Predictive Validity of a New Instrumental Activities of Daily Living Scale for Detecting the Incidence of Functional Disability among Community-Dwelling Older Japanese Adults: A Prospective Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment of Functional Disability
2.3. Assessment of IADL
2.4. Potential Confounding Factors
2.5. Statistical Analyses
2.6. Patients and Public Involvement
3. Results
3.1. Characteristics of Participants with and without Functional Disability
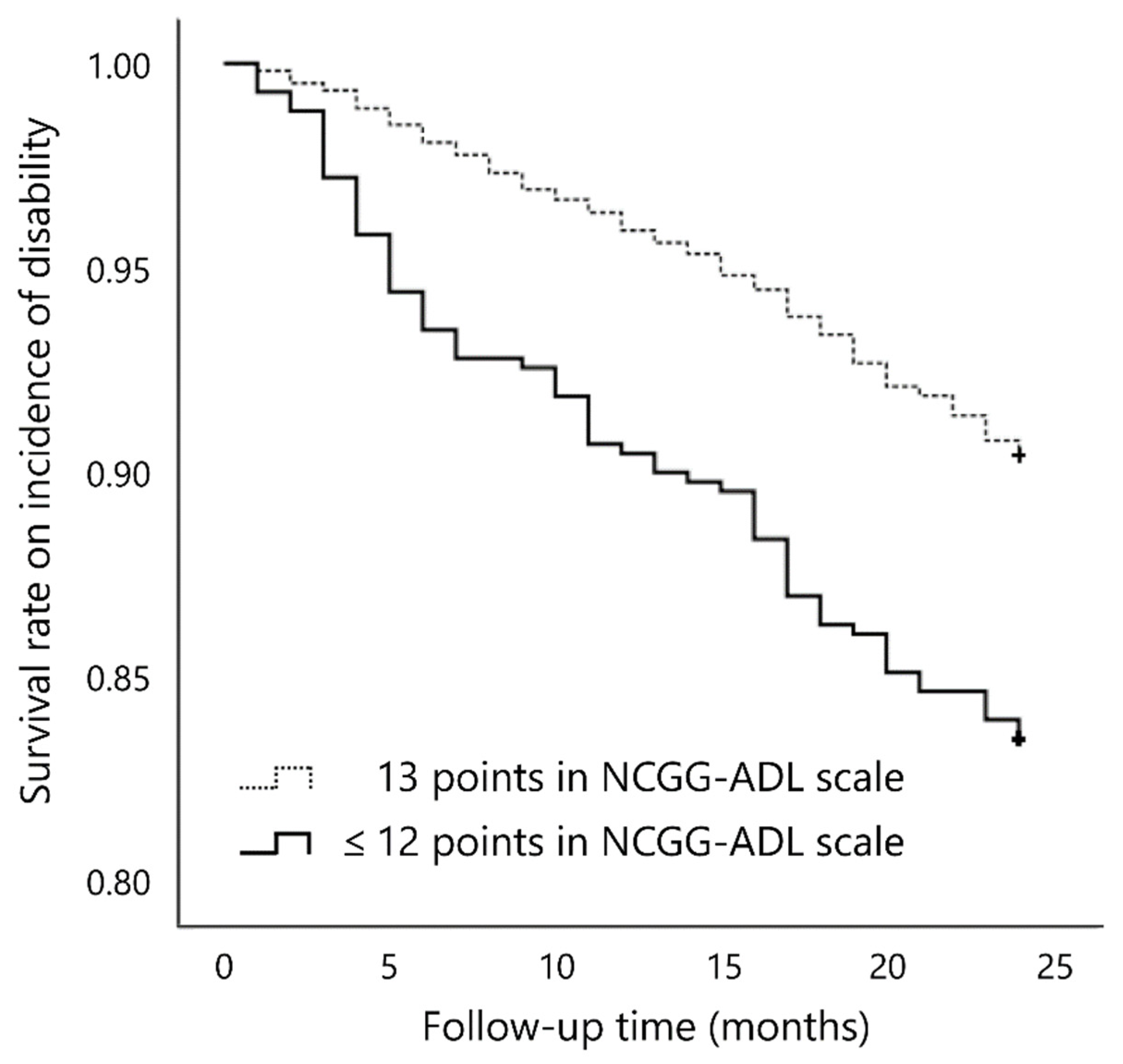
3.2. Association between Ability in IADL as Measured by the NCGG-ADL and the Incidence of Functional Disability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Institute of Population and Social Security Research. Population Projections for Japan: 2016–2065. 2017. Available online: http://www.ipss.go.jp/pp-zenkoku/j/zenkoku2017/pp29_ReportALL.pdf (accessed on 16 July 2019).
- Aida, J.; Kondo, K.; Hirai, H.; Nakade, M.; Yamamoto, T.; Hanibuchi, T.; Osaka, K.; Sheiham, A.; Watt, R.G. Association between dental status and incident disability in an older Japanese population. J. Am. Geriatr. Soc. 2012, 60, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Okochi, J. Increase of mild disability in Japanese elders: A seven year follow-up cohort study. BMC Public Health 2005, 5, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansah, J.P.; Malhotra, R.; Lew, N.; Chiu, C.T.; Chan, A.; Bayer, S.; Matchar, D.B. Projection of young-old and old-old with functional disability: Does accounting for the changing educational composition of the elderly population make a difference? PLoS ONE 2015, 10, e0126471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millán-Calenti, J.C.; Tubío, J.; Pita-Fernández, S.; González-Abraldes, I.; Lorenzo, T.; Fernández-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Judge, J.O.; Schechtman, K.; Cress, E.; FICSIT Group. The relationship between physical performance measures and independence in instrumental activities of daily living. J. Am. Geriatr. Soc. 1996, 44, 1332–1341. [Google Scholar] [CrossRef]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG Index of Competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Holbrook, M.; Skilbeck, C.E. An activities index for use with stroke patients. Age Ageing 1983, 12, 166–170. [Google Scholar] [CrossRef]
- Schuling, J.; de Haan, R.; Limburg, M.; Groenier, K.H. The Frenchay Activities Index. Assessment of functional status in stroke patients. Stroke 1993, 24, 1173–1177. [Google Scholar] [CrossRef] [Green Version]
- Nouri, F.M.; Lincoln, N.B. An extended activities of daily living scale for stroke patients. Clin. Rehabil. 1987, 1, 301–305. [Google Scholar] [CrossRef]
- Gompertz, P.; Pound, P.; Ebrahim, S. Validity of the Extended Activities of Daily Living Scale. Clin. Rehabil. 1994, 8, 275–280. [Google Scholar] [CrossRef]
- Sikkes, S.A.; de Lange-de Klerk, E.S.; Pijnenburg, Y.A. A new informant-based questionnaire for instrumental activities of daily living in dementia. Alzheimers Dement. 2012, 8, 536–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, H. A Survey on Instrumental Activities of Daily Living and Service Usage Details of Elderly Persons Requiring Personal Support. 2013. Available online: http://www.ncgg.go.jp/ncgg-kenkyu/documents/roken/rojinhokoku2_24.pdf (accessed on 16 July 2019).
- Shimada, H.; Tsutsumimoto, K.; Lee, S.; Doi, T.; Makizako, H.; Lee, S.; Harada, K.; Hotta, R.; Bae, S.; Nakakubo, S.; et al. Driving continuity in cognitively impaired older drivers. Geriatr. Gerontol. Int. 2015, 16, 508–514. [Google Scholar] [CrossRef]
- Tsutsui, T.; Muramatsu, N. Care-needs certification in the long-term care insurance system of Japan. J. Am. Geriatr. Soc. 2005, 53, 522–527. [Google Scholar] [CrossRef]
- Saito, T.; Murata, C.; Aida, J.; Kondo, K. Cohort study on living arrangements of older men and women and risk for basic activities of daily living disability: Findings from the AGES project. BMC Geriatr. 2017, 17, 183. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Williams, C.S. The effect of falls and fall injuries on functioning in community-dwelling older persons. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, M112–M119. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Suzuki, T. Cognitive impairment and disability in older Japanese adults. PLoS ONE 2016, 11, e0158720. [Google Scholar] [CrossRef]
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The Mini-Mental State Examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef]
- Kaufer, D.I.; Williams, C.S.; Braaten, A.J.; Gill, K.; Zimmerman, S.; Sloane, P.D. Cognitive screening for dementia and mild cognitive impairment in assisted living: Comparison of 3 tests. J. Am. Med. Dir. Assoc. 2008, 9, 586–593. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Hotta, R.; Nakakubo, S.; Harada, K.; Lee, S.; Bae, S.; et al. Cognitive functioning and walking speed in older adults as predictors of limitations in self-reported instrumental activity of daily living: Prospective findings from the Obu Study of Health Promotion for the Elderly. Int. J. Environ. Res. Public Health 2015, 12, 3002–3013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, A.B.; Enright, P.L.; Manolio, T.A.; Haponik, E.F.; Wahl, P.W. Sleep disturbance, psychosocial correlates, and cardiovascular disease in 5201 older adults: The Cardiovascular Health Study. J. Am. Geriatr. Soc. 1997, 45, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Dupre, M.E.; Qiu, L.; Zhou, W.; Zhao, Y.; Gu, D. Urban-rural differences in the association between access to healthcare and health outcomes among older adults in China. BMC Geriatr. 2017, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Freedman, V.A.; Martin, L.G.; Schoeni, R.F.; Cornman, J.C. Declines in late-life disability: The role of early-and mid-life factors. Soc. Sci. Med. 2008, 66, 1588–1602. [Google Scholar] [CrossRef] [Green Version]
- Makino, K.; Ihira, H.; Mizumoto, A.; Shimizu, K.; Ishida, T.; Yamaguchi, R.; Kihara, Y.; Ito, K.; Sasaki, T.; Furuna, T. Structural analysis of impact of physical, cognitive and social status on the incidence of disability in community-dwelling people aged ≥ 75 years. Geriatr. Gerontol. Int. 2018, 18, 1614–1619. [Google Scholar] [CrossRef]
- Portegijs, E.; Rantakokko, M.; Viljanen, A.; Sipilä, S.; Rantanen, T. Identification of older people at risk of ADL disability using the life-space assessment: A longitudinal cohort study. J. Am. Med. Dir. Assoc. 2016, 17, 410–414. [Google Scholar] [CrossRef] [Green Version]
- MacNeil Vroomen, J.L.; Han, L.; Monin, J.K.; Lipska, K.J.; Allore, H.G. Diabetes, heart disease, and dementia: National estimates of functional disability trajectories. J. Am. Geriatr. Soc. 2018, 66, 766–772. [Google Scholar] [CrossRef]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y.; Matsuzaki, T. Mortality in relation to instrumental activities of daily living: One-year follow-up in a Japanese urban community. J. Gerontol. 1989, 44, S107–S109. [Google Scholar] [CrossRef]
- Spector, W.D.; Katz, S.; Murphy, J.B.; Fulton, J.P. The hierarchical relationship between activities of daily living and instrumental activities of daily living. J. Chronic Dis. 1987, 40, 481–489. [Google Scholar] [CrossRef]
- Gu, D.; Gomez-Redondo, R.; Dupre, M.E. Studying disability trends in aging populations. J. Cross Cult. Gerontol. 2015, 30, 21–49. [Google Scholar] [CrossRef]
- Bryant, L.L.; Shetterly, S.M.; Baxter, J.; Hamman, R.F. Changing functional status in a biethnic rural population: The San Luis Valley Health and Aging Study. Am. J. Epidemiol. 2002, 155, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Overall (n = 2708) M (SD) | Independent (n = 2419) M (SD) | Incident Disability (n = 289) M (SD) | p | |
|---|---|---|---|---|
| Age (years) | 79.0 (3.5) | 78.8 (3.3) | 81.1 (3.9) | <0.001 |
| Body mass index (kg/m2) | 22.9 (3.0) | 23.0 (3.0) | 22.6 (3.3) | 0.053 |
| Education (years) | 11.7 (2.7) | 11.8 (2.7) | 11.4 (2.6) | 0.028 |
| MMSE (score) | 25.7 (2.5) | 25.8 (2.4) | 25.0 (2.6) | <0.001 |
| NCGG-ADL (score) | 12.7 (0.8) | 12.8 (0.7) | 12.5 (1.3) | <0.001 |
| n (%) | n (%) | n (%) | p | |
| Female | 1396 (51.6) | 1234 (51.0) | 162 (56.1) | 0.105 |
| Medical conditions: | ||||
| Hypertension | 1472 (54.4) | 1307 (54.1) | 165 (57.1) | 0.327 |
| Diabetes mellitus | 361 (13.3) | 316 (13.1) | 45 (15.6) | 0.238 |
| Heart disease | 579 (21.4) | 503 (20.9) | 76 (26.5) | 0.028 |
| Parkinson’s disease | 11 (0.4) | 9 (0.4) | 2 (0.7) | 0.419 |
| Stroke | 190 (7.0) | 165 (6.8) | 25 (8.7) | 0.254 |
| Depression | 103 (3.8) | 92 (3.8) | 11 (3.8) | 0.999 |
| Living alone | 476 (17.6) | 413 (17.1) | 63 (21.9) | 0.044 |
| Fall history | 593 (21.9) | 510 (21.1) | 83 (28.7) | 0.003 |
| Mild cognitive impairment (<28 points on the MMSE) | 1973 (72.9) | 1737 (71.8) | 236 (81.7) | <0.001 |
| IADL limitation (≤12 points on the NCGG-ADL scale) | 430 (15.9) | 359 (14.8) | 71 (24.6) | <0.001 |
| Crude Model | Adjusted Model | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| NCGG-ADL score | (points) | 0.79 | 0.73–0.86 | <0.001 | 0.84 | 0.77–0.92 | <0.001 |
| Age | (years) | 1.14 | 1.11–1.17 | <0.001 | |||
| Female | (yes) | 1.39 | 1.07–1.80 | 0.014 | |||
| Body mass index | (kg/m2) | 0.97 | 0.94–1.01 | 0.179 | |||
| Education | (years) | 1.01 | 0.97–1.06 | 0.632 | |||
| Hypertension | (yes) | 1.04 | 0.82–1.33 | 0.724 | |||
| Diabetes mellitus | (yes) | 1.21 | 0.87–1.67 | 0.259 | |||
| Heart disease | (yes) | 1.31 | 1.00–1.71 | 0.052 | |||
| Parkinson’s disease | (yes) | 1.75 | 0.43–7.07 | 0.435 | |||
| Stroke | (yes) | 1.15 | 0.76–1.75 | 0.503 | |||
| Depression | (yes) | 0.98 | 0.54–1.80 | 0.952 | |||
| Living alone | (n, %) | 0.82 | 0.61–1.11 | 0.199 | |||
| Fall history | (n, %) | 1.28 | 0.98–1.66 | 0.066 | |||
| Mild cognitive impairment | (n, %) | 1.53 | 1.12–2.08 | 0.008 | |||
| Crude Model | Adjusted Model | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| NCGG-ADL scale | |||||||
| 13 points | Reference | Reference | |||||
| ≤12 points | 1.82 | 1.39–2.38 | <0.001 | 1.58 | 1.19–2.09 | 0.002 | |
| Age | (years) | 1.14 | 1.11–1.18 | <0.001 | |||
| Female | (yes) | 1.42 | 1.10–1.85 | 0.008 | |||
| Body mass index | (kg/m2) | 0.97 | 0.93–1.01 | 0.150 | |||
| Education | (years) | 1.01 | 0.97–1.06 | 0.573 | |||
| Hypertension | (yes) | 1.06 | 0.83–1.35 | 0.667 | |||
| Diabetes mellitus | (yes) | 1.24 | 0.90–1.71 | 0.197 | |||
| Heart disease | (yes) | 1.29 | 0.99–1.69 | 0.061 | |||
| Parkinson’s disease | (yes) | 1.73 | 0.43–7.01 | 0.442 | |||
| Stroke | (yes) | 1.17 | 0.78–1.78 | 0.447 | |||
| Depression | (yes) | 0.96 | 0.53–1.77 | 0.907 | |||
| Living alone | (n, %) | 0.82 | 0.61–1.11 | 0.201 | |||
| Fall history | (n, %) | 1.26 | 0.97–1.64 | 0.081 | |||
| Mild cognitive impairment | (n, %) | 1.54 | 1.12–2.10 | 0.007 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makino, K.; Lee, S.; Bae, S.; Shinkai, Y.; Chiba, I.; Shimada, H. Predictive Validity of a New Instrumental Activities of Daily Living Scale for Detecting the Incidence of Functional Disability among Community-Dwelling Older Japanese Adults: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 2291. https://doi.org/10.3390/ijerph17072291
Makino K, Lee S, Bae S, Shinkai Y, Chiba I, Shimada H. Predictive Validity of a New Instrumental Activities of Daily Living Scale for Detecting the Incidence of Functional Disability among Community-Dwelling Older Japanese Adults: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(7):2291. https://doi.org/10.3390/ijerph17072291
Chicago/Turabian StyleMakino, Keitaro, Sangyoon Lee, Seongryu Bae, Yohei Shinkai, Ippei Chiba, and Hiroyuki Shimada. 2020. "Predictive Validity of a New Instrumental Activities of Daily Living Scale for Detecting the Incidence of Functional Disability among Community-Dwelling Older Japanese Adults: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 7: 2291. https://doi.org/10.3390/ijerph17072291