1. Introduction
Prostate cancer (PCa) is the most frequent cancer and the leading cancer-related cause of death in African men [
1]. Early-stage PCa is often asymptomatic or shares symptoms of benign prostatic hyperplasia. Due to the lack of screening and public awareness of prostate diseases in Africa, PCa is discovered at advanced stages [
2]. In Senegal, of over 60% of patients affected with advanced cancer, only less than 40% are a treatable form of localized disease [
3,
4], a stark contrast to the USA where about 89% of PCa cases are diagnosed early [
5]. Alas, the 5-year survival rate after diagnosis hovers around 30% in Senegal [
4], versus 98% in the USA [
5].
Once diagnosed, early stage PCa is a treatable disease. The primary treatment option is total surgical resection via radical prostatectomy, which is available in Senegal. The ultimate key to PCa diagnosis is core tissue biopsy (PBx). This procedure has evolved since the early 1990s and is well standardized [
6]. PBx is usually performed transrectally under local anesthesia, with transrectal ultrasound (TRUS) imaging guidance, and it is well tolerated [
7,
8]. Bleeding is the most frequent side effect, usually resolved naturally while infection is suppressed with antimicrobial prophylaxis [
9]. In addition to cancer detection, prostate biopsy plays a crucial role in grading the disease and making treatment decisions. While PBx is universally available in North America, in Senegal it is only offered in a small number of hospitals in the capital, Dakar, where trained urologists and pathologists, and the requisite equipment, are available. Of the 16 million inhabitants of Senegal, about 3.5 million people living in the Dakar metropolitan area have “geographical access” to advanced urological services. In the Dakar region however, many patients still cannot get a prostate biopsy, because the waiting lists are too long in the public clinics and the procedure is prohibitively expensive in the private clinics.
Transrectal ultrasound-guided PBx is difficult to perform; simultaneous imaging, anatomical interpretation and placement of the biopsy needle requires extensive training and experience. Ultrasound offers poor imaging of the prostate anatomy zones and low sensitivity in showing PCa foci growing in these zones. Altogether, standard PBx suffers from a low diagnostic yield (~40%), high false negative rates [
7,
10], and cancer lesions as large as half a sugar cube (0.5 cc, the smallest clinically significant prostate cancer [
11]), are often missed. The outcomes are worse in Senegal, where it is reported that among all patients referred for PBx, cancer was found in only 30%, even though over 60% of Senegalese patients have advanced disease [
12], showing the need for improvements in how the biopsy procedure is delivered in Senegal. In high-income countries, “fusion biopsy”, also known as “real-time virtual sonography” (i.e., spatial navigation that registers ultrasound with multi-parametric MRI), has emerged as a method for improving prostate biopsy [
13,
14]. This approach is not feasible in West Africa, where fewer than 40 high-field MRI units serve a population larger than North America, with Senegal having just 2 suitable MRI units [
15]. There is a critical need to address the lack of availability and the quality of prostate cancer biopsy in Senegal, with high reward from doing so: the ability to diagnose prostate cancer early will shift clinical practice and allow us to cure many patients who will eventually succumb to terminal cancer.
Our objective is to create a prostate biopsy system, herein named NaviPBx, that visualizes cancer-suspicious locations highlighted in multiparametric transrectal ultrasound imaging, and allows for the real-time navigation of the biopsy needle to ensure the accurate targeting of potential lesions, and the extensive evaluation of its feasibility, usability and scalability. The essence of our innovation lies in combining low cost with functionality and usability, optimized for conditions in Senegal, yielding a system with functionality and technical performance comparable with state-of-the-art fusion biopsy systems, at a fraction of the cost. Our technical approach concentrates on “frugal technology”, intended to be affordable in Senegal and generally for low–middle income (LMIC) countries.
We will integrate techniques, the clinical effectiveness of which have been extensively validated in peer-reviewed literature, resulting in a system that promises to enable the first national-level implementation of an image-guided intervention program based entirely on free, open-source software. NaviPBx is set to be implemented nationwide through the Senegalese Military Health Service, in a total of ten hospitals across the country, in which over 90% of the patients are civilians with no connection to the military.
2. System Design and Architecture
2.1. System Design
We aim to create a prostate biopsy system that visualizes cancer-suspicious target locations highlighted in multiparametric transrectal ultrasound imaging, and facilitates real-time navigation of the biopsy needle to allow for the systematic and targeted sampling of possible prostate cancer locations. We derive the proposed system from the current most advanced implementation of PBx, “fusion biopsy” (a.k.a. “real-time virtual sonography”), which entails the registration of MRI and TRUS [
13,
14]. The main advantages of MRI lie in two key functions for determining and accessing the biopsy targets: (1) showing the intraprostatic anatomy for systematic sampling and (2) showing cancer-suspicious locations for additional sampling. The real-time tracking of the TRUS probe enables the fusion action, allowing the physician to navigate the biopsy needle to the desired biopsy target locations without having to mentally interpret low-quality live 2D TRUS images. As MRI is scarcely available in Senegal, our research strategy is to develop a PBx system that provides most of the benefits of fusion biopsy without using MRI, while retaining the same physical layout, anatomical access, and overall workflow. We will use spatially navigated, multiparametric, transrectal ultrasound imaging to solve this problem. In doing so, we will adopt methods whose clinical utility have been extensively evaluated in the peer-reviewed literature.
As envisioned, NaviPBX will have about the same overall functionality as other commercial fusion biopsy systems (e.g., UroNav), except in NaviPBX the pre-operative multi-parametric MRI imaging will be replaced with multi-parametric ultrasound imaging. Unfortunately, ultrasound will no doubt be inferior to MRI, but it is our only viable prostate imaging option in Senegal. Additionally, NaviPBX will not involve a separate MR imaging session. This is a significant disadvantage in Senegal, where deep-routed sociocultural reflexes hinder public discourse about genitourinary diseases and, as a result, discourage men from seeking treatment for prostate disease.
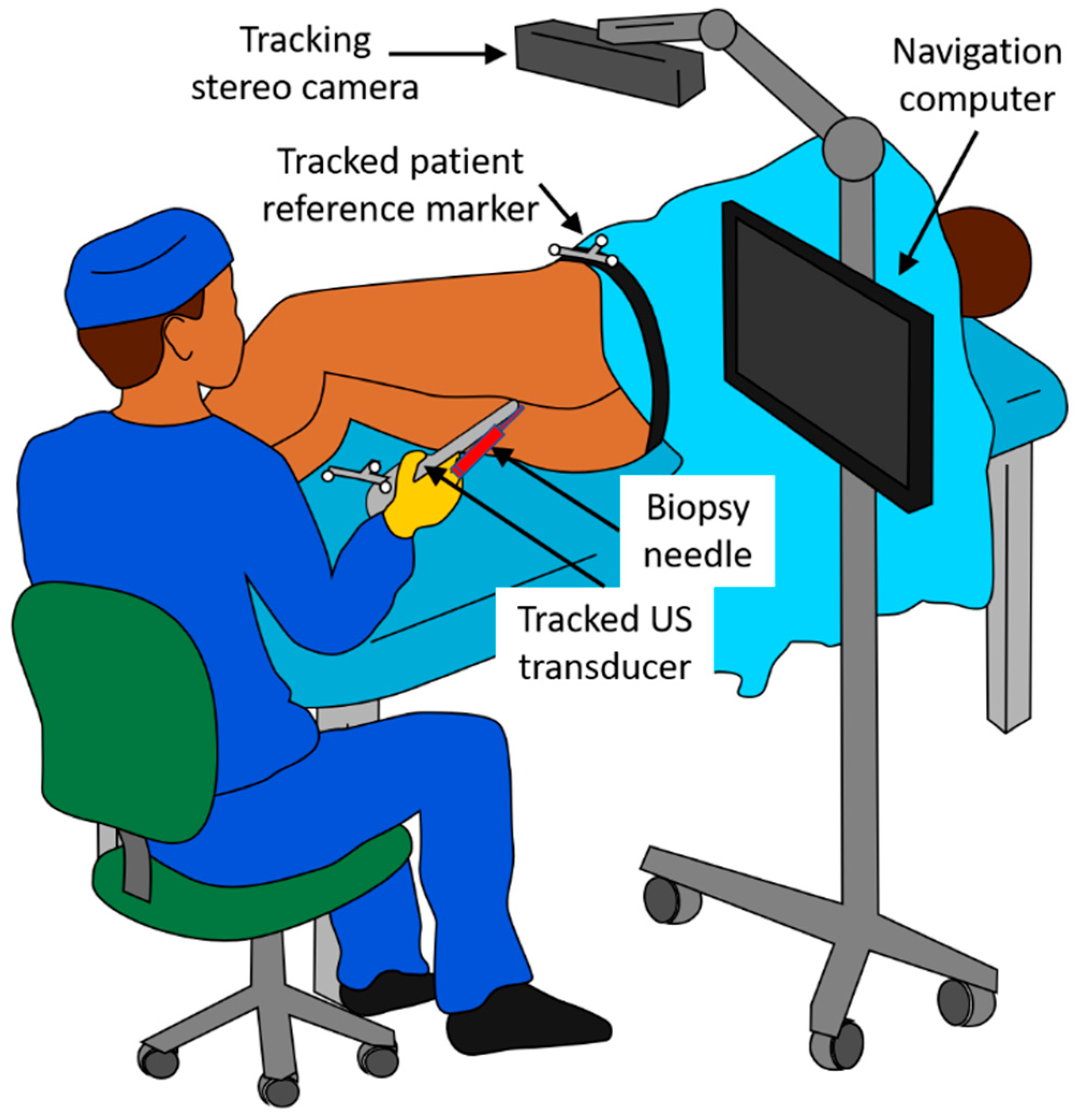
NaviPBx is envisioned as shown in
Figure 1. The patient is in the lateral decubitus position, slightly pulled up with their knees bent and rectum cleansed, the most common approach to PBx. (The alternative would be transperineal PBx performed under full or lumbar anesthesia with extensive special hardware, altogether impractical). A sterile latex cover filled with coupling gel is used for the TRUS probe. A standard sterile biopsy needle guide is clipped on the TRUS probe. An optical stereo tracking camera is mounted over the scene. Optical tracking has been used reliably for decades in surgical navigation systems, which are constantly improving and becoming less expensive. Optical tracking markers are reusable and inexpensive to manufacture locally. (The alternative would be electromagnetic (EM) tracking, used in the current commercial fusion biopsy systems. While EM does not require a clear line of sight, it has numerous drawbacks. It is adversely affected by metal objects and electric currents and is expensive and difficult to resupply in Senegal. Current EM tracking systems are produced by one company monopolizing the market, having kept both the price and technology stagnant for over a decade). Standard optical markers are clipped onto the transducer and attached onto the patient’s hip, allowing the live TRUS image to be tracked with respect to the patient. There is an un-obstructed line of sight for the tracking camera; no drapes, tools or persons obstruct the view. The biopsy needle guide and the tracking markers are attached to the TRUS transducer reproducibly and always in the same position. The transducer is delicately inserted into the rectum, rotated, and translated while observing the ultrasound image on the screen.
According to our design, the physician is assisted by two key system functions in determining the biopsy target positions. Firstly, to observe the intraprostatic anatomy for systematic sampling, the physician begins with an exploratory TRUS scan of the prostate. NaviPBx records the images and compounds a 3D TRUS volume. It is worth noting that 3D TRUS is used in the same manner in all fusion biopsy systems, e.g., Philips UroNav, Eigen Artemis™, and KOELIS Trinity
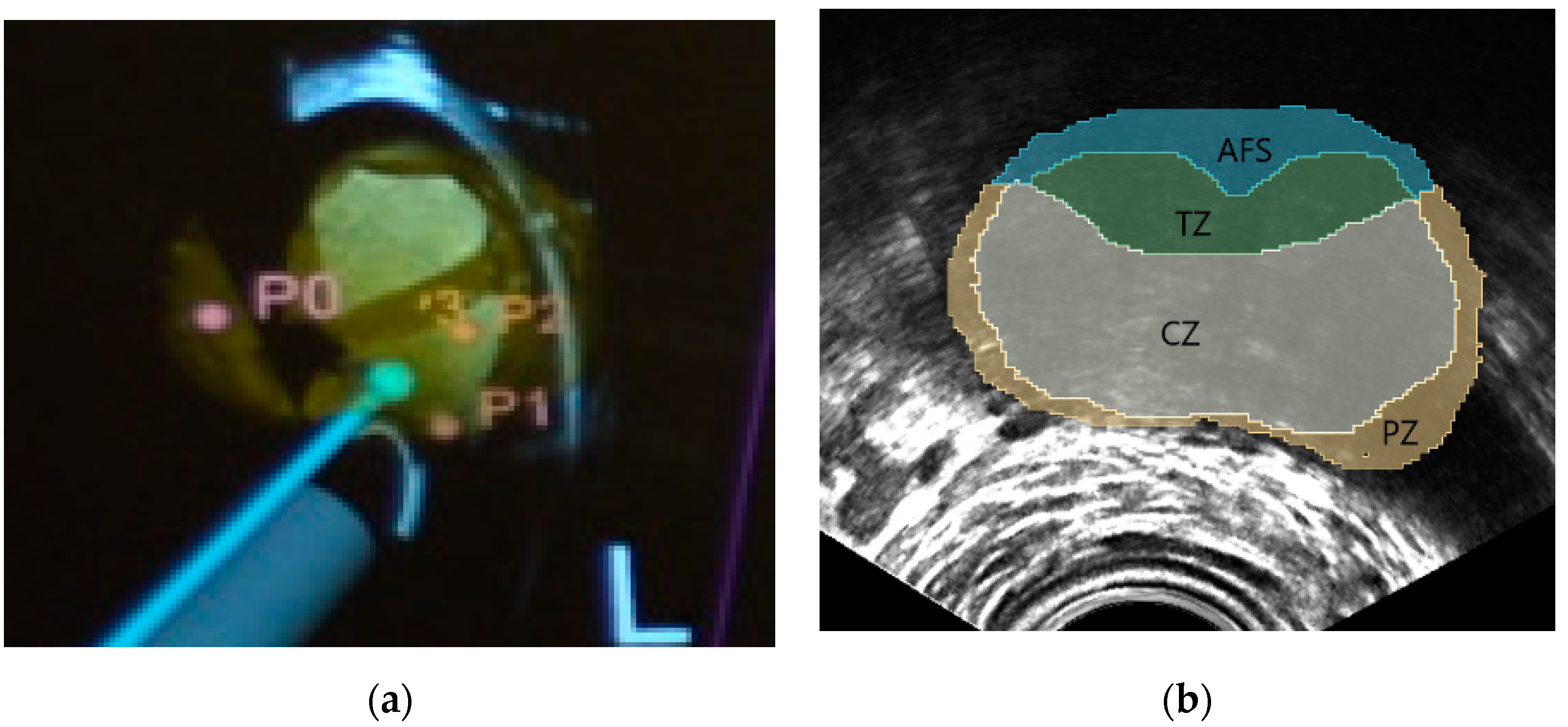
®, and thoroughly validated in the peer-reviewed clinical literature. NaviPBx automatically segments the prostate gland and computes a map of the intraprostatic McNeal zonal anatomy [
16], based on which it computes the systematic target locations (typically 12 cores), according to convention [
7]. A standard biopsy needle is inserted into the guide channel for harvesting the samples. The physician manipulates the transducer in the rectum, assisted by real-time “labels” painted over the live 2D TRUS image, e.g., current biopsy needle path, prostate gland, McNeal zonal anatomy map, and the preplanned systematic biopsy locations (
Figure 1). As the transducer displaces and deforms the prostate gland, NaviPBx automatically adjusts the labels on the live 2D TRUS image. Secondly, to show the cancer-suspicious locations for additional sampling, multiparametric transrectal ultrasound (mpTRUS) imagery is constructed from multiple ultrasound modalities (B-mode, elasticity, and Doppler). In the peer-reviewed literature, each of these modalities has been proven to contribute to recognizing PCa. With the use of 3D tracking, NaviPBx constructs a hyperdimensional image array from the available component ultrasound modalities, allowing for the analysis and visualization of them together in 3D. Finally, NaviPBx provides a variety of measurement tools to complete the diagnostic picture: dimensions, volume, shape and symmetry of the prostate; integrity of the prostate capsule; echogenicity of each McNeal zone; presentation (dimensions, symmetry, and angulation) of the seminal vesicles; presentation of the ampullae of the ducti deferens; stiffened areas quantified in elasticity imaging; and vascularization measured in Doppler imaging. We plan for these measurements to be made offline, conveniently after the biopsy in the compounded mpTRUS volume.
2.2. System Architecture
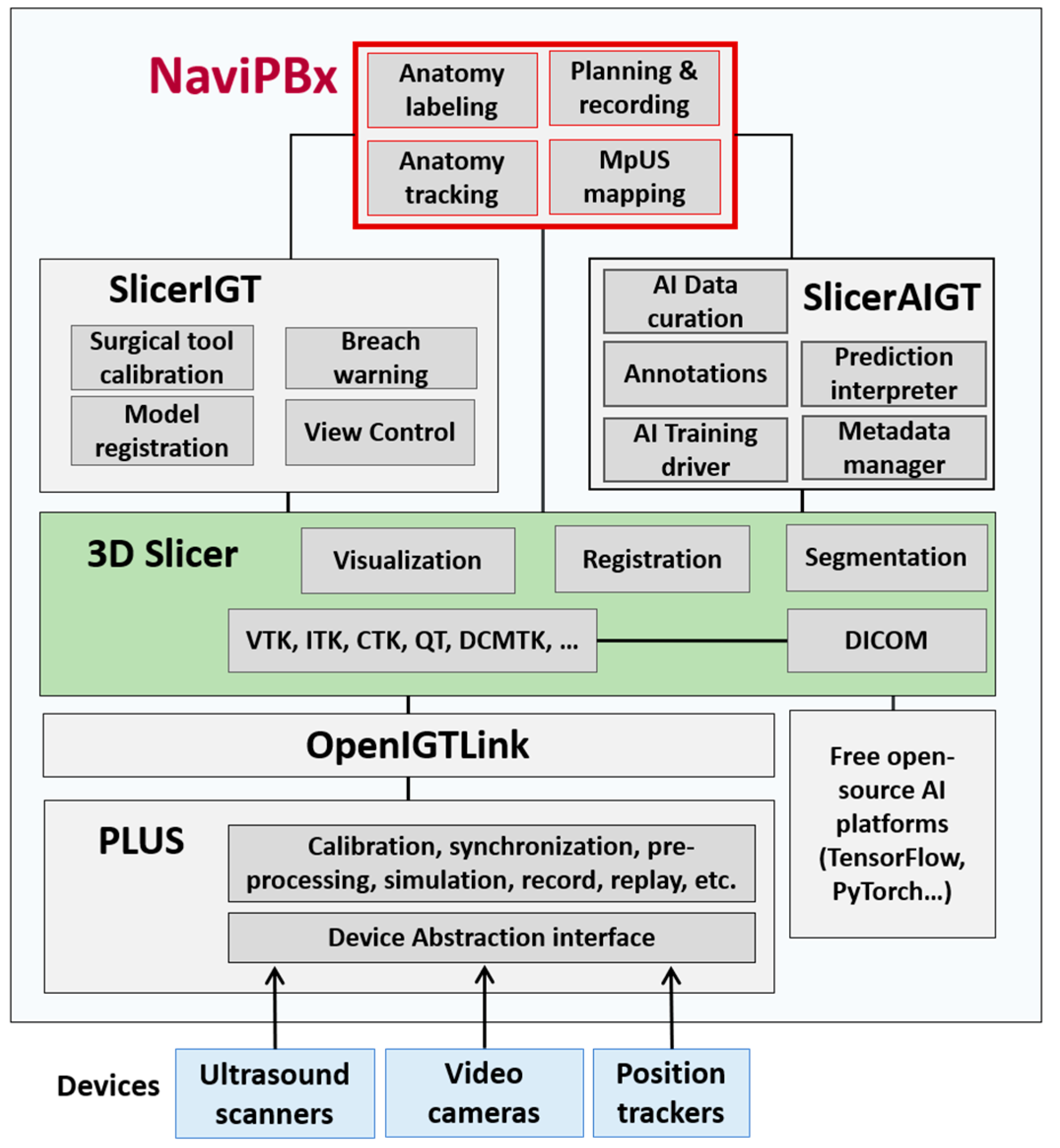
NaviPBx (
Figure 2) builds from the software 3D Slicer (
www.slicer.org (accessed on 8 August 2021)), a free, open-source software ecosystem for multimodal medical image analysis and visualization, simultaneously extended for image-guided interventions [
17].
The software, 3D Slicer, facilitates the exploration, evaluation and clinical translation of novel methods by freeing researchers from recurring tasks. The software offers thousands of features through 81 core modules and 156 extension packages. It follows a modular design, where each module is a feature-complete functional unit. Generic functions (e.g., image import/export, segmentation, and registration) used in most clinical applications are grouped in the 3D Slicer core. Domain-specific features, such as image-guided therapy and interventions, are packaged in dynamically loadable extensions, allowing users to “cherry pick” features from multiple extensions, without programming overhead. The extensions of 3D Slicer, and the software itself, run on all three major operating systems without hardware dependency. Developed since 1998 by a worldwide developer community with over 2000 years of FTE effort, 3D Slicer has become the leading open-source software resource in its field. Cumulative downloads of 3D Slicer resources have surpassed one million, and its current download rate is 400 times per day.
The Public Library for Ultrasound Toolkit (PLUS,
www.PlusToolkit.org (accessed on 8 August 2021)) [
18] is an abstraction layer for hardware devices, e.g., ultrasound scanners, position tracking devices, cameras, and generally any kind of data-streaming device. PLUS provides generic functions for pre-processing, such as the 3D ultrasound volume compounding [
19] and live volume rendering [
20] of tracked ultrasound image streams. PLUS offers complete end-user software applications for spatial and temporal calibration, an essential toolset in clinical translation and system maintenance. PLUS allows for seamlessly changing hardware devices without any change to the rest of the system. Additionally, PLUS supports the simultaneous running of multiple data streamers, a function often used to run multiple tracking devices simultaneously for cross-validation of their respective performances [
21], and an essential function for upgrade, maintenance, and quality control. Many leading research groups have adopted PLUS for developing image-guided intervention and therapy applications.
OpenIGTLink [
22] provides a unified solution to import real-time imagery (e.g., ultrasound, video) and general data streams (e.g., position tracking) into image-guided therapy and intervention systems. OpenIGTLink has become the default communication standard in its field. SlicerIGT, a dynamically loadable extension to 3D Slicer, enables the rapid translation of image-guided intervention and therapy applications without any programming overhead, using only configuration scripts [
23]. Machine learning (ML) and artificial intelligence (AI) functions for training and invoking deep learning neural networks are grouped in the SlicerAIGT extension package. SlicerIGT offers great speed and ease for integrating new clinical applications and translating them to clinical trials. The generic theme of “spatially tracked ultrasound navigation” is an out-of-the-box feature which does not require any programming, and it works with most ultrasound and spatial tracking devices [
23]. Building on this platform, the application-specific code, written as a Python script, is less than 0.01% of the code base, while the remaining 99.99% is free, open-source software infrastructure [
23], allowing for an extremely high degree to which previously validated software can be reused. The functional and architectural designs of the NaviPBx system are complete.
4. Clinical Validation and Deployment Plan
4.1. Clinical Safety and Feasibility Study
Following an accuracy and workflow evaluation in training phantoms, we will first ensure the safety NaviPBx in human use through a Clinical Safety and Feasibility Study. We will implement a systematic risk management process following the ISO 14,971 standard. Additionally, technical accuracy validation, based on anatomical landmarks and recorded TRUS, will prove the ability to sample a clinically significant prostate cancer target, 0.5 cc in volume. This study will be performed at the Department of Urology of the Aristide Le Dantec University Hospital in Dakar, Senegal. The minimum number of patients will depend on whether major design revisions will be needed, currently estimated to be 50 patients over 1 year.
Research Ethics Approval will be obtained according to standing regulations in Senegal; the country has a nationally centralized process. The approval of a clinical study is valid in any government-acknowledged medical care facility in Senegal, which includes all clinical sites in this project: the Aristide Le Dantec University Hospital and all hospitals of the Senegalese Military Health Service.
We do not plan to analyze specific clinical outcomes in the early implementation phase of the program, for two reasons. Firstly, NaviPBx uses techniques that have been previously validated in peer-reviewed literature. Secondly, there is no reliable baseline data on PBx outcomes in Senegal, as the country’s PBx practice is limited and insufficiently documented. This project will yield nationwide PBx data to be analyzed in follow-up research. We will therefore concentrate our validation efforts on clinical usability and the scalability of nationwide deployment.
4.2. Formative Clinical Usability Study
Malfunctions caused by the inadequate usability of a medical device have become an increasing safety concern. Without thorough investigation of usability aspects, NaviPBx could be non-intuitive and difficult to learn and use, a critically important issue to be addressed before NaviPBx is passed into the hands of less experienced physicians. Formative usability testing will be performed to help developers identify design weaknesses. Formative testing is based on the expertise and knowledge of developers and how they interpret the user’s struggle with the system interface. Another aim of the formative test is to define a “minimum viable product” that incorporates the set of functions necessary and is sufficient for deploying a prospective system in clinical practice. We will implement a usability engineering process, according to the Risk Management Plan previously laid out, to identify and minimize erroneous use and reduce use-associated risks. Following the IEC 62,366 standard, the process will be executed in parallel to risk management. A first-order estimation for the formative usability study, following the guidelines in IEC 62,366 and Faulkner [
35], suggests N = 5–10 urologists as users. The planned study locations are the Aristide Le Dantec University Hospital and the Military Hospitals of Ouakam, Principal and Lemonier, in Dakar, Senegal. Each hospital will participate with two to three attending urologists. The commander of the urological services in the Senegalese Military Health Service will coordinate with the military hospitals, with Ouakam Military Hospital in Dakar acting as the command center. For a military hospital to work efficiently, there is a threshold volume when the scale of economy starts to prevail. For the optimal utilization of the army’s logistical system, each hospital should carry a uniform load, so that the dispatching of personnel and materials can be uniformly managed from the command center. We estimate that 50 patients per year, per hospital would be the optimal intake. The projected length of participation is 1 year, enrolling about one patient per week and per hospital.
4.3. Summative Clinical Usability & Scalability Study
Finally, we will run a summative usability test in which users perform workflow tasks; performance is rated by the usability quotient computed for each design element previously identified in the Risk Management Plan. The summative test will identify the percentage of users having trouble performing a certain action. This will help us to modify the design and/or reimplement the problematic system elements. The second objective is it to evaluate how the operation of NaviPBx scales up to national use across the country, and to quantify the technical, material, and human resource requirements for operating the nationwide program. This information will be reviewed by the Senegalese Military Health Service, which intends to sustain the national program. Based on our previous experience, we estimate that 20–25 users are needed for a successful summative evaluation; this target can be achieved by involving two to three urologists from each of the participating hospitals, with corresponding nurses in each hospital. The targeted number of patients, for previously explained reasons related to the operation efficiency of the Senegalese Military Health Service, is 50 patients per year, per hospital. The planned study locations are 10 hospitals: the Aristide Le Dantec University Hospital; three military hospitals in Dakar; and one hospital in each military zone outside Dakar: Thies (mid-west), Saint-Louis (north), Ziguinchor and Kolda (south), Kaolack (central), and Tambacounda (east), covering the entire territory of Senegal. The projected project length is 2 years, enacted in two stages, each year with three new hospitals, enrolling approximately one patient per week and per hospital.
By end of the project, the clinical studies will have involved a combined 20–30 urologists (within 10 hospitals) and over 1000 patients, cumulatively.
4.4. Training Plan
We will establish mechanisms to train associated personnel (e.g., software engineers, technicians, nurses, physicians) who are qualified to partake in the proposed studies and who will sustain the operation of the prostate biopsy program. The curriculum will include instructional and practice sessions in simulation setup on training dummies and assist expert urologists in human patient cases performed with the NaviPBx system. The training plan also involves nurses’ and technicians’ participation in various tasks (e.g., preparation, calibration, setup, takedown, cleaning, transportation, and storage).
6. Sustainability Plan
The Senegalese Military Health Service is committed to sustaining the NaviPBx program upon successful completion of the project. Senegal is one of the most stable countries in Africa, having experienced peaceful political transitions since its independence in 1960. The main mission of the Senegalese Military Medical Service is to provide medical support to the Armed Forces and ensure health protection at home and abroad, in peacetime and during operations. The Military Health Service has a longstanding civilian mandate within the Senegalese healthcare system, independently from political parties elected to government. Its facilities are open to the public, contributing to national public health coverage. In the care facilities operated by the Military Medical Service, over 90% of the patients are civilians with no connection to the military. The Service operates 14 military regional medical centers over the national territory, nine of which offer urological services and will partake in the NaviPBx program.
Our clinical studies aim to generate evidence of NaviPBx’s robust usability and scalability to nationwide deployment and to quantify the requisite technical, material, and human resources for the continued operation of the prostate biopsy program. The training plan for personnel (e.g., engineers, technicians, nurses, physicians), as outlined earlier, is a critical factor in the continual operation of the national prostate biopsy program.
Importantly, NaviPBx will be shared as a free, open-source software resource, and vigorously advocated as such. Given the successful history over the past two decades in promoting 3D Slicer platform resources, one can anticipate a robust uptake on NaviPBx as a diagnostic and therapy delivery platform for prostate cancer and beyond.
The commercialization of NaviPBx and/or its consumable parts in Senegal and/or regionally in West Africa is an option that is being actively explored, while noting that regulatory aspects of domestically produced medical devices are currently uncertain in Senegal.
We will promote the prostate biopsy program to the general public through our ongoing annual Prostate Disease Awareness Day (PDAD), organized by two expert urologists. A sweeping outreach effort in the Senegalese media and social platforms, PDAD aims to increase the awareness of prostate diseases, particularly of prostate cancer, and to inform patients about the role of prostate biopsy in the early diagnosis and curative management of prostate cancer. Participating media outlets include the Senegalese National Television, four private television networks, six radio stations, and two major social platforms. PDAD provides general information to the public and also free, walk-in urology consultation for ad hoc patients. In Dakar, an average of 55–60 physicians (urologists and general practitioners) participate, seeing 250 to 300 patients for clinical consultations. Upon launching NaviPBx in hospitals across the country, we will extend PDAD into a nationwide campaign. In a preliminary study [
36], we found that using 3D digital anatomy models vastly improved the effectiveness of communication about prostate disease with patients in Senegal. Expanding on this idea, we will create video animations of NaviPBx for public release. Clinical stakeholders will receive project updates through newsletters and symposia of the Senegalese Urological Association, encouraging members to partake in our PDAD campaigns and to reach out to the public. In addition to the Senegalese Military Health Service, we will liaise with the Ministry of Health through demonstrations, regular progress reports, and by extending invitations to NaviPBx project events. The Société Internationale d’Urologie, the Association Francaise d’Urologie, and the American Urological Association will be regularly informed about our progress and results.
Building translational R&D capacities in Senegal is also a critical aspect of increasing the likelihood for the project to exert a sustained positive impact. We aim to help develop translational clinical research capacities in Senegal by training a large portion of Senegal’s urology staff in the Senegalese Military Health Service. Under the leadership of academically minded senior military commanders, this corps is expected to emerge as a highly organized, experienced, and productive translational research force. The clinical and engineering personnel emerging from this program stand to represent a national resource in Senegal, to be leveraged in research and in the development of image-guided diagnostic and therapeutic intervention technologies. The project personnel will gain experience in translational research and apply their knowledge to high-impact medical problems with practical and societal implications. Such a skillset will be of utmost value to the biotechnology and healthcare sectors in Senegal. A recent report by the World Economic Forum on the Future of Jobs identified emerging job roles in Sub-Saharan Africa through extensive surveys and studies of local industry. Amongst the top five emerging job roles were “Software Application Developers and Analysists, Data Analysts and Scientists,” with the critical skills of “analytical thinking and innovation, technology design and programing” [
37]. Overall, the diverse pool of individuals trained through this project will be important stakeholders in the emergent healthcare job market in Senegal.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



