Health-Related Rehabilitation after the 2008 Great Wenchuan Earthquake in China: A Ten Year Retrospective Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. The Search Strategy
2.4. The Data Abstraction Process
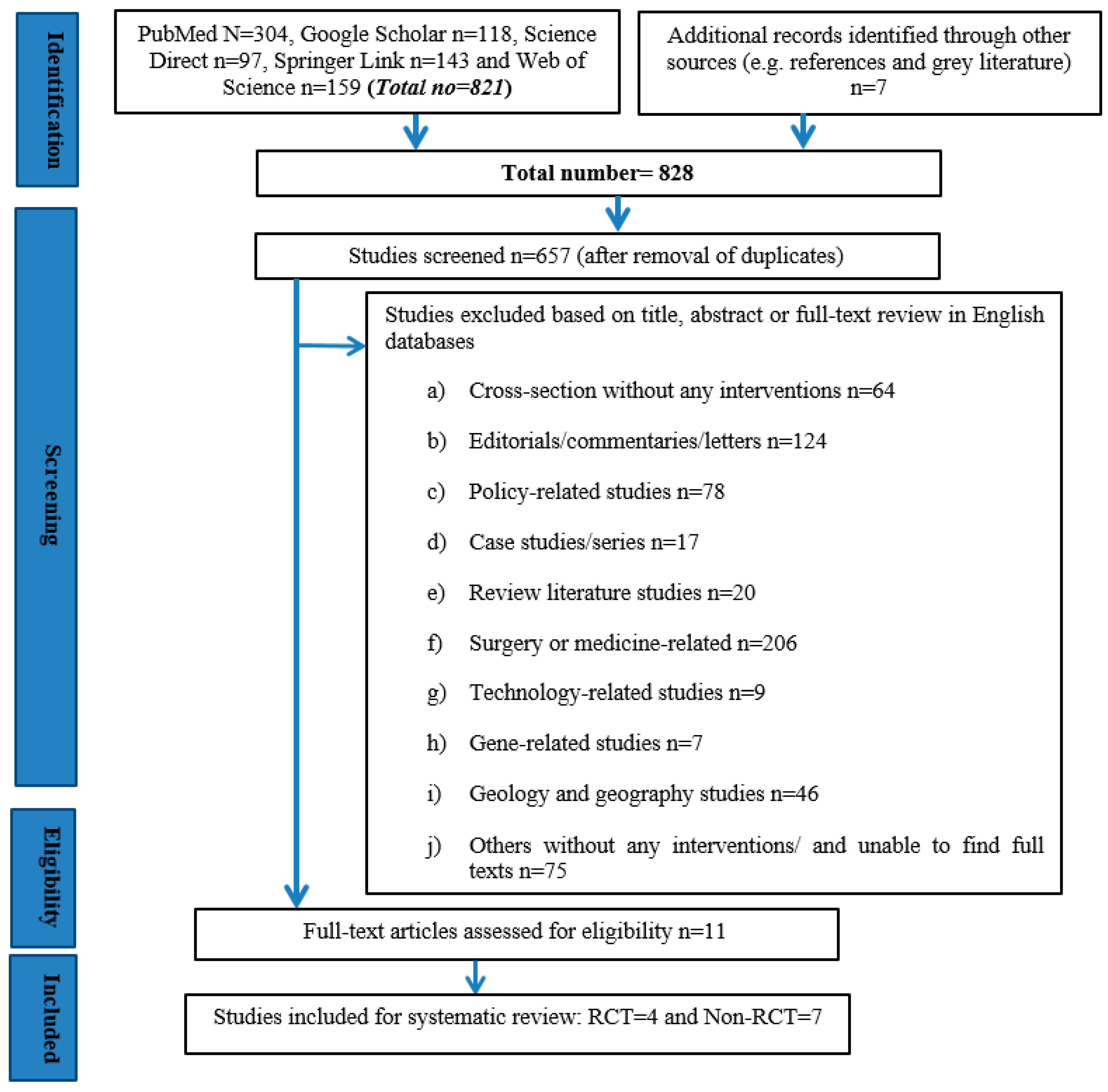
2.5. Screening and Study Selection
2.6. Quality Assessment
3. Results
3.1. Search Results
3.2. Characteristics of Participants
3.3. Mean Age and Gender
3.4. Study Designs
3.5. Interventions and Settings
3.6. HRR Outcomes
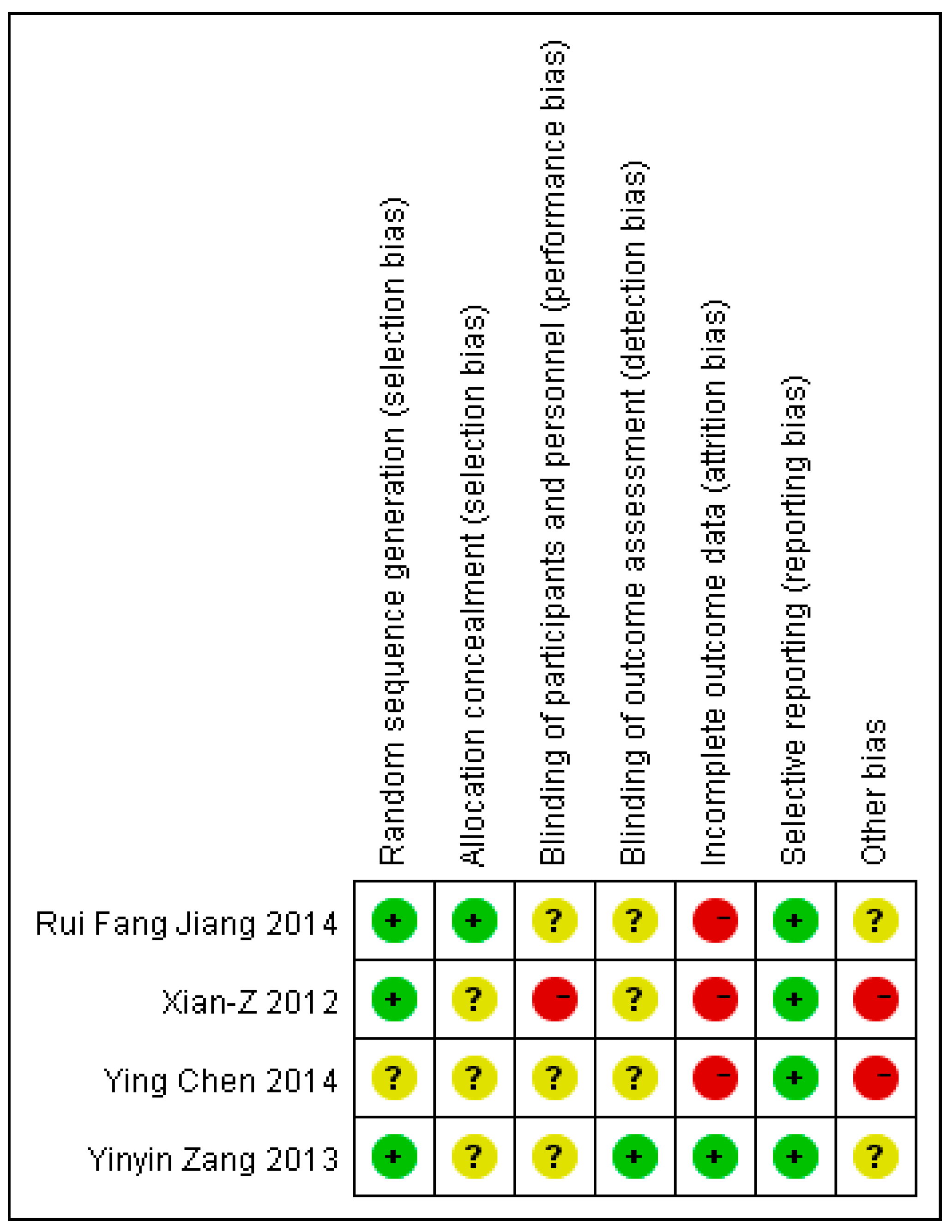
3.7. Quality Assessment and the Risk of Bias
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sim, T.; Jun, L.Y. Natural Hazards Governance in China. In Oxford Research Encyclopedia of Natural Hazard Science; Oxford University Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Gao, Y.; Griffiths, M.S. Literature review of health impact post-earthquakes in China 1906–2007. J. Public Health 2009, 32, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Wu, J.; He, X.; Ye, M.; Liu, W.; Tang, R. Emerging Trends and New Developments in Disaster Research after the 2008 Wenchuan Earthquake. Int. J. Environ. Res. Public Health 2019, 16, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Chen, J.; Liu, H.; Zheng, J. Comparison of two large earthquakes in China: The 2008 Sichuan Wenchuan Earthquake and the 2013 Sichuan Lushan Earthquake. Nat. Hazards 2014, 73, 1127–1136. [Google Scholar] [CrossRef] [Green Version]
- Han, W.; Liang, C.; Jiang, B.; Ma, W.; Zhang, Y. Major Natural Disasters in China, 1985–2014: Occurrence and Damages. Int. J. Environ. Res. Public Health 2016, 13, 1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guha-Sapir, D. The Emergency Events Database in The Emergency Events Database EM-DAT; Universite Catholique de Louvain (UCL), CRED: Brussels, Belgium, 2019. [Google Scholar]
- Zhou, Y.; Liu, Y.; Wu, W.; Li, N. Integrated risk assessment of multi-hazards in China. Nat. Hazards 2015, 78, 257–280. [Google Scholar] [CrossRef]
- Balikuddembe, J.K.; Sinclair, P. Uganda at Glance of 5.7 Magnitude Earthquake: Lessons for Earthquake Risk Reduction. PLoS Curr. 2018, 10. [Google Scholar] [CrossRef]
- Lu-Ping, Z.; Manuel Rodriguez-Llanes, M.J.; Qi, W.; van den Oever, B.; Westman, L.; Albela, M.; Liang, P.; Gao, C.; De-Sheng, Z.; Hughes, M.; et al. Multiple injuries after earthquakes: A retrospective analysis on 1,871 injured patients from the 2008 Wenchuan earthquake. Crit. Care 2012, 16, R87. [Google Scholar] [CrossRef] [Green Version]
- Chan, E.Y. The untold stories of the Sichuan earthquake. Lancet 2008, 372, 359–362. [Google Scholar] [CrossRef]
- Tang, B.; Chen, Q.; Chen, X.; Glik, D.; Liu, X.; Liu, Y.; Zhang, L. Earthquake-related injuries among survivors: A systematic review and quantitative synthesis of the literature. Int. J. Disaster Risk Reduct. 2017, 21, 159–167. [Google Scholar] [CrossRef]
- Dai, W.; Chen, L.; Lai, Z.; Li, Y.; Wang, J.; Liu, A. The incidence of post-traumatic stress disorder among survivors after earthquakes:a systematic review and meta-analysis. BMC Psychiatry 2016, 16, 188. [Google Scholar] [CrossRef] [Green Version]
- Beaglehole, B.; Mulder, R.T.; Boden, J.M.; Bell, C.J. A systematic review of the psychological impacts of the Canterbury earthquakes on mental health. Aust. N. Z. J. Public Health 2019, 43, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Yiming, L.; Jin, C.; Ruzek, J.I.; Zhengkui, L. Posttraumatic stress disorder following the 2008 Wenchuan earthquake: A 10-year systematic review among highly exposed populations in China. J. Affect. Disord. 2019, 243, 327–339. [Google Scholar]
- Hong, C.; Efferth, T. Systematic Review on Post-Traumatic Stress Disorder Among Survivors of the Wenchuan Earthquake. Trauma Violence Abus. 2016, 17, 542–561. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Reinhardt, J.D.; Gosney, J.E.; Li, J. The NHV Rehabilitation Services Program Improves Long-Term Physical Functioning in Survivors of the 2008 Sichuan Earthquake: A Longitudinal Quasi Experiment. PLoS ONE 2013, 8, e53995. [Google Scholar] [CrossRef]
- Ni, J.; Reinhardt, D.J.; Zhang, X.; Xiao, M.; Ling, L.; Jin, H.; Zeng, X.; Jianan, L. Dysfunction and Post-Traumatic Stress Disorder in Fracture Victims 50 Months after the Sichuan Earthquake. PLoS ONE 2013, 8, e77535. [Google Scholar] [CrossRef]
- Jones, C.E.; Faas, A.J. Social Network Analysis Focused on Individuals Facing Hazards and Disasters. In Social Network Analysis of Disaster Response, Recovery, and Adaptation; Jones, C.E., Faas, A.J., Eds.; Butterworth-Heineman (Elsevier): Kidlington, Oxford, UK, 2017. [Google Scholar]
- Li, Y.; Reinhardt, J.D.; Gosney, J.E.; Zhang, X.; Hu, X.; Chen, S.; Ding, M.; Li, J. Evaluation of functional outcomes of physical rehabilitation and medical complications in spinal cord injury victims of the Sichuan earthquake. J. Rehabil. Med. 2012, 44, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Reinhardt, J.D.; Zhang, X.; Pennycott, A.; Zhao, Z.; Zeng, X.; Li, J. Physical function, pain, quality of life and life satisfaction of amputees from the 2008 Sichuan earthquake: A prospective cohort study. J. Rehabil. Med. 2015, 47, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Alexander, D. Disability and disaster: An Overview. In Disability and Disaster; Kelman, I., Stough, L.M., Eds.; Palgrave Macmillan: London, UK, 2015; pp. 384–394. [Google Scholar]
- World Health Organization (WHO). World Report on Disability; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization (WHO). Concept Paper: WHO Guidelines on Health-Related Rehabilitation (Rehabilitation Guidelines); WHO: Geneva, Switzerland, 2012. [Google Scholar]
- United Nations (UN). Universal Declaration of Human Rights; UN: New York, NY, USA, 1948. [Google Scholar]
- World Health Organization (WHO). Rehabilitation 2030: A Call for Action; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization (WHO). WHO). WHO Global Disability Action Plan 2014–2021. In Better Health for All People With Disabilities; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- United Nations (UN). United Nations Convention on the Rights of People with Disabilities (UNCRD); UN: New York, NY, USA, 2008. [Google Scholar]
- Balikuddembe, K.J.; Reinhardt, D.J. Can Digitization of Healthcare help Low-Resourced Countries Provide Better Community-Based Rehabilitation Services? Phys. Ther. 2019, 100, 217–224. [Google Scholar]
- United Nations International Strategy for Disaster Reduction (UNISDR). Sendai Framework for Disaster Risk Reduction 2015–2030; The United Nations Office for Disaster Risk Reduction: Geneva, Switzerland, 2015. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 511, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Sayers, A. Tips and tricks in performing a systematic review. Br. J. Gen. Pract. 2007, 57, 999. [Google Scholar] [CrossRef]
- Eriksen, B.M.; Frandsen, F.T. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernán, A.M.; Higgins, J.P.; Reeves, B.C.; Savović, J.; Berkman, D.N.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, T.M.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.Z.; Wu, F.; Wei, K.P.; Xiu, J.L.; Shi, J.; Pang, B.; Sun, D.Z.; Qin, F.Z.; Huang, Y.; Lao, L. A Chinese Herbal Formula to Improve General Psychological Status in Posttraumatic Stress Disorder: A Randomized Placebo-Controlled Trial on Sichuan Earthquake Survivors. Evid. Based Complement Altern. Med. 2012, 2012, 691258. [Google Scholar] [CrossRef]
- Zang, Y.; Hunt, N.; Cox, T. A randomized controlled pilot study: The effectiveness of narrative exposure therapy with adult survivors of the Sichuan earthquake. BMC Psychiatry 2013, 13, 41. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Wang, R.; Kao, H.S.; Zong, Y.; Liu, Z.; Tang, S.; Xu, M.; Liu, I.C.; Lam, S.P. Effect of calligraphy training on hyperarousal symptoms for childhood survivors of the 2008 China earthquakes. Neuropsychiatr. Dis. Treat. 2014, 10, 977–985. [Google Scholar]
- Chen, Y.; Shen, W.W.; Gao, K.; Lam, C.S.; Chang, W.C.; Deng, H. Effectiveness RCT of a CBT Intervention for Youths Who Lost Parents in the Sichuan, China, Earthquake. Phychiatric Serv. 2014, 2, 259–262. [Google Scholar] [CrossRef]
- Jiang, R.F.; Tong, H.Q.; Delucchi, K.L.; Neylan, T.C.; Shi, Q.; Meffert, S.M. Interpersonal psychotherapy versus treatment as usual for PTSD and depression among Sichuan earthquake survivors: A randomized clinical trial. Confl. Health 2014, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Li, W.S.; Chan, S.Y.; Chau, W.W.; Law, S.W.; Chan, K.M. Mobility, prosthesis use and health-related quality of life of bilateral lower limb amputees from the 2008 Sichuan earthquake. Prosthet. Orthot. Int. 2019, 43, 104–111. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Maercker, A. Program Use and Outcome Change in a Web-Based Trauma Intervention: Individual and Social Factors. J. Med. Internet Res. 2016, 18, e243. [Google Scholar] [CrossRef] [Green Version]
- Stucki, G.; Cieza, A.; Melvin, J. The International Classification of Functioning, Disability and Health: A unifying model for the conceptual description of the rehabilitation strategy. J. Rehabil. Med. 2007, 39, 279–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.P.; Macedo, T.F.; Coutinho, E.S.F.; Figueira, I.; Ventura, P.R. Systematic Review of the Efficacy of Cognitive-Behavior Therapy Related Treatments for Victims of Natural Disasters: A Worldwide Problem. PLoS ONE 2014, 9, e109013. [Google Scholar] [CrossRef] [PubMed]
- Von Groote, P.; Bickenbach, J.; Gutenbrunner, C. The world report on disability-Implications, perspectives and opportunities for physical and rehabilitation medicine (PRM). J. Rehabil. Med. 2011, 43, 869–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathore, F.A.; Gosney, J.E.; Reinhardt, J.D.; Haig, A.J.; Li, J. Medical Rehabilitation After Natural Disasters: Why, When, and How? Arch. Phys. Med. Rehabil. 2012, 93, 1875–1881. [Google Scholar] [CrossRef] [PubMed]
- Gosney, J. Physical Medicine and Rehabilitation: Critical Role in Disaster Response. Disaster Med. Public Health Prep. 2010, 4, 110–112. [Google Scholar] [CrossRef]
- Ghasem, M.; Ardalan, A.; Hamidreza, K.; Mohammad, K.; Abba, O. Physical Rehabilitation Services in Disasters and Emergencies: A Systematic Review. Iran. J. Public Health 2019, 48, 808–815. [Google Scholar]
- Khan, F.; Amatya, B.; Gosney, J.; Rathore, F.A.; Burkle, F.M., Jr. Medical Rehabilitation in Natural Disasters: A Systematic Review. Arch. Phys. Med. Rehabil. 2015, 96, 1709–1727. [Google Scholar] [CrossRef] [Green Version]
- Sheikhbardsiri, H.; Yarmohammadian, M.H.; Rezaei, F.; Maracy, M.R. Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review. World J. Emerg. Med. 2017, 8, 253–263. [Google Scholar] [CrossRef] [Green Version]
- Parker, G.; Lie, D.; Siskind, J.D.; Martin-Khan, M.; Raphael, B.; Crompton, D.; Kisely, S. Mental health implications for older adults after natural disasters—A systematic review and meta-analysis. Int. Psychogeriatr. 2016, 28, 11–20. [Google Scholar] [CrossRef]
- Takayama, S.; Kaneko, S.; Numata, T.; Kamiya, T.; Arita, R.; Saito, N.; Kikuchi, A.; Ohsawa, M.; Kohayagawa, Y.; Ishii, T. Literature Review: Herbal Medicine Treatment after Large-Scale Disasters. Am. J Chin. Med. 2017, 45, 1345–1364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osei, F.; Omoniyi, M.; Boateng, A.K. Clinical and Traditional Rehabilitation Approaches on Injured Football Athletes in Ashanti Region. Ital. J. Sports Rehabil. Posturol. 2015, 2, 242–253. [Google Scholar]
- Dunning, K.N.; Zhao, M.; Haley, R. Physical therapy in China: Entwining cultural practices. Rehab. Manag. 2009, 22, 28–29. [Google Scholar]
- Nussbaum, R.; Kelly, C.; Quinby, E.; Mac, A.; Parmanto, B.; Dicianno, B.E. Systematic Review of Mobile Health Applications in Rehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Paparrigopoulos, T.J.; Pappa, D.A.; Christodoulou, G.N. Early post-traumatic stress disorder in relation to acute stress reaction: An ICD-10 study among help seekers following an earthquake. Psychiatry Res. 2006, 143, 245–253. [Google Scholar] [CrossRef]
- Rintala, A.; Päivärinne, V.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of Technology-Based Distance Physical Rehabilitation Interventions for Improving Physical Functioning in Stroke: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 1339–1358. [Google Scholar] [CrossRef]
- García-Rudolph, A.; Laxe, S.; Saurí, J.; Opisso, E.; Tormos, J.M.; Bernabeu, M. Evidence of chronic stroke rehabilitation interventions in activities and participation outcomes: Systematic review of meta-analyses of randomized controlled trials. Eur. J. Phys. Rehabil. Med. 2019. [Google Scholar] [CrossRef]
- Alejandro, R.J.; Murray, W.E. (Eds.) Randomized Controlled Trials: Questions, Answers, and Musings; BMJ Books; John Wiley & Sons: Hoboken, NJ, USA, 2007; Volume 2, p. 160. [Google Scholar]
- Gosney, J.; O’Connell, C. Rehabilitation of Disaster Casualties. In Disaster Medicine: Comprehensive Principles and Practices, 2nd ed.; Koenig, K., Schultz, C., Eds.; Cambridge University Press: Cambridge, MA, USA, 2016; pp. 377–388. [Google Scholar]



{kind=link}
{kind=link}
| Author/Year | Study Design | Study Objective(s)/Aim(s) | Intervention(s) | Participant Inclusion and Type of Subject | Subject Gender/Age | Study Outcome Measurement | Recommendations/Primary Findings | |
|---|---|---|---|---|---|---|---|---|
| 1 | Zang Yinyin [36]/ 2013 | RCT | Evaluate the efficacy of NET as a short-term treatment for PTSD earthquake survivors. | NET | 22/PTSD | Male = 5; Female = 17/ E = 56.64 & C = 54.82 | PTSD symptoms, general mental health, social support, coping style and posttraumatic change | Effectiveness in treating post-earthquake traumatic symptoms in adult Chinese earthquake survivors |
| 2 | Ying Chen [38]/ 2014 | RCT | Compared the treatment effectiveness of short-term CBT with a general supportive intervention and with a control group of non-treatment. | CBT | 40/Adolescence | Male = 13; Female = 27/Age = 14.50 | Psychological resilience, PTSD & depression | CBT was effective in reducing PTSD and depressive symptoms, improved psychological resilience |
| 3 | Meng XianZe [35]/ 2012 | RCT | Investigated effects of a Chinese herbal formula on GPS in earthquake survivors with PTSD | 12g packages of granulated XTJYF or placebo twice a day for eight weeks. Instructed to drink the contents dissolved in warm, boiled water. | 268/PTSD | Male = 71; Female = 174/E = 51.2 & C = 51.0 | Self-reporting psychological distress | XTJYF may be an effective and safe treatment option for improving GPS in patients with PTSD |
| 4 | Jiang Ruifang [39]/ 2014 | RCT | Test the efficacy of IPT delivered by trained local personnel compared with TAU for PTSD and MDD among adults affected by the Sichuan 2008 earthquake. | IPT | 49/PTSD, MDD | Male = 35; Female = 14/ E = 24.79 & C = 36.05 | CAPS & SCID | IPT is a promising treatment for reducing PTSD and depression |
| 5 | Xia Zhang [16]/ 2013 | Longitudinal quasi-experimental study | Evaluated the effectiveness of the NHV program | NHV Rehabilitation Services Program | 510/Disabling injuries | Male = 179; Female = 331/ E = 55.2:L = 53.4 & C = 51.8 | BI | NHV improved the long-term physical functioning of Sichuan earthquake survivors with disabling injuries |
| 6 | Jun Ni [17]/2013 | Cross-sectional survey | Evaluated the effectiveness of a rehabilitation intervention on PDF and PTSD in fractured victims to identify risk factors for PTSD. | Regular rehabilitation | 459/Fracture | Male = 16; Female = 296/<30 = 52:30–50 = 129:50–70 = 196: > 70 = 82 | PCL-C, Muscle strength, ROM, sensory function and sit-to-stand balance capacity | PDF and PTSD were significantly reduced by the rehabilitation intervention |
| 7 | Li Ling [20]/ 2015 | Prospective cohort study | Examined the development and determinants of long-term outcomes for earthquake victims with amputations | Institution-based rehabilitation | 45/Amputation | Male = 22; Female = 23/Age = 43.5 | VAS, BI, SF-36 and Life Satisfaction Questionnaire-11 | While amputees’ functioning and pain were improved over time, QoL and life satisfaction did not change |
| 8 | Li Wing Sum [40]/ 2018 | Cross-sectional study | Identified factors associated with successful functional recovery of bilateral amputees’ age. | Stand Tall rehabilitation programme | 17/Traumatic bilateral amputation | Male = 8; Female = 9/ Age = 26.59 | Mobility, prosthesis use and health-related QoL | Rehabilitation makes better in adjustment and QoL in bilateral lower limb amputees |
| 9 | Li Yongqiang [19]/ 2012 | Non-RCT clinical study | Assessed the effect of individualized physical rehabilitation programming on victims’ functional recovery. | Physical rehabilitation programming | 51/ SCI | Male = 21; Female = 30/age ranged 11–77 years - with the majority of persons between 18 and 60 years of age. | Ambulation, wheelchair mobility and ADL | Earthquake victims with SCI improved on physical rehabilitation programme |
| 10 | Zhu Zhuohong [37]/ 2014 | Non-RCT clinical study | Investigated the treatment effects of calligraphy therapy on child survivors of Sichuan earthquakes | Calligraphy training 1 hour a day | 210/PTSD | Boys = 105; Girls = 105/children in the fourth and fifth grades | PTSD, calligraphy therapy, salivary cortisol, salivary cortisol levels and arousal scores | Successful calligraphy treatment is an effective and culturally congruent system of intervention |
| 11 | Wang Z [41]/2016 | Non-RCT clinical study | Examined the use of a Web-based self-help intervention program and investigate the relationship between program use and user characteristics | A Web-based self-help intervention | 146/General | Male = 34; Female = 112/Age range:16-25 = 30:26-40 = 64:41-70 = 52 | PDS, SCL-D, CSE, CSS & SFI | Both individual (e.g. demographic, health problems, psychological) and social factors (e.g. social functioning, social support) should be considered when delivering Web-based interventions |
| Author(s)/Year | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Measurement of Intervention(s) | Bias Due to Departures from Intended Intervention(s) | Bias Due to Missing Data | Bias in Measurement of Outcome(s) | Bias in Selection of Reported Result(s) | Overall Bias | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Li Yongqiang/ 2012 | Low | Moderate | Low | Low | Moderate | Moderate | Low | Moderate |
| 2 | Xia Zhang/ 2013 | Low | Moderate | Low | Moderate | Moderate | Moderate | Low | Moderate |
| 3 | Jun Ni/ 2013 | Moderate | Moderate | Low | Moderate | Low | Moderate | Low | Moderate |
| 4 | Zhu Zhuohong/ 2014 | Low | Low | Moderate | Moderate | Low | Moderate | Low | Moderate |
| 5 | Li Ling/ 2015 | Serious | Moderate | Serious | No information | Critical | Low | Low | Critical |
| 6 | Wang Z/ 2016 | Moderate | Moderate | Moderate | No information | Low | Moderate | Low | Moderate |
| 7 | Li Wing Sum/ 2019 | Moderate | Serious | Moderate | Low | Low | Moderate | Low | Serious |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimuli Balikuddembe, J.; Zeng, X.; Chen, C. Health-Related Rehabilitation after the 2008 Great Wenchuan Earthquake in China: A Ten Year Retrospective Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2297. https://doi.org/10.3390/ijerph17072297
Kimuli Balikuddembe J, Zeng X, Chen C. Health-Related Rehabilitation after the 2008 Great Wenchuan Earthquake in China: A Ten Year Retrospective Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(7):2297. https://doi.org/10.3390/ijerph17072297
Chicago/Turabian StyleKimuli Balikuddembe, Joseph, Xinglin Zeng, and Chuandong Chen. 2020. "Health-Related Rehabilitation after the 2008 Great Wenchuan Earthquake in China: A Ten Year Retrospective Systematic Review" International Journal of Environmental Research and Public Health 17, no. 7: 2297. https://doi.org/10.3390/ijerph17072297