Diet, Lifestyle and Cardiovascular Diseases: Linking Pathophysiology to Cardioprotective Effects of Natural Bioactive Compounds

 ,
,  , ,
, , 
 , , ,
, , ,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Cardiovascular Risk Factors, Diet, Lifestyle and Cardioprotective Benefits of Plant-Food Derived Bioactive Compounds
2.1. Sedentary Lifestyle
2.2. Hypertension
2.3. Smoking
2.4. Stress
2.5. Obesity
2.6. Diabetes
2.7. Dyslipidemia
3. Cardioprotective Properties of Plant-Food Bioactives—Preclinical Studies
3.1. In Vitro Studies
3.2. In Vivo Studies
4. Clinical Trials of Natural Bioactive Molecules with Cardioprotective Properties

{kind=link}
{kind=link}
{kind=link}
| Natural Compound | Model | Molecular Mechanism of Action | Ref |
|---|---|---|---|
| In Vitro Preclinical Studies | |||
| omega-3 polyunsaturated fatty acids | neonatal cardiac myocytes | ↑endothelial function antiarrhythmic potential: cell membrane structure modification, direct effect on calcium channels and cardiomyocytes, role in eicosanoid metabolism | [143] |
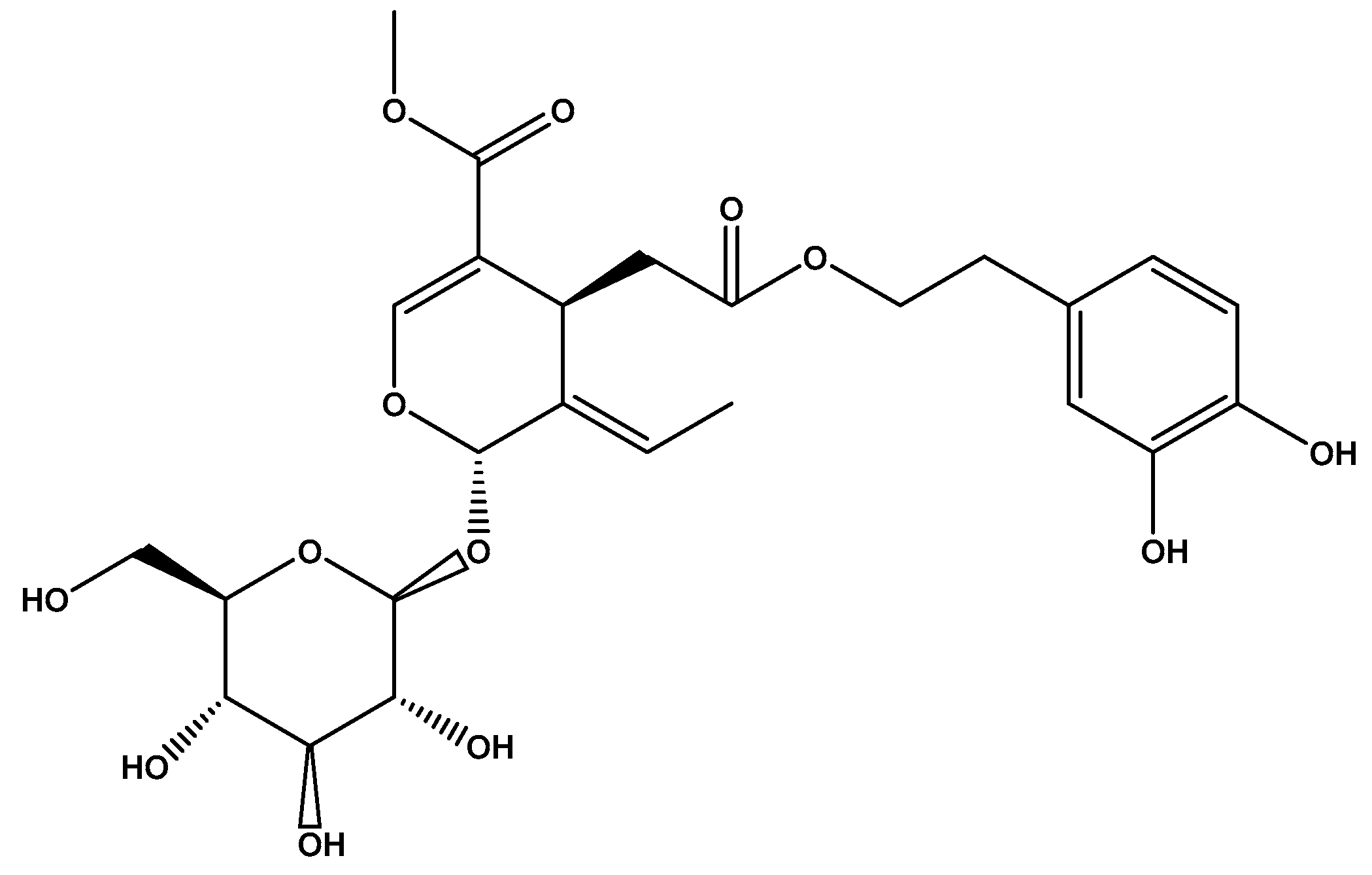
| oleuropein | human LDL and Caco-2 cell lines | ↓prooxidative processes | [149] |
| flavonoids | hepatocytes cell lines | ↓plasma lipids, ↑vascular inflammatory response reduction ↓LDL oxidation, ↑LDL receptor expression, ↓ MMP-2, ↓MMP-9 | [150] |
| anthocyanins | H9C2 cardiomyocytes cell lines | cardioprotective effects on endothelial cell level, ↑vascular homeostasis ↓ROS | [155] [157] [158] |
| aspalathin (flavonoid from rooibos tea) | H9C2 cardiomyocytes cell lines | reverse in metabolic abnormalities by activating ADIPOQ gene, while modulates Pparγ and SREBF 1/2 expression, ↓inflammation via Il6/Jak2 pathway ↑Bcl2 expression, ↓myocardium apoptosis | [159]. |
| cinnamic acid (phenol from cinnamon) | H9C2 cardiomyocytes cell lines | ↑mitochondrial function ↓apoptosis | [160] |
| dealcoholized red wine and cacao procyanidin trimers/pentamers | ex vivo platelet activation | ↑PAC-1 binding, ↑P-selectin expression in blood ↓platelet activation | [161] |
| cocoa flavan-3-ols | human endothelial cells | ↓vascular arginase activity ↑ACE inhibitory activity | [162] [163] |
| almond protein | human umbilical vascular endothelial cells | ↑ACE inhibitory peptides, antihypertensive effect | [164] |
| In vivo preclinical studies | |||
| sterols, tocopherols, phospholipids, phenols, coenzyme (Co) Q9 and Q10 | rats | ↓triglycerides, ↓cholesterol ↑ferric antioxidant capacity, ↑ SOD, ↑GPx, ↑GSH, ↓lipid peroxidation | [178] |
| dichloromethanic fraction of mango leaves | spontaneously hypertensive rats | antihypertensive effect ↓cardiac hypertrophy in spontaneously hypertensive rats treated with the dichloromethanic fraction, ↑ ratio heart weight/body weight | [166] |
| polyphenols (from pomegranate peel) | rats | ↑antioxidative activity against oxidative injury (especially for intestinal injury) | [180] |
5. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pittman, R.N. Regulation of Tissue Oxygenation. In The Circulatory System and Oxygen Transport; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2011. [Google Scholar]
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef] [Green Version]
- WHO. Cardiovascular Diseases (CVDs); World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 12 December 2019).
- Jamee Shahwan, A.; Abed, Y.; Desormais, I.; Magne, J.; Preux, P.M.; Aboyans, V.; Lacroix, P. Epidemiology of coronary artery disease and stroke and associated risk factors in Gaza community -Palestine. PLoS ONE 2019, 14, e0211131. [Google Scholar] [CrossRef] [PubMed]
- Woteki, C.E.; Thomas, P.R. Eat for Life: The Food and Nutrition Board’s Guide to Reducing Your Risk of Chronic Disease; Institute of Medicine (US) Committee on Diet and Health, National Academies Press: Washington, DC, USA, 1992. [Google Scholar]
- Holvoet, P. Stress in obesity and associated metabolic and cardiovascular disorders. Scientifica 2012, 2012, 205027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowles, J.W.; Ashley, E.A. Cardiovascular disease: The rise of the genetic risk score. PLoS Med. 2018, 15, e1002546. [Google Scholar] [CrossRef] [PubMed]
- Assimes, T.L.; Roberts, R. Genetics: Implications for prevention and management of coronary artery disease. J. Am. Coll. Cardiol. 2016, 68, 2797–2818. [Google Scholar] [CrossRef] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Chen, C.Y.; Milbury, P.E.; Lapsley, K.; Blumberg, J.B. Flavonoids from almond skins are bioavailable and act synergistically with vitamins C and E to enhance hamster and human LDL resistance to oxidation. J. Nutr. 2005, 135, 1366–1373. [Google Scholar] [CrossRef]
- Hattori, Y.; Jojima, T.; Tomizawa, A.; Satoh, H.; Hattori, S.; Kasai, K.; Hayashi, T. A glucagon-like peptide-1 (GLP-1) analogue, liraglutide, upregulates nitric oxide production and exerts anti-inflammatory action in endothelial cells. Diabetologia 2010, 53, 2256–2263. [Google Scholar] [CrossRef]
- Salehi, B.; Lopez-Jornet, P.; Pons-Fuster López, E.; Calina, D.; Sharifi-Rad, M.; Ramírez-Alarcón, K.; Forman, K.; Fernández, M.; Martorell, M.; Setzer, W.N. Plant-Derived Bioactives in Oral Mucosal Lesions: A Key Emphasis to Curcumin, Lycopene, Chamomile, Aloe vera, Green Tea and Coffee Properties. Biomolecules 2019, 9, 106. [Google Scholar] [CrossRef] [Green Version]
- Wink, M. Modes of action of herbal medicines and plant secondary metabolites. Medicines 2015, 2, 251–286. [Google Scholar] [CrossRef]
- Zhang, H.; Tsao, R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr. Opin. Food Sci. 2016, 8, 33–42. [Google Scholar] [CrossRef]
- Zern, T.L.; Fernandez, M.L. Cardioprotective effects of dietary polyphenols. J. Nutr. 2005, 135, 2291–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-Pinilla, F.; Nguyen, T.T.J. Natural mood foods: The actions of polyphenols against psychiatric and cognitive disorders. Nutr. Neurosci. 2012, 15, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Scalbert, A.; Williamson, G. Dietary intake and bioavailability of polyphenols. J. Nutr. 2000, 130, 2073–2085. [Google Scholar] [CrossRef]
- Tomas-Barberan, F.A.; Selma, M.V.; Espín, J.C. Polyphenols’ Gut Microbiota Metabolites: Bioactives or Biomarkers? J. Agric. Food Chem. 2018, 66, 3593–3594. [Google Scholar] [CrossRef]
- Bhuyan, D.; Basu, A. Phenolic Compounds: Potential Health Benefits and Toxicity. In Utilisation of Bioactive Compounds from Agricultural and Food Waste; Laylor and Francis: Boca Raton, FL, USA, 2017; pp. 27–34. [Google Scholar]
- Cicero, A.; Colletti, A. Food and plant bioactives for reducing cardiometabolic disease: How does the evidence stack up? Trends Food Sci. Technol. 2017, 69, 192–202. [Google Scholar] [CrossRef]
- Duthie, G.; Duthie, S.; Kyle, J. Plant polyphenols in cancer and heart disease: Implications as nutritional antioxidants. Nutr. Res. Rev. 2000, 23, 79–106. [Google Scholar] [CrossRef] [Green Version]
- Chao, S.-C.; Chen, Y.-J.; Huang, K.-H.; Kuo, K.-L.; Yang, T.-H.; Huang, K.-Y.; Wang, C.-C.; Tang, C.-H.; Yang, R.-S.; Liu, S.-H. Induction of sirtuin-1 signaling by resveratrol induces human chondrosarcoma cell apoptosis and exhibits antitumor activity. Sci. Rep. 2017, 7, 3180. [Google Scholar] [CrossRef]
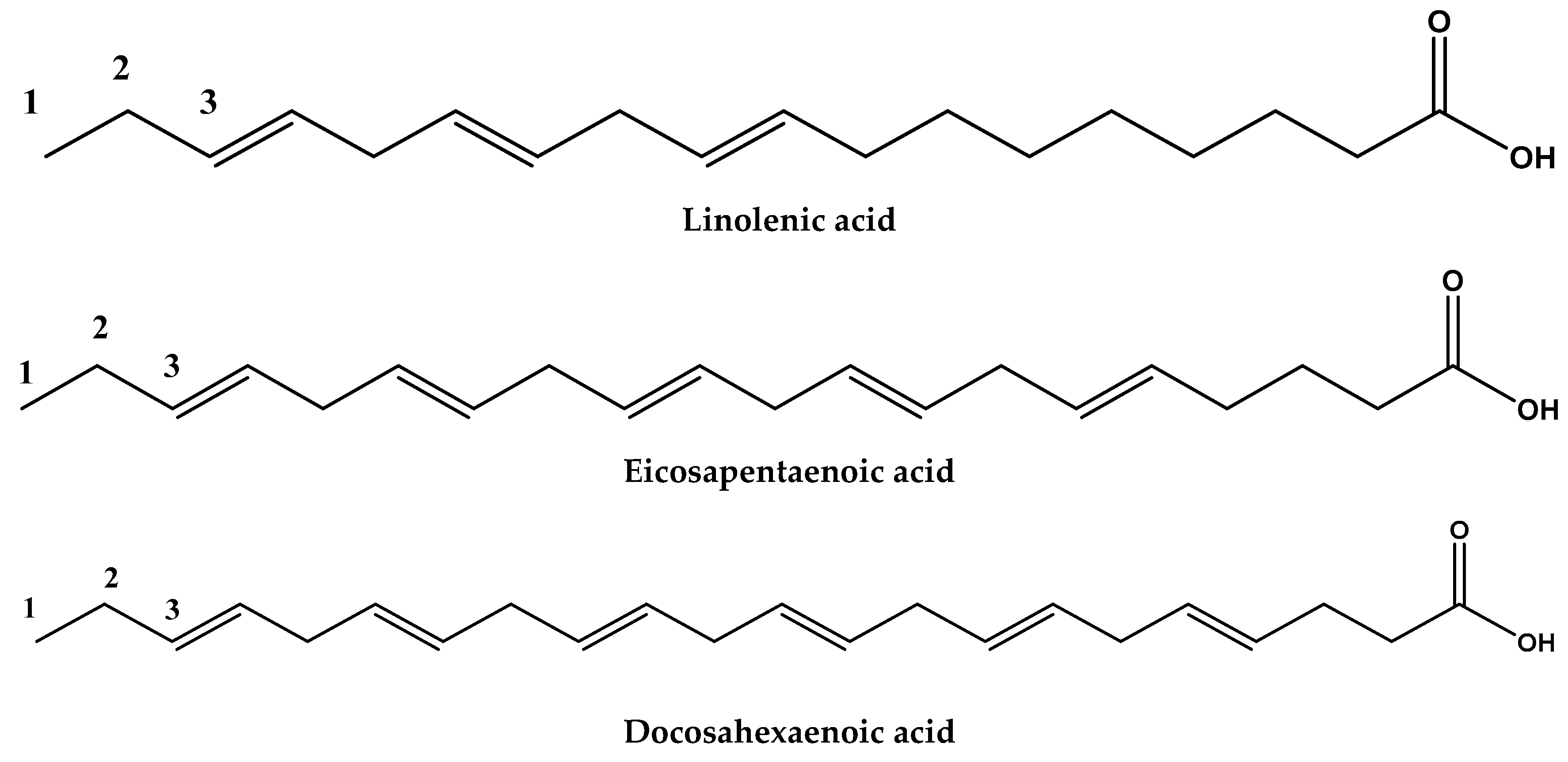
- Abedi, E.; Mohammad, A.S. Long-chain polyunsaturated fatty acid sources and evaluation of their nutritional and functional properties. Food Sci. Nutr. 2014, 2, 443–463. [Google Scholar] [CrossRef]
- Ander, B.P.; Dupasiquer, C.; Prociuk, M.A.; Pierce, G.N. Polyunsaturated fatty acids and their effects on cardiovascular disease. Exp. Clin. Cardiol. 2003, 8, 85–91. [Google Scholar]
- Siriwardhana, N.; Kalupahana, N.S.; Moustaid Moussa, N. Health benefits of n-3 polyunsaturated fatty acids: Eicosapentaenoic acid and docosahexaenoic acid. Adv. Food Nutr. Res. 2012, 65, 211–222. [Google Scholar]
- González, K.; Fuentes, J.; Márquez, J.L. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Gaziano, T.A. Economic burden and the cost-effectiveness of treatment of cardiovascular diseases in Africa. Heart 2008, 94, 140–144. [Google Scholar] [CrossRef]
- Warren, T.Y.; Barry, V.; Hooker, S.P.; Sui, X.; Church, T.S.; Blair, S.N. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med. Sci. Sports Exerc. 2010, 42, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Young, D.R.; Reynolds, K.; Sidell, M.; Brar, S.; Ghai, N.R.; Sternfeld, B.; Jacobsen, S.J.; Slezak, J.M.; Caan, B.; Quinn, V.P. Effects of physical activity and sedentary time on the risk of heart failure. Circ. Heart Fail. 2014, 7, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Young, D.R.; Hivert, M.F.; Alhassan, S.; Camhi, S.M.; Ferguson, J.F.; Katzmarzyk, P.T.; Lewis, C.E.; Owen, N.; Perry, C.K.; Siddique, J.; et al. Sedentary behavior and cardiovascular morbidity and mortality. Circulation 2016, 134, 262–279. [Google Scholar] [CrossRef]
- Reddigan, J.I.; Ardern, C.I.; Riddell, M.C.; Kuk, J.L. Relation of physical activity to cardiovascular disease mortality and the influence of cardiometabolic risk factors. Am. J. Cardiol. 2011, 108, 1426–1431. [Google Scholar] [CrossRef]
- Gobbo, L.C.D.; Kalantarian, S.; Imamura, F.; Lemaitre, R.; Siscovick, D.S.; Psaty, B.M. Contribution of major lifestyle risk factors for incident heart failure in older adults. JACC Heart Fail. 2015, 3, 520–528. [Google Scholar] [CrossRef] [Green Version]
- Hong, X.; Lin, J.; Gu, W. Risk factors and therapies in vascular diseases: An umbrella review of updated systematic reviews and meta-analyses. J. Cell. Physiol. 2019, 234, 8221–8232. [Google Scholar] [CrossRef]
- Tsatsakis, A.; Docea, A.O.; Calina, D.; Tsarouhas, K.; Zamfira, L.-M.; Mitrut, R.; Sharifi-Rad, J.; Kovatsi, L.; Siokas, V.; Dardiotis, E. A mechanistic and pathophysiological approach for stroke associated with drugs of abuse. J. Clin. Med. 2019, 8, 1295. [Google Scholar] [CrossRef] [Green Version]
- Nicoll, R.; Zhao, Y.; Ibrahimi, P.; Olivecrona, G.; Henein, M. Diabetes and hypertension consistently predict the presence and extent of coronary artery calcification in symptomatic patients: A systematic review and meta-analysis. Int. J. Mol. Sci. 2016, 17, 1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Fogacci, F.; Colletti, A. Food and plant bioactives for reducing cardiometabolic disease risk: An evidence based approach. Food Funct. 2017, 8, 2076–2088. [Google Scholar] [CrossRef] [PubMed]
- Patten, G.S.; Abeywardena, M.Y.; Bennett, L.E. Inhibition of angiotensin converting enzyme, angiotensin II receptor blocking, and blood pressure lowering bioactivity across plant families. Crit. Rev. Food Sci. Nutr. 2016, 56, 181–214. [Google Scholar] [CrossRef] [PubMed]
- Li, G.H.; Le, G.W.; Shi, Y.H.; Shrestha, S. Angiotensin I–converting enzyme inhibitory peptides derived from food proteins and their physiological and pharmacological effects. Nutr. Res. 2004, 24, 469–486. [Google Scholar] [CrossRef]
- Salehi, B.; Mnayer, D.; Özçelik, B.; Altin, G.; Kasapoǧlu, K.N.; Daskaya-Dikmen, C.; Sharifi-Rad, J. Plants of the genus Lavandula: From farm to pharmacy. Natl. Prod. Commun. 2018, 13, 726–740. [Google Scholar] [CrossRef] [Green Version]
- Iwaniak, A.; Minkiewicz, P.; Darewicz, M. Food-originating ACE inhibitors, including antihypertensive peptides, as preventive food components in blood pressure reduction. Compr. Rev. Food Sci. Food Saf. 2014, 13, 114–134. [Google Scholar] [CrossRef]
- Daskaya-Dikmen, C.; Yucetepe, A.; Karbancioglu-Guler, F.; Daskaya, H.; Ozcelik, B.; Daskaya-Dikmen, C.; Ozcelik, B. Angiotensin-I-converting enzyme (ACE)-inhibitory peptides from plants. Nutrients 2017, 9, 316. [Google Scholar] [CrossRef]
- Guang, C.; Phillips, R.D. Plant food-derived angiotensin I converting enzyme inhibitory peptides. J. Agric. Food Chem. 2009, 57, 5113–5120. [Google Scholar] [CrossRef]
- Ademiluyi, A.O.; Oboh, G.; Ogunsuyi, O.B.; Oloruntoba, F.M. A comparative study on antihypertensive and antioxidant properties of phenolic extracts from fruit and leaf of some guava (Psidium guajava L.) varieties. Comp. Clin. Pathol. 2016, 25, 363–374. [Google Scholar] [CrossRef]
- García, M.C.; González-García, E.; Vásquez-Villanueva, R.; Marina, M.L. Apricot and other seed stones: Amygdalin content and the potential to obtain antioxidant, angiotensin I converting enzyme inhibitor and hypocholesterolemic peptides. Food Funct. 2016, 7, 4693–4701. [Google Scholar] [CrossRef]
- Gupta, N.; Srivastava, N.; Bhagyawant, S.S. Vicilin—A major storage protein of mungbean exhibits antioxidative potential, antiproliferative effects and ACE inhibitory activity. PLoS ONE 2018, 13, e0191265. [Google Scholar] [CrossRef] [PubMed]
- Bagchi, D.; Sen, C.K.; Ray, S.D.; Das, D.K.; Bagchi, M.; Preuss, H.G.; Vinson, J.A. Molecular mechanisms of cardioprotection by a novel grape seed proanthocyanidin extract. Mutat. Res. 2003, 523–524, 87–97. [Google Scholar] [CrossRef]
- Kahl, K.G.; Stapel, B.; Frieling, H. Link between depression and cardiovascular diseases due to epigenomics and proteomics: Focus on energy metabolism. Prog. Neuropsychopharmacol. Biol. Psychiatr. 2019, 89, 146–157. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Singh, S. Herbal approach for management of atherosclerosis: A review. Curr. Atheroscler. Rep. 2019, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Rescigno, A.; Dettori, T.; Calina, D.; Docea, A.O.; Singh, L.; Cebeci, F.; Özçelik, B.; Bhia, M.; Dowlati Beirami, A. Avocado–Soybean Unsaponifiables: A Panoply of Potentialities to Be Exploited. Biomolecules 2020, 10, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habanova, M.; Saraiva, J.A.; Haban, M.; Schwarzova, M.; Chlebo, P.; Predna, L.; Gažo, J.; Wyka, J. Intake of bilberries (Vaccinium myrtillus L.) reduced risk factors for cardiovascular disease by inducing favorable changes in lipoprotein profiles. Nutr. Res. 2016, 36, 1415–1422. [Google Scholar] [CrossRef]
- Wenzig, E.; Widowitz, U.; Kunert, O.; Chrubasik, S.; Bucar, F.; Knauder, E.; Bauer, R. Phytochemical composition and in vitro pharmacological activity of two rose hip (Rosa canina L.) preparations. Phytomedicine 2008, 15, 826–835. [Google Scholar] [CrossRef]
- Król, S.K.; Kiełbus, M.; Rivero-Müller, A.; Stepulak, A. Comprehensive review on betulin as a potent anticancer agent. BioMed Res. Int. 2015, 2015, 584189. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.; Liu, X.-F.; Ke, Z.-Q.; Yao, Q.; Guo, S.; Liu, C. Resveratrol modulates apoptosis and autophagy induced by high glucose and palmitate in cardiac cells. Cell. Physiol. Biochem. 2018, 46, 2031–2040. [Google Scholar] [CrossRef]
- Sgambato, A.; Ardito, R.; Faraglia, B.; Boninsegna, A.; Wolf, F.I.; Cittadini, A. Resveratrol, a natural phenolic compound, inhibits cell proliferation and prevents oxidative DNA damage. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2001, 496, 171–180. [Google Scholar] [CrossRef]
- Wright, E.N.; Hanlon, A.; Lozano, A.; Teitelman, A.M. The impact of intimate partner violence, depressive symptoms, alcohol dependence, and perceived stress on 30-year cardiovascular disease risk among young adult women: A multiple mediation analysis. Prev. Med. 2019, 121, 47–54. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.; Seeman, T. Allostatic Load and Allostatsis. In MacArthur Research Network on Socioeconomic Status and Health: Allostatic Load Notebook. 2009. Available online: http://www.macses.ucsf.edu/research/allostatic/allostatic.php (accessed on 12 December 2019).
- Coughlin, S.S. Post-traumatic stress disorder and cardiovascular disease. Open Cardiovasc. Med. J. 2011, 5, 164–170. [Google Scholar] [CrossRef]
- Milenkovic, D.; Morand, C.; Cassidy, A.; Konic-Ristic, A.; Tomás-Barberán, F.; Ordovas, J.M.; Kroon, P.; De Caterina, R.; Rodriguez-Mateos, A. Interindividual variability in biomarkers of cardiometabolic health after consumption of major plant-food bioactive compounds and the determinants involved. Adv. Nutr. 2017, 8, 558–570. [Google Scholar] [PubMed]
- Runnie, I.; Salleh, M.N.; Mohamed, S.; Head, R.J.; Abeywardena, M.Y. Vasorelaxation induced by common edible tropical plant extracts in isolated rat aorta and mesenteric vascular bed. J. Ethnopharmacol. 2004, 92, 311–316. [Google Scholar] [CrossRef]
- Juneja, L.R.; Chu, D.C.; Okubo, T.; Nagato, Y.; Yokogoshi, H. L-theanine—A unique amino acid of green tea and its relaxation effect in humans. Trends Food Sci. Technol. 1999, 10, 199–204. [Google Scholar] [CrossRef]
- Steptoe, A.; Gibson, E.L.; Vounonvirta, R.; Williams, E.D.; Hamer, M.; Rycroft, J.A.; Erusalimsky, J.D.; Wardle, J. The effects of tea on psychophysiological stress responsivity and post-stress recovery: A randomised double-blind trial. Psychopharmacology 2007, 190, 81–89. [Google Scholar] [CrossRef]
- Chen, J.A.; Vijapura, S.; Papakostas, G.I.; Parkin, S.R.; Kim, D.J.H.; Cusin, C.; Baer, L.; Clain, A.J.; Fava, M.; Mischoulon, D. Association between physician beliefs regarding assigned treatment and clinical response: Re-analysis of data from the hypericum depression trial study group. Asian J. Psychiatr. 2015, 13, 23–29. [Google Scholar] [CrossRef] [Green Version]
- WHO. Obesity and Overweight; World Health Organization. 2017. Available online: http://www.who.int/mediacentre/factsheets/ (accessed on 27 November 2019).
- Vasileva, L.V.; Marcheva, A.S.; Georgiev, M.I. Causes and solutions to “globesity”: The new fa(s)t alarming global epidemic. Food Chem. Toxicol. 2018, 121, 173–193. [Google Scholar] [CrossRef]
- Carbone, S.; Canada, J.M.; Billingsley, H.E.; Siddiqui, M.S.; Elagizi, A.; Lavie, C.J. Obesity paradox in cardiovascular disease: Where do we stand? Vasc. Health Risk Manag. 2019, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Lavie, C.J.; Arena, R.; Alpert, M.A.; Milani, R.V.; Ventura, H.O. Management of cardiovascular diseases in patients with obesity. Nat. Rev. Cardiol. 2018, 15, 45–56. [Google Scholar] [CrossRef]
- Igel, L.I.; Saunders, K.H.; Fins, J.J. Why weight? An analytic review of obesity management, diabetes prevention, and cardiovascularrisk reduction. Curr. Atheroscler. Rep. 2018, 20, 39–45. [Google Scholar] [CrossRef]
- Cripps, C.; Roslin, M. Endoluminal treatments for obesity and related hypertension: Updates, review, and clinical perspective. Curr. Hypertens. Rep. 2016, 18, 79–100. [Google Scholar] [CrossRef]
- Paulis, W.D.; Silva, S.; Koes, B.W.; van Middelkoop, M. Overweight and obesity are associated withmusculoskeletal complaints as early as childhood: A systematic review. Obes. Rev. 2014, 15, 52–67. [Google Scholar] [CrossRef]
- Smith, L.A.; O’Flanagan, C.H.; Bowers, L.W.; Allott, E.H.; Hursting, S.D. Translating mechanism-based strategies to break the obesity-cancer link: A narrative review. J. Acad. Nutr. Diet. 2018, 118, 652–667. [Google Scholar] [CrossRef] [Green Version]
- Karri, S.; Sharma, S.; Hatware, K.; Patil, K. Natural anti-obesity agents and their therapeutic role in management of obesity: A future trend perspective. Biomed. Pharmacother. 2019, 110, 224–238. [Google Scholar] [CrossRef]
- Hsu, C.L.; Yen, G.C. Phenolic compounds: Evidence for inhibitory effects against obesity and their underlying molecular signaling mechanisms. Mol. Nutr. Food Res. 2008, 52, 53–61. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Cekanova, M.; LeMieux, M.; Greer, B.; Moustaid-Moussa, N. Modulation of adipose tissue inflammation by bioactive food compounds. J. Nutr. Biochem. 2013, 24, 613–623. [Google Scholar] [CrossRef]
- Suzuki, T.; Pervin, M.; Goto, S.; Isemura, M.; Nakamura, Y. Beneficial effects of tea and the green tea catechin epigallocatechin-3-gallate on obesity. Molecules 2016, 21, 1305. [Google Scholar] [CrossRef] [Green Version]
- Martel, J.; Ojcius, D.M.; Chang, C.J.; Lin, C.S.; Lu, C.C.; Ko, Y.F.; Tseng, S.F.; Lai, H.C.; Young, J.D. Anti-obesogenic and antidiabetic effects of plants and mushrooms. Nat. Rev. Endocrinol. 2017, 13, 149–160. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, B.; Shen, J.; Wan, L.; Zhu, Y.; Yi, T.; Xiao, Z. The beneficial effects of quercetin, curcumin, and resveratrol in obesity. Oxidative Med. Cell. Longev. 2017, 2017, 1459497. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Virgous, C.; Si, H. Ginseng and obesity: Observations and understanding in cultured cells, animals and humans. J. Nutr. Biochem. 2017, 44, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Azzini, E.; Giacometti, J.; Russo, G.L. Antiobesity effects of anthocyanins in preclinical and clinical studies. Oxidative Med. Cell. Longev. 2017, 2017, 2740364. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.G.V.; Garcia-Diaz, D.F.; Jimenez, P.; Silva, P.I. Bioactive compounds and health benefits of exotic tropical red-blackberries. J. Funct. Foods 2013, 5, 539–549. [Google Scholar] [CrossRef]
- Xie, L.; Su, H.; Sun, C.; Zheng, X.; Chen, W. Recent advances in understanding the anti-obesity activity of anthocyanins and their biosynthesis in microorganisms. Trends Food Sci. Technol. 2018, 72, 13–24. [Google Scholar] [CrossRef]
- Raiola, A.; Errico, A.; Petruk, G.; Monti, D.M.; Barone, A.; Rigano, M.M. Bioactive compounds in Brassicaceae vegetables with a role in the prevention of chronic diseases. Molecules 2018, 23, 15. [Google Scholar] [CrossRef] [Green Version]
- Salehi, B.; Calina, D.; Docea, A.O.; Koirala, N.; Aryal, S.; Lombardo, D.; Pasqua, L.; Taheri, Y.; Marina Salgado Castillo, C.; Martorell, M. Curcumin’s Nanomedicine Formulations for Therapeutic Application in Neurological Diseases. J. Clin. Med. 2020, 9, 430. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Zhang, T.; Shi, L.; Gong, M.; Jin, J.; Zhang, Y.; Liu, R.; Chang, M.; Jin, Q.; Wang, X. The relationship between lipid phytochemicals, obesity and its related chronic diseases. Food Funct. 2018, 9, 6048. [Google Scholar] [CrossRef]
- Trigueros, L.; Peña, S.; Ugidos, A.V.; Sayas-Barberá, E.; Pérez-Álvarez, J.A.; Sendra, E. Food ingredients as anti-obesity agents: A review. Crit. Rev. Food Sci. Nutr. 2013, 53, 929–942. [Google Scholar] [CrossRef]
- Chatterjee, C.; Gleddie, S.; Xiao, W. Soybean bioactive peptides and their functional properties. Nutrients 2018, 10, 1211. [Google Scholar] [CrossRef] [Green Version]
- Marrelli, M.; Amodeo, V.; Statti, G.; Conforti, F. Biological properties and bioactive components of Allium cepa L.: Focus on potential benefits in the treatment of obesity and related comorbidities. Molecules 2019, 24, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, S.; Duncan, A.M. The role of pulses in satiety, food intake and body weight management. J. Funct. Foods 2017, 38, 612–623. [Google Scholar] [CrossRef]
- McCay, C.M.; Crowell, M.F.; Maynard, L.A. The effect of retarded growth upon the length of life span and upon the ultimate body size: One figure. J. Nutr. 1935, 10, 63–79. [Google Scholar] [CrossRef]
- Masoro, E.J. Caloric restriction and aging: An update. Exp. Gerontol. 2000, 35, 299–305. [Google Scholar] [CrossRef]
- Fontana, L.; Villareal, D.T.; Weiss, E.P.; Racette, S.B.; Steger-May, K.; Klein, S.; Holloszy, J.O. Calorie restriction or exercise: Effects on coronary heart disease risk factors. A randomized, controlled trial. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E197–E202. [Google Scholar] [CrossRef] [PubMed]
- Stewart, T.; Bhapkar, M.; Das, S.; Galan, K.; Martin, C.; McAdams, L.; Pieper, C.; Redman, L.; Roberts, S.; Stein, R. Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy Phase 2 (CALERIE Phase 2) screening and recruitment: Methods and results. Contemp. Clin. Trials 2013, 34, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggenenti, P.; Abbate, M.; Ruggiero, B.; Rota, S.; Trillini, M.; Aparicio, C.; Parvanova, A.; Iliev, I.P.; Pisanu, G.; Perna, A. Renal and systemic effects of calorie restriction in patients with type 2 diabetes with abdominal obesity: A randomized controlled trial. Diabetes 2017, 66, 75–86. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; Wohlgemuth, S.E.; Anton, S.D.; Bernabei, R.; Carter, C.S.; Leeuwenburgh, C. Cellular mechanisms of cardioprotection by calorie restriction: State of the science and future perspectives. Clin. Geriatr. Med. 2009, 25, 715–732. [Google Scholar] [CrossRef] [Green Version]
- ROTH, G.S.; LANE, M.A.; INGRAM, D.K. Caloric restriction mimetics: The next phase. Ann. N. Y. Acad. Sci. 2005, 1057, 365–371. [Google Scholar] [CrossRef]
- Mariño, G.; Pietrocola, F.; Kong, Y.; Eisenberg, T.; Hill, J.A.; Madeo, F.; Kroemer, G. Dimethyl α-ketoglutarate inhibits maladaptive autophagy in pressure overload-induced cardiomyopathy. Autophagy 2014, 10, 930–932. [Google Scholar] [CrossRef] [Green Version]
- Devipriya, B.; Kumaradhas, P. Molecular flexibility and the electrostatic moments of curcumin and its derivatives in the active site of p300: A theoretical charge density study. Chem. Biol. Interact. 2013, 204, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanyam, K.; Altaf, M.; Varier, R.A.; Swaminathan, V.; Ravindran, A.; Sadhale, P.P.; Kundu, T.K. Polyisoprenylated benzophenone, garcinol, a natural histone acetyltransferase inhibitor, represses chromatin transcription and alters global gene expression. J. Biol. Chem. 2004, 279, 33716–33726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devipriya, B.; Kumaradhas, P. Probing the effect of intermolecular interaction and understanding the electrostatic moments of anacardic acid in the active site of p300 enzyme via DFT and charge density analysis. J. Mol. Graph. Model. 2012, 34, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.-C.; Jung, M.G.; Lee, Y.-H.; Yoon, J.C.; Kwon, S.H.; Kang, H.-B.; Kim, M.-J.; Cha, J.-H.; Kim, Y.J.; Jun, W.J. Epigallocatechin-3-gallate, a histone acetyltransferase inhibitor, inhibits EBV-induced B lymphocyte transformation via suppression of RelA acetylation. Cancer Res. 2009, 69, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morselli, E.; Mariño, G.; Bennetzen, M.V.; Eisenberg, T.; Megalou, E.; Schroeder, S.; Cabrera, S.; Bénit, P.; Rustin, P.; Criollo, A. Spermidine and resveratrol induce autophagy by distinct pathways converging on the acetylproteome. J. Cell Biol. 2011, 192, 615–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barger, J.L.; Kayo, T.; Pugh, T.; Prolla, T.; Weindruch, R. Short-term consumption of a resveratrol-containing nutraceutical mixture mimics gene expression of long-term caloric restriction in mouse heart. Exp. Gerontol. 2008, 43, 859–866. [Google Scholar] [CrossRef]
- WHO. Global Report on Diabetes; World Health Organization. 2016. Available online: https://www.who.int/diabetes/global-report/en/ (accessed on 27 November 2019).
- Chen, L.; Magliano, D.J.; Zimmet, P.Z. The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat. Rev. Endocrinol. 2012, 8, 228–236. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes-2008. Diabetes Care 2008, 31, 12–54. [Google Scholar] [CrossRef] [Green Version]
- Prasad, V.S.S.; Adapa, D.; Van, D.R.; Choudhury, A.; Jahangir, M.A.; Chatterjee, A. Nutritional components relevant to type-2-diabetes: Dietary sources, metabolic functions and glycaemic effects. J. Res. Med. Dent. Sci. 2018, 6, 52–75. [Google Scholar]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary polyphenols, Mediterranean diet, prediabetes, and type 2 diabetes: A narrative review of the evidence. Oxid. Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Parveen, A.; Kim, J.H.; Oh, B.G.; Subedi, L.; Khan, Z.; Kim, S.Y. Phytochemicals: Target-based therapeutic strategies for diabetic retinopathy. Molecules 2018, 23, 1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teoh, S.L.; Das, S. Phytochemicals and their effective role in the treatment of diabetes mellitus: A short review. Phytochem. Rev. 2018, 17, 1111–1128. [Google Scholar] [CrossRef]
- Anuradha, C.V. Phytochemicals targeting genes relevant for type 2 diabetes. Can. J. Physiol. Pharmacol. 2013, 91, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Martinez-González, M.Á.; Bulló, M.; Ros, E. The role of diet in the prevention of type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 32–48. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Zare, V.; Butler, A.E.; Barreto, G.E.; Sahebkar, A. Antidiabetic potential of saffron and its active constituents. J. Cell. Physiol. 2019, 234, 8610–8617. [Google Scholar] [CrossRef] [PubMed]
- Rosa-Sibakov, N.; Poutanen, K.; Micard, V. How does wheat grain, bran and aleurone structure impact their nutritional and technological properties? Trends Food Sci. Technol. 2015, 41, 118–134. [Google Scholar] [CrossRef]
- McRae, M.P. Dietary fiber intake and type 2 diabetes mellitus: An umbrella review of metaanalyses. J. Chiropr. Med. 2018, 17, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.; Hillen, C.; Robinson, J.G. Composition, nutritional value, and health benefits of pulses. Cereal Chem. 2017, 94, 11–31. [Google Scholar] [CrossRef]
- Rebello, C.J.; Greenway, F.L.; Finley, J.W. Whole grains and pulses: A comparison of the nutritional and health benefits. J. Agric. Food Chem. 2014, 62, 7029–7049. [Google Scholar] [CrossRef]
- Kopin, L.; Lowenstein, C.J. Dyslipidemia. Ann. Intern. Med. 2017, 167, ITC81–ITC96. [Google Scholar] [CrossRef]
- Goldstein, J.L.; Brown, M.S. A century of cholesterol and coronaries: From plaques to genes to statins. Cell 2015, 161, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Status Report on Noncommunicable Diseases; World Health Organization. 2014. Available online: https://www.who.int/nmh/publications/ncd-status-report-2014/en/ (accessed on 27 November 2019).
- Sirtori, C.R.; Anderson, J.W.; Arnoldi, A. Nutritional and nutraceutical considerations for dyslipidemia. Future Lipidol. 2007, 3, 313–339. [Google Scholar] [CrossRef]
- Ashen, M.D.; Blumenthal, R.S. Clinical practice. Low HDL cholesterol levels. N. Engl. J. Med. 2005, 353, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Tomé-Carneiro, J.; Visioli, F. Polyphenol-based nutraceuticals for the prevention and treatment of cardiovascular disease: Review of human evidence. Phytomedicine 2016, 23, 1145–1174. [Google Scholar] [CrossRef] [PubMed]
- Potì, F.; Santi, D.; Spaggiari, G.; Zimetti, F.; Zanotti, I. Polyphenol health effects on cardiovascular and neurodegenerative disorders: A review and meta-analysis. Int. J. Mol. Sci. 2019, I20, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menezes, R.; Rodriguez-Mateos, A.; Kaltsatou, A.; González-Sarrías, A.; Greyling, A.; Giannaki, C.; Andres-Lacueva, C.; Milenkovic, D.; Gibney, R.; Dumont, J.; et al. Impact of flavonols on cardiometabolic biomarkers: A meta-analysis of randomized controlled human trials to explore the role of inter-individual variability. Nutrients 2017, 9, 117. [Google Scholar] [CrossRef]
- Yung, L.M.; Leung, F.P.; Wong, W.T.; Tian, X.Y.; Yung, L.H.; Chen, Z.Y.; Huang, Y. Tea polyphenols benefit vascular function. Inflammopharmacology 2008, 16, 230–234. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Colletti, A. Combinations of phytomedicines with different lipid lowering activity for dyslipidemia management: The available clinical data. Phytomedicine 2016, 23, 1113–1118. [Google Scholar] [CrossRef]
- Polia, A.; Barbagallo, C.M.; Cicero, A.F.G.; Corsini, A.; Manzato, E.; Trimarco, B.; Bernini, F.; Visioli, F.; Bianchi, A.; Canzone, G.; et al. Nutraceuticals and functional foods for the control of plasma cholesterol levels. An intersociety position paper. Pharmacol. Res. 2018, 134, 51–60. [Google Scholar] [CrossRef]
- Tokede, O.A.; Onabanjo, T.A.; Yansane, A.; Gaziano, J.M.; Djoussé, L. Soya products and serum lipids: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 114, 831–843. [Google Scholar] [CrossRef]
- WHO. Noncommunicable Diseases Country Profiles 2014; World Health Organization. 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf (accessed on 12 December 2019).
- Guha, S.; Majumder, K. Structural-features of food-derived bioactive peptides with anti-inflammatory activity: A brief review. J. Food Biochem. 2019, 43, e12531. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Chandra, S.; Alexander, S.; Soble, J.; Williams, K.A. Plant-based nutrition: An essential component of cardiovascular disease prevention and management. Curr. Cardiol. Rep. 2017, 19, 104. [Google Scholar] [CrossRef] [PubMed]
- Hassellund, S.S.; Flaa, A.; Kjeldsen, S.E.; Seljeflot, I.; Karlsen, A.; Erlund, I.; Rostrup, M. Effects of anthocyanins on cardiovascular risk factors and inflammation in pre-hypertensive men: A double-blind randomized placebo-controlled crossover study. J. Hum. Hypertens. 2013, 27, 100–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granato, D.; Nunes, D.S.; Barba, F.J. An integrated strategy between food chemistry, biology, nutrition, pharmacology, and statistics in the development of functional foods: A proposal. Trends Food Sci. Technol. 2017, 62, 13–22. [Google Scholar] [CrossRef]
- Martins, N.; Barros, L.; Ferreira, I.C. In vivo antioxidant activity of phenolic compounds: Facts and gaps. Trends Food Sci. Technol. 2016, 48, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Padureanu, R.; Albu, C.V.; Mititelu, R.R.; Bacanoiu, M.V.; Docea, A.O.; Calina, D.; Padureanu, V.; Olaru, G.; Sandu, R.E.; Malin, R.D. Oxidative stress and inflammation interdependence in multiple sclerosis. J. Clin. Med. 2019, 8, 1815. [Google Scholar] [CrossRef] [Green Version]
- Torres-Fuentes, C.; Schellekens, H.; Dinan, T.G.; Cryan, J.F. A natural solution for obesity: Bioactives for the prevention and treatment of weight gain. A review. Nutr. Neurosci. 2015, 18, 49–65. [Google Scholar] [CrossRef]
- Salehi, B.; Capanoglu, E.; Adrar, N.; Catalkaya, G.; Shaheen, S.; Jaffer, M.; Giri, L.; Suyal, R.; Jugran, A.K.; Calina, D. Cucurbits plants: A key emphasis to its pharmacological potential. Molecules 2019, 24, 1854. [Google Scholar] [CrossRef] [Green Version]
- Colussi, G.; Catena, C.; Novello, M.; Bertin, N.; Sechi, L.A. Impact of omega-3 polyunsaturated fatty acids on vascular function and blood pressure: Relevance for cardiovascular outcomes. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 191–200. [Google Scholar] [CrossRef]
- Harris, W.S.; Miller, M.; Tighe, A.P.; Davidson, M.H.; Schaefer, E.J. Omega-3 fatty acids and coronary heart disease risk: Clinical and mechanistic perspectives. Atherosclerosis 2008, 197, 12–24. [Google Scholar] [CrossRef]
- Siegel, G.; Ermilov, E. Omega-3 fatty acids: Benefits for cardio-cerebro-vascular diseases. Atherosclerosis 2012, 225, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Siscovick, D.S.; Barringer, T.A.; Fretts, A.M.; Wu, J.H.; Lichtenstein, A.H.; Costello, R.B.; Kris-Etherton, P.M.; Jacobson, T.A.; Engler, M.B.; Alger, H.M.; et al. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and the Prevention of Clinical Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation 2017, 135, e867–e884. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, P.; Davidson, N.C.; Schmidt, E.B.; Calder, P.C. Cardiovascular effects of marine omega-3 fatty acids. Lancet 2010, 376, 540–550. [Google Scholar] [CrossRef]
- De Caterina, R.; Cybulsky, M.I.; Clinton, S.K.; Gimbrone, M.A.; Libby, P. The omega-3 fatty acid docosahexaenoate reduces cytokine-induced expression of proatherogenic and proinflammatory proteins in human endothelial cells. Arteriosclerosis and Thrombosis. J. Vasc. Biol. 1994, 14, 1829–1836. [Google Scholar]
- Thota, R.N.; Ferguson, J.J.A.; Abbott, K.A.; Dias, C.B.; Garg, M.L. Science behind the cardio-metabolic benefits of omega-3 polyunsaturated fatty acids: Biochemical effects vs. clinical outcomes. Food Funct. 2018, 9, 3576–3596. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.S.D.; Leitch, J.W.; Falconer, J.; Garg, M.L. Prevention of cardiaca arrhythmia by dietary (n-3) polyunsaturated fatty acids and their mechanism of action. J. Nutr. 1997, 127, 383–393. [Google Scholar] [CrossRef] [Green Version]
- Tejada, S.; Pinya, S.; Mar Bibiloni, M.; Tur, J.A.; Pons, A.; Sureda, A. Cardioprotective effects of the polyphenol hydroxytyrosol from olive oil. Curr. Drug Targets 2017, 18, 1477–1486. [Google Scholar] [CrossRef]
- Omar, S.H. Cardioprotective and neuroprotective roles of oleuropein in olive. Saudi Pharm. J. 2010, 18, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Odiatou, E.M.; Skaltsounis, A.L.; Constantinou, A.I. Identification of the factors responsible for the in vitro pro-oxidant and cytotoxic activities of the olive polyphenols oleuropein and hydroxytyrosol. Cancer Lett. 2013, 330, 113–121. [Google Scholar] [CrossRef]
- Coni, E.; Di Benedetto, R.; Di Pasquale, M.; Masella, R.; Modesti, D.; Mattei, R.; Carlini, E.A. Protective effect of oleuropein, an olive oil biophenol, on low density lipoprotein oxidizability in rabbits. Lipids 2000, 35, 45–54. [Google Scholar] [CrossRef]
- Ruel, G.; Couillard, C. Evidences of the cardioprotective potential of fruits: The case of cranberries. Mol. Nutr. Food Res. 2007, 51, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Shivaprasad Shetty, M.; VAnil Kumar, N.; Živković, J.; Calina, D.; Oana Docea, A.; Emamzadeh-Yazdi, S.; Sibel Kılıç, C.; Goloshvili, T.; Nicola, S.; et al. Veronica Plants—Drifting from Farm to Traditional Healing, Food Application, and Phytopharmacology. Molecules 2019, 24, 2454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, Y.F.; Liu, R.H. Cranberries inhibit LDL oxidation and induce LDL receptor expression in hepatocytes. Life Sci. 2005, 77, 1892–1901. [Google Scholar] [CrossRef] [PubMed]
- Matchett, M.D.; MacKinnon, S.L.; Sweeney, M.I.; Gottschall-Pass, K.T.; Hurta, R.A. Blueberry flavonoids inhibit matrix metalloproteinase activity in DU145 human prostate cancer cells. Biochem. Cell Biol. 2005, 83, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Tate, P.; God, J.; Bibb, R.; Lu, Q.; Larcom, L.L. Inhibition of metalloproteinase activity by fruit extracts. Cancer Lett. 2004, 212, 153–158. [Google Scholar] [CrossRef]
- Castañeda-Ovando, A.; Pacheco-Hernández, M.L.; Páez-Hernández, M.E.; Rodríguez, J.A.; Galán-Vidal, C.A. Chemical studies of anthocyanins: A review. Food Chem. 2009, 113, 859–871. [Google Scholar] [CrossRef]
- Salehi, B.; Sharifi-Rad, J.; Capanoglu, E.; Adrar, N.; Catalkaya, G.; Shaheen, S.; Jaffer, M.; Giri, L.; Suyal, R.; Jugran, A.K. Cucurbita Plants: From farm to industry. Appl. Sci. 2019, 9, 3387. [Google Scholar] [CrossRef] [Green Version]
- Krga, I.; Milenkovic, D. Anthocyanins: From sources and bioavailability to cardiovascular-health benefits and molecular mechanisms of action. J. Agric. Food Chem. 2019, 67, 1771–1783. [Google Scholar] [CrossRef]
- Tenore, G.C.; Manfra, M.; Stiuso, P.; Coppola, L.; Russo, M.; Campiglia, P. Polyphenolic pattern and in vitro cardioprotective properties of typical red wines from vineyards cultivated in Scafati (Salerno, Italy). Food Chem. 2013, 140, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.; Dludla, P.V.; Muller, C.J.F.; Huisamen, B.; Essop, M.F.; Louw, J. The transcription profile unveils the cardio-protective effect of aspalathin against lipid toxicity in an in vitro H9c2 model. Molecules 2017, 22, 219. [Google Scholar] [CrossRef] [Green Version]
- Anupama, N.; Preetha Rani, M.R.; Shyni, G.L.; Raghu, K.G. Glucotoxicity results in apoptosis in H9c2 cells via alteration in redox homeostasis linked mitochondrial dynamics and polyol pathway and possible reversal with cinnamic acid. Toxicol. In Vitro 2018, 53, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Rein, D.; Paglieroni, T.G.; Pearson, D.A.; Wun, T.; Schmitz, H.H.; Gosselin, R.; Keen, C.L. Cocoa and wine polyphenols modulate platelet activation and function. J. Nutr. 2000, 130, 2120–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnorr, O.; Brossette, T.; Momma, T.Y.; Kleinbongard, P.; Keen, C.L.; Schroeter, H.; Sies, H. Cocoa flavanols lower vascular arginase activity in human endothelial cells in vitro and in erythrocytes in vivo. Arch. Biochem. Biophys. 2008, 476, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Actis-Goretta, L.; Ottaviani, J.I.; Keen, C.L.; Fraga, C.G. Inhibition of angiotensin converting enzyme (ACE) activity by flavan-3-ols and procyanidins. FEBS Lett. 2003, 555, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.L.; Ge, X.L.; Gao, X.Y.; Zhan, H.Y.; Shi, T.; Su, N.; Zhang, Z.Q. Two angiotensin-converting enzyme-inhibitory peptides from almond protein and the protective action on vascular endothelial function. Food Funct. 2016, 7, 3733–3739. [Google Scholar] [CrossRef] [PubMed]
- Soncini, R.; Santiago, M.B.; Orlandi, L.; Moraes, G.O.; Peloso, A.L.; dos Santos, M.H.; Alves-da-Silva, G.; Paffaro, V.A., Jr.; Bento, A.C.; Giusti-Paiva, A. Hypotensive effect of aqueous extract of Averrhoa carambola L. (Oxalidaceae) in rats: An in vivo and in vitro approach. J. Ethnopharmacol. 2011, 133, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Ronchi, S.N.; Brasil, G.A.; Nascimento, A.M.; Lima, E.M.; Scherer, R.; Costa, H.B.; Romão, W.; Boëchat, G.A.P.; Lenz, D.; Fronza, M.; et al. Phytochemical and in vitro and in vivo biological investigation on the antihypertensive activity of mango leaves (Mangifera indica L.). Ther. Adv. Cardiovasc. Dis. 2015, 9, 244–256. [Google Scholar] [CrossRef] [Green Version]
- Zarei, M.; Hejazi, S.; Javadi, S.A.; Farahani, H. The efficacy of wet cupping in the treatment of hypertension. ARYA Atheroscler. J. 2012, 8, 1–4. [Google Scholar]
- Geleta, B.; Makonnen, E.; Debella, A.; Tadele, A. In vivo antihypertensive and antihyperlipidemic effects of the crude extracts and fractions of Moringa stenopetala (Baker f.) Cufod. Leaves in rats. Front. Pharmacol. 2016, 7, 97. [Google Scholar] [CrossRef]
- Girgih, A.T.; He, R.; Malomo, S.; Offengenden, M.; Wu, J.; Aluko, R.E. Structural and functional characterization of hemp seed (Cannabis sativa L.) protein-derived antioxidant and antihypertensive peptides. J. Funct. Foods 2014, 6, 384–394. [Google Scholar] [CrossRef]
- Jordan, J. CrossTalk opposing view: Which technique for controlling resistant hypertension? Carotid sinus stimulation. J. Physiol. 2014, 592, 933–3935. [Google Scholar] [CrossRef] [Green Version]
- Menne, J.; Jordan, J.; Linnenweber-Held, S.; Haller, H. Resistant hypertension: Baroreflex stimulation as a new tool. Nephrol. Dial. Transplant. 2013, 28, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myung, S.K.; Ju, W.; Cho, B.; Oh, S.W.; Park, S.M.; Koo, B.K.; Park, B.J. Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: Systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 346, 10–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Y.F.; Sigg, D.C.; Ujhelyi, M.R.; Wilhelm, J.J.; Richardson, E.S.; Iaizzo, P.A. Pericardial delivery of omega-3 fatty acid: A novel approach to reducing myocardial infarct sizes and arrhythmias. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Jao, L.E.; Appel, B.; Wente, S.R. A zebrafish model of lethal congenital contracture syndrome 1 reveals Gle1 function in spinal neural precursor survival and motor axon arborization. Development 2012, 139, 1316–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Y.F.; Sigg, D.C.; Leaf, A. The antiarrhythmic effect of n-3 polyunsaturated fatty acids: Modulation of cardiac ion channels as a potential mechanism. J. Membr. Biol. 2005, 206, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. Effect of dietary omega-3 polyunsaturated fatty acids on heart rate and heart rate variability in animals susceptible or resistant to ventricular fibrillation. Front. Physiol. 2012, 3, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devaraj, S.; Leonard, S.; Traber, M.G.; Jialal, I. Gamma-tocopherol supplementation alone and in combination with alpha-tocopherol alters biomarkers of oxidative stress and inflammation in subjects with metabolic syndrome. Free Radic. Biol. Med. 2008, 44, 1203–1208. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Ma, C.; Han, L.; Gao, H.; Zhou, Q.; Yang, M.; Chen, C.; Deng, Q.; Huang, Q.; Huang, F. Optimized rapeseed oils rich in endogenous micronutrients ameliorate risk factors of atherosclerosis in high fat diet fed rats. Lipids Health Dis. 2014, 13, 166. [Google Scholar] [CrossRef] [Green Version]
- Zarei, M.; Forghani, B.; Ebrahimpour, A.; Abdul-Hamid, A.; Anwar, F.; Saari, N. In vitro and in vivo antihypertensive activity of palm kernel cake protein hydrolysates: Sequencing and characterization of potent bioactive peptides. Ind. Crops Prod. 2015, 76, 112–120. [Google Scholar] [CrossRef]
- Sun, Y.Q.; Xin, T.A.O.; Men, X.M.; Xu, Z.W.; Tian, W.A.N.G. In vitro and in vivo antioxidant activities of three major polyphenolic compounds in pomegranate peel: Ellagic acid, punicalin, and punicalagin. J. Integr. Agric. 2017, 16, 1808–1818. [Google Scholar] [CrossRef] [Green Version]
- Smoliga, J.M.; Vang, O.; Baur, J.A. Challenges of translating basic research into therapeutics: Resveratrol as an example. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2012, 67, 158–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaldo, L.; Narváez, A.; Izzo, L.; Graziani, G.; Gaspari, A.; Minno, G.D.; Ritieni, A. Red Wine Consumption and Cardiovascular Health. Molecules 2019, 24, 3626. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Wright, M.; Gomez-Gracia, E. Development of a short dietary intake questionnaire for the quantitative estimation of adherence to a cardioprotective Mediterranean diet. Eur. J. Clin. Nutr. 2004, 58, 1550–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stull, A.; Cash, K.; Champagne, C.; Gupta, A.; Boston, R.; Beyl, R.; Cefalu, W.T. Blueberries improve endothelial function, but not blood pressure, in adults with metabolic syndrome: A randomized, double-blind, placebo-controlled clinical trial. Nutrients 2015, 7, 4107–4123. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Du, M.; Leyva, M.J.; Sanchez, K.; Betts, N.M.; Wu, M.; Lyons, T.J. Blueberries decrease cardiovascular risk factors in obese men and women with metabolic syndrome. J. Nutr. 2010, 140, 1582–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goszcz, K.; Duthie, G.G.; Stewart, D.; Leslie, S.J.; Megson, I.L. Bioactive polyphenols and cardiovascular disease: Chemical antagonists, pharmacological agents or xenobiotics that drive an adaptive response? Br. J. Pharmacol. 2017, 174, 1209–1225. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sandoo, A.; van Zanten, J.J.C.V.; Metsios, G.S.; Carroll, D.; Kitas, G.D. The endothelium and its role in regulating vascular tone. Open Cardiovasc. Med. J. 2010, 4, 302–312. [Google Scholar] [CrossRef]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.A.; de la Torre, R.; Corella, D.; Lamuela-Raventós, R.M. Inverse association between habitual polyphenol intake and incidence of cardiovascular events in the PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 639–647. [Google Scholar] [CrossRef]
- Asgary, S.; Sahebkar, A.; Afshani, M.R.; Keshvari, M.; Haghjooyjavanmard, S.; Rafieian-Kopaei, M. Clinical evaluation of blood pressure lowering, endothelial function improving, hypolipidemic and anti-inflammatory effects of pomegranate juice in hypertensive subjects. Phytother. Res. 2014, 28, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Dohadwala, M.M.; Holbrook, M.; Hamburg, N.M.; Shenouda, S.M.; Chung, W.B.; Titas, M.; Vita, J.A. Effects of cranberry juice consumption on vascular function in patients with coronary artery disease. Am. J. Clin. Nutr. 2011, 93, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Artero, A.; Artero, A.; Tarín, J.J.; Cano, A. The impact of moderate wine consumption on health. Maturitas 2015, 80, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Berglund, L.; Anuurad, E. Role of lipoprotein (a) in cardiovascular disease. J. Am. Coll. Cardiol. 2008, 52, 132–134. [Google Scholar] [CrossRef] [Green Version]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Estruch, R. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef]
- Borriello, A.; Cucciolla, V.; Della Ragione, F.; Galletti, P. Dietary polyphenols: Focus on resveratrol, a promising agent in the prevention of cardiovascular diseases and control of glucose homeostasis. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 618–625. [Google Scholar] [CrossRef]
- Zordoky, B.N.M.; Robertson, I.M.; Dyck, J.R.B. Preclinical and clinical evidence for the role of resveratrol in the treatment of cardiovascular diseases. Biochem. Biophys. Acta 2015, 1852, 1155–1177. [Google Scholar] [CrossRef] [Green Version]
- Fitó, M.; Cladellas, M.; de la Torre, R.; Martí, J.; Alcántara, M.; Pujadas-Bastardes, M.; Covas, M.I. Antioxidant effect of virgin olive oil in patients with stable coronary heart disease: A randomized, crossover, controlled, clinical trial. Atherosclerosis 2005, 181, 149–158. [Google Scholar] [CrossRef]
- Aguilera, C.M.; Mesa, M.D.; Ramirez-Tortosa, M.C.; Nestares, M.T.; Ros, E.; Gil, A. Sunflower oil does not protect against LDL oxidation as virgin olive oil does in patients with peripheral vascular disease. Clin. Nutr. 2004, 23, 673–681. [Google Scholar] [CrossRef]
- Griel, A.E.; Kris-Etherton, P.M. Tree nuts and the lipid profile: A review of clinical studies. Br. J. Nutr. 2006, 96, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Damasceno, N.R.T.; Pérez-Heras, A.; Serra, M.; Cofán, M.; Sala-Vila, A.; Salas-Salvadó, J.; Ros, E. Crossover study of diets enriched with virgin olive oil, walnuts or almonds. Effects on lipids and other cardiovascular risk markers. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Jayalath, V.H.; de Souza, R.J.; Sievenpiper, J.L.; Ha, V.; Chiavaroli, L.; Mirrahimi, A.; Jenkins, D.J.A. Effect of dietary pulses on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Am. J. Hypertens. 2014, 27, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Nouri, F.; Sarrafzadegan, N.; Mohammadifard, N.; Sadeghi, M.; Mansourian, M. Intake of legumes and the risk of cardiovascular disease: Frailty modeling of a prospective cohort study in the Iranian middle-aged and older population. Eur. J. Clin. Nutr. 2016, 70, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Thompson, A.M.; Tees, M.T.; Nguyen, C.H.; Winham, D.M. Non-soy legume consumption lowers cholesterol levels: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 94–103. [Google Scholar] [CrossRef] [Green Version]
- He, M.; van Dam, R.M.; Rimm, E.; Hu, F.B.; Qi, L. Whole-grain, cereal fiber, bran, and germ intake and the risks of all-cause and cardiovascular disease-specific mortality among women with type 2 diabetes mellitus. Circulation 2010, 121, 2162–2168. [Google Scholar] [CrossRef] [Green Version]
- Tighe, P.; Duthie, G.; Vaughan, N.; Brittenden, J.; Simpson, W.G.; Duthie, S.; Thies, F. Effect of increased consumption of whole-grain foods on blood pressure and other cardiovascular risk markers in healthy middle-aged persons: A randomized controlled trial. Am. J. Clin. Nutr. 2010, 92, 733–740. [Google Scholar] [CrossRef]
- Roncaglioni, M.C.; Tombesi, M.; Avanzini, F.; Barlera, S.; Caimi, V.; Longoni, P.; Marzona, I.; Milani, V.; Silletta, M.G.; Tognoni, G. n-3 fatty acids in patients with multiple cardiovascular risk factors. N. Engl. J. Med. 2013, 368, 1800. [Google Scholar]
- Kwak, S.M.; Myung, S.K.; Lee, Y.J.; Seo, H.G.; Korean Meta-analysis Study Group. Efficacy of omega-3 fatty acid supplements (eicosapentaenoic acid and docosahexaenoic acid) in the secondary prevention of cardiovascular disease: A meta-analysis of randomized, double-blind, placebo-controlled trials. Arch. Intern. Med. 2012, 172, 686–694. [Google Scholar]
- Burr, M.L.; Gilbert, J.; Holliday, R.A.; Elwood, P.; Fehily, A.; Rogers, S.; Sweetnam, P.; Deadman, N. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: Diet and reinfarction trial (DART). Lancet 1989, 334, 757–761. [Google Scholar] [CrossRef]
- Investigators, G.-P. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: Results of the GISSI-Prevenzione trial. Lancet 1999, 354, 447–455. [Google Scholar] [CrossRef]
- Tavazzi, L.; Maggioni, A.P.; Marchioli, R.; GISSI-HF investigators. Effect of n-3 polyunsaturated fatty acids in patients with chronic heart failure (the GISSI-HF trial): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): A randomised open-label, blinded endpoint analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef]
- Rizos, E.C.; Ntzani, E.E.; Bika, E.; Kostapanos, M.S.; Elisaf, M.S. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: A systematic review and meta-analysis. JAMA 2012, 308, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, D.; Giltay, E.J.; Geleijnse, J.M. n–3 Fatty acids and cardiovascular events after myocardial infarction. N. Engl. J. Med. 2010, 363, 2015–2026. [Google Scholar] [CrossRef] [PubMed]
- Rauch, B.; Schiele, R.; Schneider, S.; Diller, F.; Victor, N.; Gohlke, H.; Gottwik, M.; Steinbeck, G.; Del Castillo, U.; Sack, R. OMEGA, a randomized, placebo-controlled trial to test the effect of highly purified omega-3 fatty acids on top of modern guideline-adjusted therapy after myocardial infarction. Circulation 2010, 122, 2152–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galan, P.; Kesse-Guyot, E.; Czernichow, S.; Briancon, S.; Blacher, J.; Hercberg, S. Effects of B vitamins and omega 3 fatty acids on cardiovascular diseases: A randomised placebo controlled trial. BMJ 2010, 341, c6273. [Google Scholar] [CrossRef] [Green Version]
- Investigators, O.T. n–3 fatty acids and cardiovascular outcomes in patients with dysglycemia. N. Engl. J. Med. 2012, 367, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Aung, T.; Haynes, R.; Barton, J.; Cox, J.; Murawska, A.; Murphy, K.; Lay, M.; Armitage, J.; Bowman, L. Cost-effective recruitment methods for a large randomised trial in people with diabetes: A Study of Cardiovascular Events iN Diabetes (ASCEND). Trials 2016, 17, 286. [Google Scholar] [CrossRef] [Green Version]
- Group, A.S.C. Effects of aspirin for primary prevention in persons with diabetes mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Manson, J.E.; Bassuk, S.S.; Lee, I.-M.; Cook, N.R.; Albert, M.A.; Gordon, D.; Zaharris, E.; MacFadyen, J.G.; Danielson, E.; Lin, J. The VITamin D and OmegA-3 TriaL (VITAL): Rationale and design of a large randomized controlled trial of vitamin D and marine omega-3 fatty acid supplements for the primary prevention of cancer and cardiovascular disease. Contemp. Clin. Trials 2012, 33, 159–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keaney, J.F.; Rosen, C.J. VITAL signs for dietary supplementation to prevent cancer and heart disease. N. Engl. J. Med. 2019, 380, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Burr, M.L.; Ashfield-Watt, P.A.; Dunstan, F.D.J.; Fehily, A.M.; Breay, P.; Ashton, T.; Zotos, P.C.; Haboubi, N.A.; Elwood, P.C. Lack of benefit of dietary advice to men with angina: Results of a controlled trial. Eur. J. Clin. Nutr. 2003, 57, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Cardiovascular Risk Factor | Pathophysiology | Benefit | Ref |
|---|---|---|---|
| sedentary lifestyle | ↑ insulin resistance, ↑ obesity, ↑blood glucose levels, ↑plasma lipids, ↑prothrombotic factors | lifestyle changes: physical activity lowers risk for CVDs mortality ↑physical activity, ↓ alcohol consumption, not smoking, ↓ obesity: ↓ risk of incident heart failure in 50% cases | [31] [32] |
| hypertension | ↑arterial hypertension and endothelial growth factor-linked polymorphisms, ↑vascular damage | berberine, green tea, cocoa, lycopene, aged garlic extract, resveratrol, grape seed extract, beetroot juice, olive oil and ascorbic acid: ↓blood pressure. apricot and olive seed protein hydrolysates: ↓ACE Resveratrol: ↑ nitric oxid production, ↑vasodilatation | [36] [37] |
| smoking | ↑oxidative stress, ↑coronary spasm, disorders of coagulation mechanisms, ↑platelet aggregation, fibrinogen growth, disorders of endothelial function ↑ LDLc, ↓ HDL | garlic extract, Angelica gigas, celery, Artemisiae annuae Herba, oat extracts, cinnamon, soy extracts, hibiscus, flaxseed, wolfberry, lycopene, basil, and cocoa ↓atherosclerosis proanthocyanins (bilberries): anti-inflammatory effect, ↓pro-inflammatory cytokines, ↓chemokines (TNFα, IL-1, IL-6, IL-8) | [49] [44] |
| stress | disturbance of the hypothalamo-pituitary-adrenal axis, ↑serum cortisol due to stress, ↑inflammation of the arterial (endothelial) wall, ↑atherosclerosis, ↑ tone of the sympathetic vegetative nervous system. | L-theanine from green tea: ↑relaxation, ↓post-stress cortisol hyperforin: ↑serotonin in brain, similar to antidepressant drugs ginseng: antistress action, ↓physical and mental fatigue, ↑ power of concentration, ↑memory, ↑work performance | [61] [62] |
| obesity | ↑dyslipidemia, hypercoagulability, platelet dysfunction, ↑insulin resistance and type 2 diabetes, ↑inflammation | polyphenols (grapes, tea, ginseng, red to purple color fruits) benefits: ↓platelet aggregation, ↓vascular inflammation, ↓apoptotis, ↓LDL oxidation EPA and DHA: anti-inflammatory and cardioprotective effects carotenoids: ↑anti-oxidant potential resveratrol: ↓fat deposits, regulate insulin levels, ↓body weight, ↑SIRT 1 protein | [19] [79,80,81] [23] |
| diabetes | altering arterial walls increasing inflammation at the endothelial level, with the deposition of VLDL and LDL cholesterol particles at this level and the formation of atheroma plaque | mediterranean diet: ↓ risk of diabetes polyphenols, flavonoids, terpenoids, saponins and lignans: antihyperglycemic effect peptides (soybean): prevent T2D onset | [86] [110] [111] |
| dyslipidemia | increasing of atherogenic effect deposits of atheroma plaques on the internal walls of medium and large arteries, with thickening of the arterial wall and loss of elasticity | phenolic compounds, flavonols: ↓TC, ↓LDLc, ↓TG levels phytosterols: ↓LDLc Soybean components, both proteins and isoflavones: ↓LDLc, ↑HDLc | [119] [120] [121] [127] [128] |
| Plant-Food Bioactive Compounds | Clinical Study | Results | Ref |
|---|---|---|---|
| polyphenols (anthocyanins) | observational study on three groups of patients with CVDs consuming mediterranean diet | ↑endothelial function and plasma lipid profiles ↓abnormal platelet aggregation, ↓oxidative stress | [185] [186] [187] [189] |
| pomegranate juice (anthocyanins, catechins, quercetin, rutin, ellagitannins) | single-blind study for hypertensive men | ↓blood pressure due to its ACE activity antioxidant activity: due to the radical scavenging effect of anthocyanins and hydrolysable tannins | [190] |
| cranberry juice (anthocyanins, polyphenols) | a placebo-controlled crossover study in patients with coronary artery disease | ↓carotid femoral pulse wave velocity only acute benefit but not a chronic effect on endothelial vasodilator function | [132] [191] |
| anthocyanins | a clinical study in hypertensive patients | anthocyanins did not exhibit anti-hypertensive activity in borderline hypertensive men | [132] |
| blueberries | a double-blind, placebo-controlled study in subjects with metabolic syndrome | blueberries did not affect blood pressure and insulin sensitivity ↑endothelial function | [184] |
| red wine (resveratrol) | randomized clinical trial | the ethanolic part of wine: ↑protective effect on the lipid profile phenolic compounds of wine: ↓lipoprotein plasma concentrations by 12%, ↓lipid peroxidation, ↓ blood pressure, ↓ serum cholesterol, ↓platelet aggregation endothelial cells protection against apoptosis | [194] [193] [195] [196] |
| virgin olive oil (oleuropein, tyrosol, hydroxytyrosol, monounsaturated fatty acids) | randomized, crossover controlled clinical trial in hypertensive patients | ↓ systolic blood pressure, ↓ diastolic blood pressure, glucose, ↓lipids antibodies against oxidized LDL did not change olive oil phenolics counteracted LDL oxidation due to both metals and radicals and acted as chain-breaking antioxidants for lipid peroxidation ↑HDL, ↓LDL | [174] |
| sunflower-oil (vitamin E) | clinical study of Spanish male patients with peripheral vascular disease | sunflower-oil-enriched diets didn’t protect LDL against oxidation | [198] |
| nuts (unsaturated omega-3 fatty acids, dietary fibers, vitamin E, potassium and magnesium) | randomized crossover study | ↓ blood cholesterol ↓ LDL-cholesterol ↓TC, ↓LDL/HDL ratios | [199] [200] |
| vegetables (fibre, plant protein, K) | randomized controlled clinical trial in patients with diabetes, metabolic syndrome without apparent disease | ↑antioxidant response, ↓oxidized LDLc ↓blood pressure, ↓TC, ↓LDLc | [201] [202] [203] |
| whole-grain food (fibre, vitamins, minerals, phenolic compounds, phytoestrogens) | a clinical trial with 233 middle-aged, healthy, overweight men and women | ↓serum lipids, ↓blood pressure, ↑endothelial function, ↓oxidative stress, ↓inflammation, ↓systolic blood pressure triglycerides, HDL, and apolipoprotein A1 concentrations did not change ↓ total cholesterol, ↓LDL-cholesterol | [205] [204] |
| unsaturated omega-3 fatty acids | secondary prevention trial performed on post-myocardial infarction patients (DART) | total CV mortality ↓of 29% and a re-infarction of 32%. | [208] |
| preventive clinical trial patients after myocardial infarction (GISSI-Prevenzione trial) | EPA + DHA reduced cardiovascular mortality by 30%, coronary mortality by 35% and sudden death by 45%.; the effects occurred early (90 days for total mortality and 120 days for sudden death) and were 4 times stronger in patients with an ejection fraction below 40% | [209] | |
| large-scale, randomized, double-blind clinical study (GISSI Heart Failure) | omega-3 fatty acids reduced cardiovascular mortality by 10%, sudden death by 7% and re-admission for ventricular arrhythmias by 28% | [210] | |
| hypercholesterolemic patients prospective, randomized, open-label study (JELIS) | the sudden cardiac death, myocardial infarction, unstable angina and revascularization procedures, were reduced by 19% | [211] | |
| a multicenter, randomized, placebo-controlled study in post-myocardial infarction patients (Alpha Omega) | dietary supplementation with ω3-PUFAs did not reduce the incidence of major ischemic or non-ischemic cardiovascular events, sudden cardiac death or interventions such as angioplasty or aortocoronary bypass | [213] | |
| randomized, placebo-controlled, double-blind, multicenter trial included patients after myocardial infarction (OMEGA) | dietary supplementation with ω3-PUFAs has no additional beneficial effect compared to standard acute myocardial infarction therapy on overall mortality, the incidence of major cardio- or cerebrovascular events, or sudden cardiac death. | [214] | |
| randomized double-blind, placebo-controlled secondary-prevention trial in patients with myocardial infarction, ischemic stroke, or unstable angina (SU.FOL.OM3) | no reduction of cardiovascular risks in patients with a history of coronary heart disease or ischemic stroke. | [215] | |
| randomized clinical trial in people at high risk of cardio- vascular disease and diabetes, impaired glucose tolerance or impaired fasting blood glucose (ORIGIN) | the study did not show a statistically significant reduction in overall mortality, major cardiovascular events, or mortality due to arrhythmia. | [216] | |
| randomized trial in participants with stable angina (DART2) | increased consumption of polyunsaturated fatty acid supplements was not beneficial in reducing cardiac deaths or sudden cardiac death, the use of fruits, vegetables and oats has no positive effect on cardiovascular risk factors | [208] | |
| randomized controlled clinical trial in patients with diabetes, but without a history of cardiovascular disease (ASCEND) | the study did not show a decrease in mortality | [218] | |
| a multicenter, randomized, double-blind controlled trial in patients with cardiovascular risk factors (diabetes) or cardiovascular disease (REDUCE-IT) | patients with hypertriglyceridemia recorded decreases in cardiovascular events compared to the placebo group major such as stroke or stroke (25%) and cardiovascular death (20%) in patients with another cardiovascular risk factor (diabetes mellitus), but without a major cardiovascular event, supplementation was not effective. It does not prevent heart attack or stroke | [219] | |
| a randomized, placebo-controlled trial study (VITAL) | no reductions in strokes, CVDs mortality, cancer incidence, cancer mortality or all- cause mortality | [220] [221] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharifi-Rad, J.; Rodrigues, C.F.; Sharopov, F.; Docea, A.O.; Can Karaca, A.; Sharifi-Rad, M.; Kahveci Karıncaoglu, D.; Gülseren, G.; Şenol, E.; Demircan, E.; et al. Diet, Lifestyle and Cardiovascular Diseases: Linking Pathophysiology to Cardioprotective Effects of Natural Bioactive Compounds. Int. J. Environ. Res. Public Health 2020, 17, 2326. https://doi.org/10.3390/ijerph17072326
Sharifi-Rad J, Rodrigues CF, Sharopov F, Docea AO, Can Karaca A, Sharifi-Rad M, Kahveci Karıncaoglu D, Gülseren G, Şenol E, Demircan E, et al. Diet, Lifestyle and Cardiovascular Diseases: Linking Pathophysiology to Cardioprotective Effects of Natural Bioactive Compounds. International Journal of Environmental Research and Public Health. 2020; 17(7):2326. https://doi.org/10.3390/ijerph17072326
Chicago/Turabian StyleSharifi-Rad, Javad, Célia F. Rodrigues, Farukh Sharopov, Anca Oana Docea, Aslı Can Karaca, Mehdi Sharifi-Rad, Derya Kahveci Karıncaoglu, Gözde Gülseren, Ezgi Şenol, Evren Demircan, and et al. 2020. "Diet, Lifestyle and Cardiovascular Diseases: Linking Pathophysiology to Cardioprotective Effects of Natural Bioactive Compounds" International Journal of Environmental Research and Public Health 17, no. 7: 2326. https://doi.org/10.3390/ijerph17072326