of an electronic health record (her) by the active entities patient and doctor.
Table 3.
Simple interaction types for the management of an electronic health record (her) by the active entities patient and doctor.
| Simple Interaction Types for the Management of an EHR in a Cloud Environment | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Message | Constraint | Initiator |
| patient-DocBox24 | Electronic Health Record1 | The patient manages his online health data and medical reports | data to manage the EHR | the patient is connected to DocBox24 | patient |
| doctor-DocBox24 | Electronic Health Record2 | The doctor manages online data and medical reports for his patients | data to manage the patient EHR | the doctor is connected to DocBox24 | doctor |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Faggini, M.; Cosimato, S.; Nota, F.D.; Nota, G. Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability 2019, 11, 165. https://doi.org/10.3390/su11010165
AMA Style
Faggini M, Cosimato S, Nota FD, Nota G. Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability. 2019; 11(1):165. https://doi.org/10.3390/su11010165
Chicago/Turabian StyleFaggini, Marisa, Silvia Cosimato, Francesco David Nota, and Giancarlo Nota. 2019. "Pursuing Sustainability for Healthcare through Digital Platforms" Sustainability 11, no. 1: 165. https://doi.org/10.3390/su11010165
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.