Maternal Exposure to Ambient Air Pollution and Pregnancy Complications in Victoria, Australia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.1.1. The Study Population
2.1.2. Outcome Assessment
2.1.3. Exposure Data
2.1.4. Weather and Other Covariates
2.1.5. Confounding
2.2. Statistical Analysis
3. Results
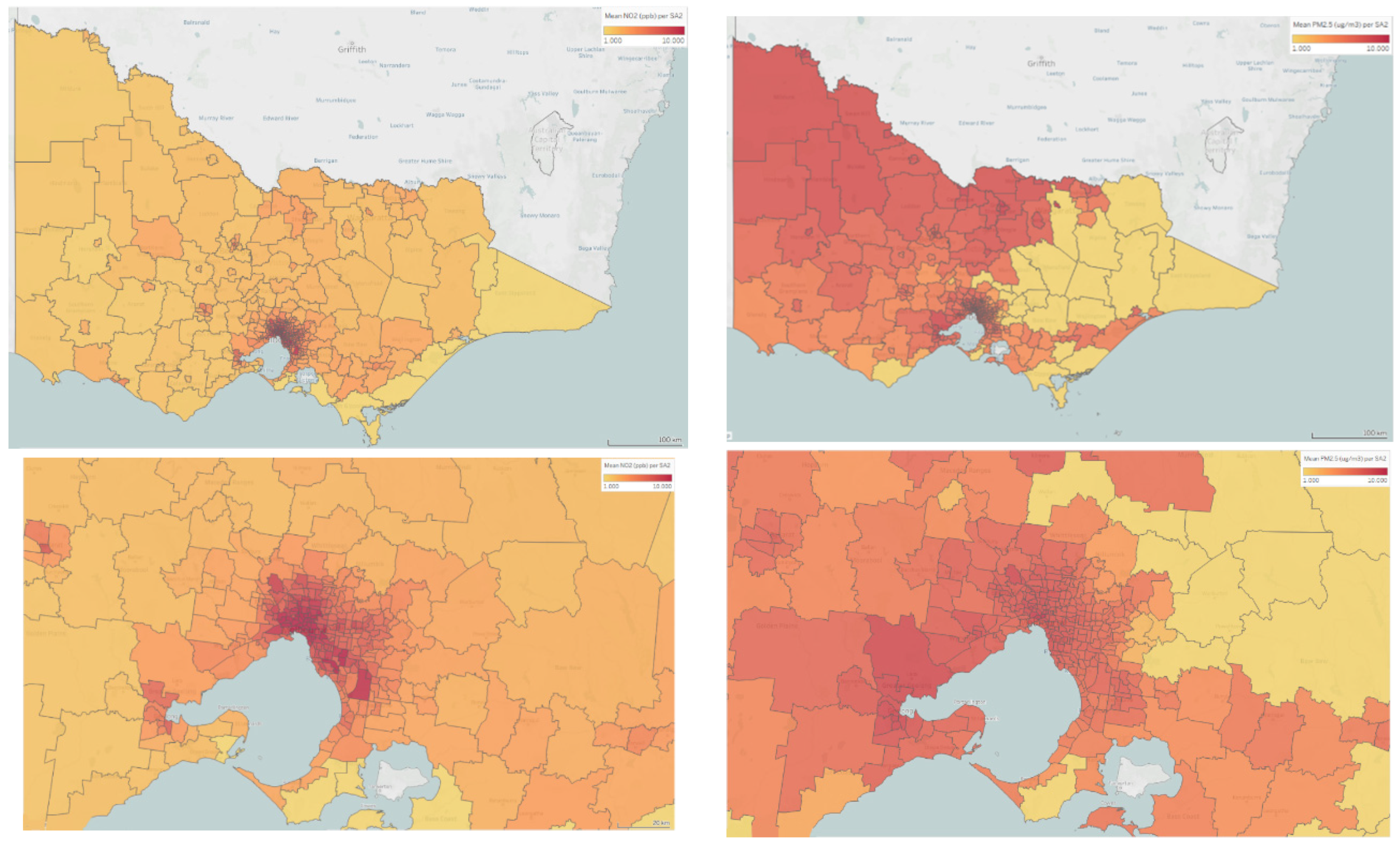
3.1. Exposure to Ambient Air Pollution
3.2. Association Between Ambient NO2 and PM2.5 and Pregnancy Conditions
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Huang, S.; Jiao, A.; Yang, X.; Yun, J.; Wang, Y.; Xue, X.; Chu, Y.; Liu, F.; Liu, Y.; et al. Association between ambient fine particulate matter and preterm birth or term low birth weight: An updated systematic review and meta-analysis. Environ. Pollut. 2017, 227, 596–605. [Google Scholar] [CrossRef] [PubMed]
- De Melo, J.O.; Soto, S.F.; Katayama, I.A.; Wenceslau, C.F.; Pires, A.G.; Veras, M.M.; Furukawa, L.N.; de Castro, I.; Saldiva, P.H.N.; Heimann, J.C. Inhalation of fine particulate matter during pregnancy increased IL-4 cytokine levels in the fetal portion of the placenta. Toxicol. Lett. 2015, 232, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Bové, H.; Bongaerts, E.; Slenders, E.; Bijnens, E.M.; Saenen, N.D.; Gyselaers, W.; Van Eyken, P.; Plusquin, M.; Roeffaers, M.B.; Ameloot, M.; et al. Ambient black carbon particles reach the fetal side of human placenta. Nat. Commun. 2019, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Van den Hooven, E.H.; Pierik, F.H.; de Kluizenaar, Y.; Hofman, A.; van Ratingen, S.W.; Zandveld, P.Y.J.; Russcher, H.; Lindemans, J.; Miedema, H.M.; Steegers, E.A.; et al. Air Pollution Exposure and Markers of Placental Growth and Function: The Generation R Study. Environ. Health Perspect. 2012, 120, 1753–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steegers, E.A.; Von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-eclampsia. Lancet 2010, 376, 631–644. [Google Scholar] [CrossRef]
- Martis, R.; Crowther, C.A.; Shepherd, E.; Alsweiler, J.; Downie, M.R.; Brown, J. Treatments for women with gestational diabetes mellitus: An overview of Cochrane systematic reviews. Cochr. Database Syst. Rev. 2018, 8. [Google Scholar] [CrossRef]
- Tikkanen, M. Placental abruption: Epidemiology, risk factors and consequences. Acta Obstet. Gynecol. Scand. 2011, 90, 140–149. [Google Scholar] [CrossRef]
- Pedersen, M.; Stayner, L.; Slama, R.; Sorensen, M.; Figueras, F.; Nieuwenhuijsen, M.J.; Raaschou-Nielsen, O.; Dadvand, P. Ambient Air Pollution and Pregnancy-Induced Hypertensive Disorders A Systematic Review and Meta-Analysis. Hypertension 2014, 64, 494. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.-Y.; Gao, X.; Fang, Y.; Jiang, W.; Huang, K.; Hua, X.-G.; Yang, X.J.; Chen, H.B.; Jiang, Z.X.; Zhang, X.J. Human epidemiological evidence about the association between air pollution exposure and gestational diabetes mellitus: Systematic review and meta-analysis. Environ. Res. 2019, 180, 108843. [Google Scholar] [CrossRef]
- Ibrahimou, B.; Albatineh, A.N.; Salihu, H.M.; Gasana, J. Ambient PM2.5 Aluminum and Elemental Carbon and Placental Abruption Morbidity. J. Occup. Environ. Med. 2017, 59, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Michikawa, T.; Morokuma, S.; Yamazaki, S.; Fukushima, K.; Kato, K.; Nitta, H. Air Pollutant Exposure Within a Few Days of Delivery and Placental Abruption in Japan. Epidemiology 2017, 28, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Ananth, C.V.; Kioumourtzoglou, M.-A.; Huang, Y.; Ross, Z.; Friedman, A.M.; Williams, M.A.; Wang, S.; Mittleman, M.A.; Schwartz, J. Exposures to air pollution and risk of acute-onset placental abruption: A case-crossover study. Epidemiology 2018, 29, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 2016 Census Community Profile: Victoria Canberra, Australia: Australian Bureau of Statistics. 2016. Available online: https://quickstats.censusdata.abs.gov.au/census_services/getproduct/census/2016/communityprofile/1?opendocument (accessed on 23 October 2019).
- Flood, M.M.; McDonald, S.J.; Pollock, W.E.; Davey, M.-A. Data Accuracy in the Victorian Perinatal Data Collection: Results of a validation study of 2011 data. Health Inf. Manag. J. 2017, 46, 113–126. [Google Scholar] [CrossRef]
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Diagnosis of Gestational Diabetes Mellitus: The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. July 2017. Available online: https://www.ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical-Obstetrics/Diagnosis-of-GDM-(C-Obs-7)-review-July-2017.pdf?ext=.pdf (accessed on 1 October 2018).
- Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Diagnosis of Gestational Diabetes Mellitus (GDM) in Australia. April 2016. Available online: https://www.ranzcog.edu.au/news/Diagnosis-GDM-Australia (accessed on 16 February 2020).
- Knibbs, L.D.; Hewson, M.G.; Bechle, M.J.; Marshall, J.D.; Barnett, A.G. A national satellite-based land-use regression model for air pollution exposure assessment in Australia. Environ. Res. 2014, 135, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Census of Population and Housing: Mesh Block Counts, Australia Canberra, Australia: Australian Bureau of Statistics. 2017. Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/2074.0 (accessed on 16 February 2020).
- Knibbs, L.D.; Van Donkelaar, A.; Martin, R.V.; Bechle, M.J.; Brauer, M.; Cohen, D.D.; Cowie, C.T.; Dirgawati, M.; Guo, Y.; Hanigan, I.C.; et al. Satellite-based land-use regression for continental-scale long-term ambient PM2. 5 exposure assessment in Australia. Environ. Sci. Technol. 2018, 52, 12445–12455. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. Statistical Area Level 1 (SA1); Australian Bureau of Statistics: Canberra, Australia, 2016.
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariable Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar]
- Strand, L.B.; Barnett, A.G.; Tong, S. Methodological challenges when estimating the effects of season and seasonal exposures on birth outcomes. BMC Med. Res. Method 2011, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- National Environment Protection (Ambient Air Quality) Measure. Available online: http://www.nepc.gov.au/nepms/ambient-air-quality (accessed on 23 October 2019).
- Park, S.K.; Wang, W. Ambient air pollution and type 2 diabetes mellitus: A systematic review of epidemiologic research. Curr. Environ. Health Rep. 2014, 1, 275–286. [Google Scholar] [CrossRef] [Green Version]
- Melody, S.M.; Ford, J.B.; Wills, K.; Venn, A.; Johnston, F.H. Maternal exposure to fine particulate matter from a large coal mine fire is associated with gestational diabetes mellitus: A prospective cohort study. Environ. Res. 2019, 108956. [Google Scholar] [CrossRef]
- Nachman, R.M.; Mao, G.; Zhang, X.; Hong, X.; Chen, Z.; Soria, C.S.; He, H.; Wang, G.; Caruso, D.; Pearson, C.; et al. Intrauterine Inflammation and Maternal Exposure to Ambient PM2.5 during Preconception and Specific Periods of Pregnancy: The Boston Birth Cohort. Environ. Health Persp. 2016, 124, 1608–1615. [Google Scholar] [CrossRef] [Green Version]
- Chiofalo, B.; Laganà, A.S.; Vaiarelli, A.; La Rosa, V.L.; Rossetti, D.; Palmara, V.; Valenti, G.; Rapisarda, A.M.; Granese, R.; Sapia, F.; et al. Do miRNAs play a role in fetal growth restriction? A fresh look to a busy corner. BioMed Res. Int. 2017, 2017, 6073167. [Google Scholar] [CrossRef] [PubMed]
- Sofo, V.; Götte, M.; Lagana, A.S.; Salmeri, F.M.; Triolo, O.; Sturlese, E.; Retto, G.; Alfa, M.; Granese, R.; Abrao, M.S. Correlation between dioxin and endometriosis: An epigenetic route to unravel the pathogenesis of the disease. Arch. Gynecol. Obstetr. 2015, 292, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Higashijima, A.; Miura, K.; Mishima, H.; Kinoshita, A.; Jo, O.; Abe, S.; Hasegawa, Y.; Miura, S.; Yamasaki, K.; Yoshida, A.; et al. Characterization of placenta-specific microRNAs in fetal growth restriction pregnancy. Prenat. Diagn. 2013, 33, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Resuehr, D.; Glore, D.R.; Taylor, H.S.; Bruner-Tran, K.L.; Osteen, K.G. Progesterone-dependent regulation of endometrial cannabinoid receptor type 1 (CB1-R) expression is disrupted in women with endometriosis and in isolated stromal cells exposed to 2, 3, 7, 8-tetrachlorodibenzo-p-dioxin (TCDD). Fertil. Steril. 2012, 98, 948–956.e1. [Google Scholar] [CrossRef] [Green Version]
- Bobak, M.; Leon, D.A. Pregnancy outcomes and outdoor air pollution: An ecological study in districts of the Czech Republic 1986–8. Occup. Environ. Med. 1999, 56, 539–543. [Google Scholar] [CrossRef] [Green Version]
- Van den Hooven, E.H.; Jaddoe, V.W.; de Kluizenaar, Y.; Hofman, A.; Mackenbach, J.P.; Steegers, E.A.; Miedema, H.M.; Pierik, F.H. Residential traffic exposure and pregnancy-related outcomes: A prospective birth cohort study. Environ. Health 2009, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Miranda, M.L.; Edwards, S.E.; Chang, H.H.; Auten, R.L. Proximity to roadways and pregnancy outcomes. J. Exp. Sci. Environ. Epidemiol. 2013, 23, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Bowatte, G.; Erbas, B.; Lodge, C.J.; Knibbs, L.D.; Gurrin, L.C.; Marks, G.B.; Thomas, P.S.; Johns, D.P.; Giles, G.G.; Hui, J.; et al. The Association of Long-Term Traffic-Related Air Pollution Exposure with Asthma and Poor Lung Function in Middle Age. Respirology 2017, 22, 108. [Google Scholar]
- Salimi, F.; Morgan, G.; Rolfe, M.; Samoli, E.; Cowie, C.T.; Hanigan, I.; Knibbs, L.; Cope, M.; Johnston, F.H.; Guo, Y.; et al. Long-term exposure to low concentrations of air pollutants and hospitalisation for respiratory diseases: A prospective cohort study in Australia. Environ. Int. 2018, 121, 415–420. [Google Scholar] [CrossRef]
- Knibbs, L.D.; de Waterman, A.M.; Toelle, B.G.; Guo, Y.; Denison, L.; Jalaludin, B.; Marks, G.B.; Williams, G.M. The Australian Child Health and Air Pollution Study (ACHAPS): A national population-based cross-sectional study of long-term exposure to outdoor air pollution, asthma, and lung function. Environ. Int. 2018, 120, 394–403. [Google Scholar] [CrossRef]
- Pereira, G.; Bracken, M.B.; Bell, M.L. Particulate air pollution, fetal growth and gestational length: The influence of residential mobility in pregnancy. Environ. Res. 2016, 147, 269–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Infant Characteristics | n (%) |
|---|---|
| Female gender | 138,979 (48.7) |
| Aboriginal and/or Torres Strait Islander | 4291 (1.5) |
| Admitted to special care nursery | 36,930 (12.9) |
| Admitted to neonatal intensive care unit | 3890 (1.4) |
| Liveborn | 284,332 (99.6) |
| Maternal characteristics | |
| Maternal smoking in early pregnancy (<20 weeks) | 28,283 (9.9) |
| Maternal smoking in late pregnancy (>20 weeks) | 16,340 (5.7) |
| Country of birth Australia | 183,441 (64.2) |
| Aboriginal and/or Torres Strait Islander | 3587 (1.3) |
| Resident in major capital city | 166,285 (58.2) |
| Pregnancy and labour characteristics | |
| Nulliparous | 127,501 (44.6) |
| Spontaneous onset of labour * | 101,725 (35.6) |
| Caesarean section birth | 93,121 (32.6) |
| Hypertensive disorder of pregnancy ^ | 9987 (3.5) |
| Gestational diabetes mellitus | 23,035 (8.1) |
| Placenta praevia | 1277 (0.5) |
| Placental abruption | 399 (0.1) |
| Year of birth | |
| 2012 | 62,018 (21.7) |
| 2013 | 73,909 (25.9) |
| 2014 | 74,802 (26.2) |
| 2015 | 74,865 (26.2) |
| Pregnancy Condition | Adjusted Relative Risk (95%CI); p Value | |
|---|---|---|
| Per IQR Increase in Annual Ambient NO2 Concentration (ppb) | Per IQR Increase in Annual Ambient PM2.5 Concentration (µg/m3) | |
| Hypertensive disorder of pregnancy (pregnancy-induced hypertension, preeclampsia, eclampsia) * | 0.89 (0.86, 0.91); <0.0001 | 0.95 (0.93, 0.97); <0.0001 |
| Gestational Diabetes Mellitus ** | 0.92 (0.90, 0.94); <0.0001 | 1.02 (1.00, 1.03); 0.03 |
| Placental abruption ** | 0.81 (0.69, 0.95); 0.01 | 1.06 (0.94, 1.20); 0.35 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melody, S.M.; Wills, K.; Knibbs, L.D.; Ford, J.; Venn, A.; Johnston, F. Maternal Exposure to Ambient Air Pollution and Pregnancy Complications in Victoria, Australia. Int. J. Environ. Res. Public Health 2020, 17, 2572. https://doi.org/10.3390/ijerph17072572
Melody SM, Wills K, Knibbs LD, Ford J, Venn A, Johnston F. Maternal Exposure to Ambient Air Pollution and Pregnancy Complications in Victoria, Australia. International Journal of Environmental Research and Public Health. 2020; 17(7):2572. https://doi.org/10.3390/ijerph17072572
Chicago/Turabian StyleMelody, Shannon M., Karen Wills, Luke D. Knibbs, Jane Ford, Alison Venn, and Fay Johnston. 2020. "Maternal Exposure to Ambient Air Pollution and Pregnancy Complications in Victoria, Australia" International Journal of Environmental Research and Public Health 17, no. 7: 2572. https://doi.org/10.3390/ijerph17072572