Using Stubby Prosthesis after Bilateral Transfemoral Amputation: A Biomechanical Case Study

 , and
, and
Abstract
:1. Introduction
2. Case Report
2.1. Outcomes
2.2. Gait Analysis
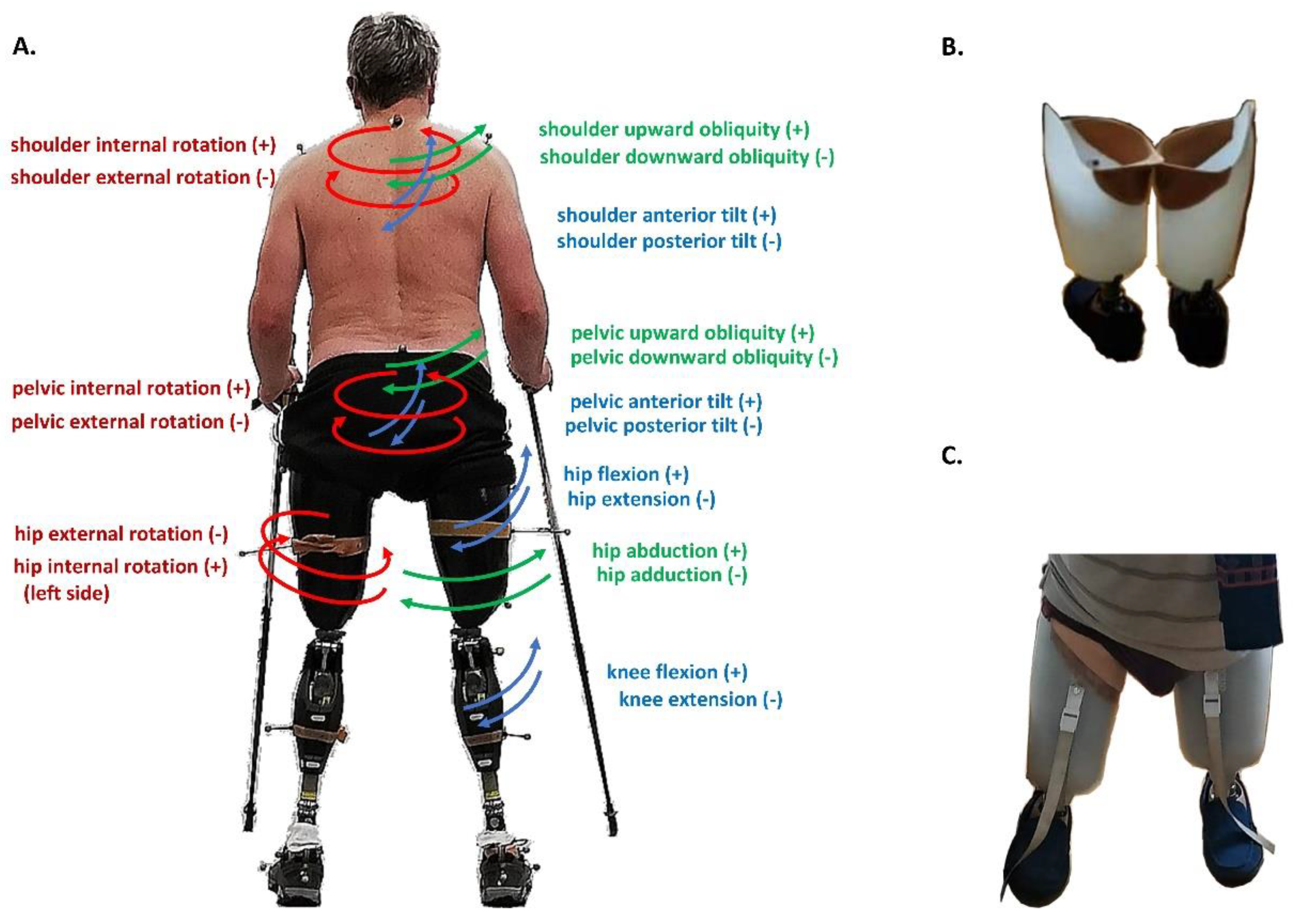
- shoulder girdle obliquity angle (up/down)—rotation of the mediolateral axis out of the horizontal plane in the frontal plane; a positive value (up) corresponds to the situation in which acromion process markers are higher than the corresponding markers on the contralateral side
- shoulder girdle tilt—anterior/posterior rotation around the mediolateral axis in the transversal plane; a positive value (up) corresponds to the normal situation in which acromion process markers are higher than the corresponding markers on the contralateral side
- shoulder girdle rotation—rotation of the mediolateral axis around the vertical axis in horizontal plane
- pelvic obliquity angle (up/down)—rotation of the mediolateral axis out of the horizontal plane in the frontal plane; a positive value (up) corresponds to the situation in which anterior and posterior superior iliac spine (ASIS and PSIS) markers are higher than the corresponding markers on the contralateral side
- pelvic tilt angle (up/down)—anterior/posterior rotation around the mediolateral axis in the transversal plane; a positive value (up) corresponds to a normal situation in which PSIS is higher than ASIS
- pelvic rotation angle (internal/external)—rotation of the mediolateral axis around the vertical axis in the horizontal plane
- hip ad/abduction angle—rotation of the proximal-distal axis out of the sagittal plane in the frontal plane
- hip flexion/extension angle—rotation of the proximal-distal axis around the mediolateral axis in the sagittal plane; a positive (flexion) angle value corresponds to a situation in which the knee is in front of the body
- hip rotation angle (internal/external)—rotation around the proximal-distal axis in the horizontal plane
- knee flexion/extension angle—rotation of the proximal-distal axis around the mediolateral axis in the sagittal plane; a positive angle corresponds to a flexed knee.
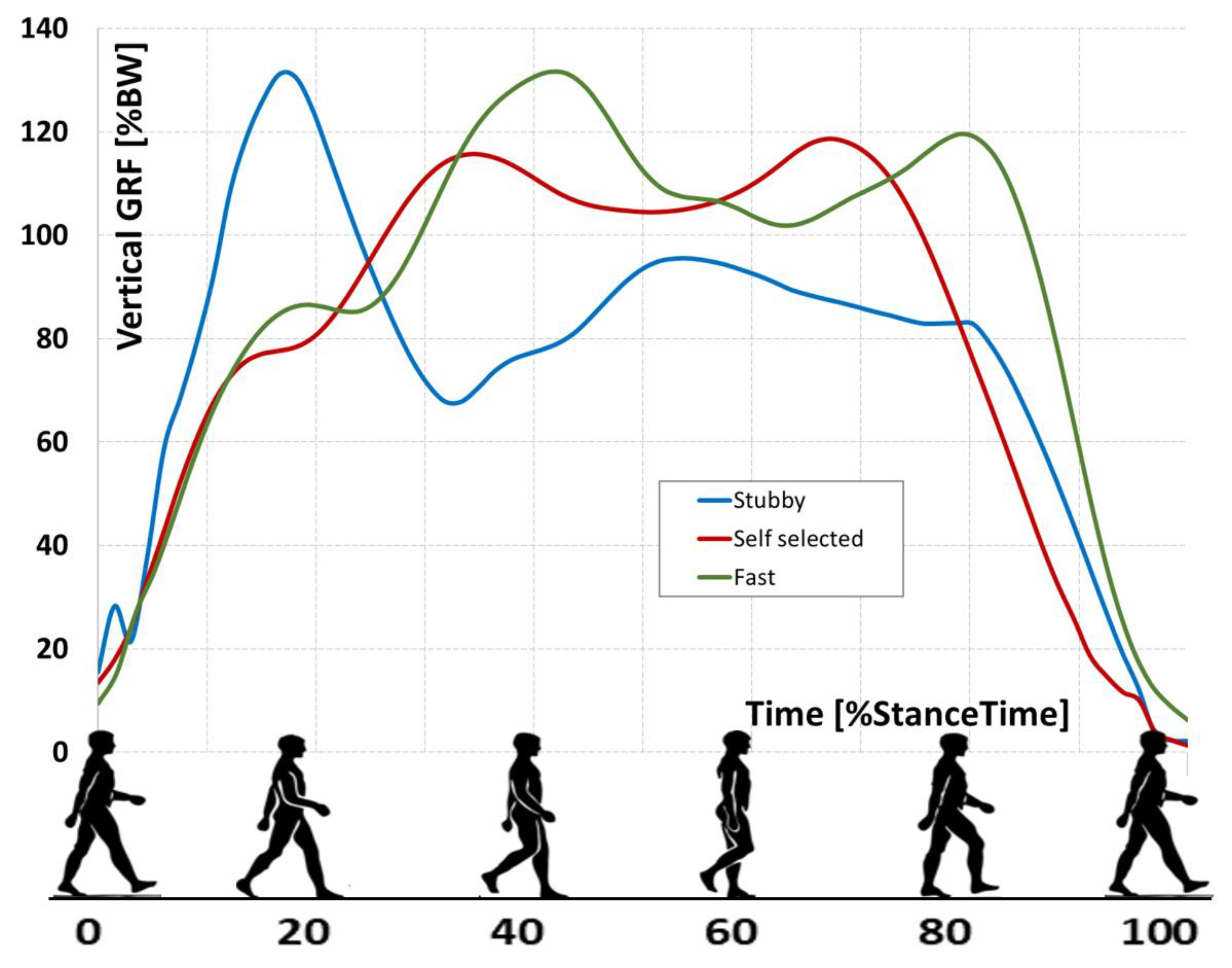
- vF1: maximal vGRF of overweight during the initial weight acceptance phase
- vF2: minimal vGRF of underweight during the middle stance phase
- vF3: maximal vGRF of overweight during the terminal stance phase
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ladlow, P.; Phillip, R.; Coppack, R.; Etherington, J.; Bilzon, J.; McGuigan, M.P.; Bennett, A.N. Influence of Immediate and Delayed Lower-Limb Amputation Compared with Lower-Limb Salvage on Functional and Mental Health Outcomes Post-Rehabilitation in the UK Military. J. Bone Jt. Surg. Am. Vol. 2016, 98, 1996–2005. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D.; Sheldahl, L.M.; Buley, K.J.; Sandford, P.R. Physiological comparison of walking among bilateral above-knee amputee and able-bodied subjects, and a model to account for the differences in metabolic cost. Arch. Phys. Med. Rehabil. 1997, 78, 385–392. [Google Scholar] [CrossRef]
- Foote, C.E.; Kinnon, J.M.; Robbins, C.; Pessagno, R.; Portner, M.D. Long-term health and quality of life experiences of Vi-etnam veterans with combat-related limb loss. Qual. Life Res. 2015, 24, 2853–2861. [Google Scholar] [CrossRef] [PubMed]
- van Schaik, L.; Geertzen, J.H.B.; Dijkstra, P.U.; Dekker, R. Metabolic costs of activities of daily living in persons with a lower limb amputation: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0213256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, I.J.; Sosnov, J.A.; Howard, J.T.; Orman, J.A.; Fang, R.; Morrow, B.D.; Zonies, D.H.; Bollinger, M.; Tuman, C.; Freedman, B.A.; et al. Retrospective Analysis of Long-Term Outcomes After Combat Injury A Hidden Cost of War. Circulation 2015, 132, 2126–2133. [Google Scholar] [CrossRef]
- Weinert-Aplin, R.; Twiste, M.; Jarvis, H.; Bennett, A.; Baker, R. Medial-lateral centre of mass displacement and base of support are equally good predictors of metabolic cost in amputee walking. Gait Posture 2017, 51, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawson, B.E.; Ruhe, B.; Shultz, A.; Goldfarb, M. A Powered Prosthetic Intervention for Bilateral Transfemoral Amputees. IEEE Trans. Biomed. Eng. 2015, 62, 1042–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Major, M.J.; Stine, R.L.; Gard, S.A. The effects of walking speed and prosthetic ankle adapters on upper extremity dy-namics and stability-related parameters in bilateral transtibial amputee gait. Gait Posture 2013, 38, 858–863. [Google Scholar] [CrossRef] [Green Version]
- Su, P.F.; Gard, S.A.; Lipschutz, R.D.; Kuiken, T.A. Differences in gait characteristics between persons with bilateral tran-stibial amputations, due to peripheral vascular disease and trauma, and able-bodied ambulators. Arch. Phys. Med. Rehabil. 2008, 89, 1386–1394. [Google Scholar] [CrossRef] [Green Version]
- Chereshnev, R.; Kertész-Farkas, A. GaIn: Human Gait Inference for Lower Limbic Prostheses for Patients Suffering from Double Trans-Femoral Amputation. Sensors 2018, 18, 4146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladlow, P.; Nightingale, T.E.; McGuigan, M.P.; Bennett, A.N.; Phillip, R.D.; Bilzon, J.L.J. Predicting ambulatory energy ex-penditure in lower limb amputees using multi-sensor methods. PLoS ONE 2019, 14, e0209249. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, K.R.; Frittoli, S.; Frigo, C.A. Gait asymmetry of transfemoral amputees using mechanical and microproces-sor-controlled prosthetic knees. Clin. Biomech. 2012, 27, 460–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNealy, L.L.; Gard, S.A. Effect of prosthetic ankle units on the gait of persons with bilateral trans-femoral amputa-tions. Prosthet. Orthot. Int. 2008, 32, 111–126. [Google Scholar] [CrossRef]
- Jarvis, H.L.; Bennett, A.N.; Twiste, M.; Phillip, R.D.; Etherington, J.; Baker, R. Temporal Spatial and Metabolic Measures of Walking in Highly Functional Individuals With Lower Limb Amputations. Arch. Phys. Med. Rehabil. 2017, 98, 1389–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, M.K.; Carroll, K.; Rheinstein, J.; Highsmith, M.J. Functional Differences of Bilateral Transfemo-Ral Amputees Using Full-Length and Stubby-Length Prostheses. Technol. Innov. 2018, 20, 75–83. [Google Scholar] [CrossRef]
- Haque, R.; Al-Jawazneh, S.; Hoellwarth, J.; Akhtar, M.A.; Doshi, K.; Tan, Y.C.; Lu, W.Y.; Roberts, C.; Al Muderis, M. Osseointegrated reconstruction and rehabilitation of transtibial am-putees: The Osseointegration Group of Australia surgical technique and protocol for a prospective cohort study. BMJ Open. 2020, 10, e038346. [Google Scholar] [CrossRef]
- Hoellwarth, J.S.; Tetsworth, K.; Kendrew, J.; Kang, N.V.; van Waes, O.J.F.; Al-Maawi, Q.; Roberts, C.; al Muderis, M. Periprosthetic osseointegration fractures are infrequent and manage-ment is familiar. Bone Jt. J. 2020, 102, 162–169. [Google Scholar] [CrossRef]
- Mcmenemy, L.; Ramasamy, A.; Sherman, K.; Mistlin, A.; Phillip, R.; Evriviades, D.; Kendrew, J. Direct Skeletal Fixation in bilateral above knee amputees following blast: 2 year follow up results from the initial cohort of UK service personnel. Injury 2020, 51, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.J.; Karduna, A.R.; McQuade, K.; Wang, X.; Frederick, W.W.; et al. ISB recommendation on definitions of joint coordinate systems of vari-ous joints for the reporting of human joint motion-Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Pietraszewski, B.; Winiarski, S.; Jaroszczuk, S. Three-dimensional human gait pattern-reference data for normal men. Acta Bioeng. Biomech. 2012, 14, 9–16. [Google Scholar]
- Day, M.C.; Wadey, R.; Strike, S. Living with limb loss: Everyday experiences of “good” and “bad” days in people with lower limb amputation. Disabil. Rehabil. 2019, 41, 2433–2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Temporo-Spatial Parameters | |||||||
|---|---|---|---|---|---|---|---|
| Fast | Self-Selected | Stubby Prostheses | |||||
| R | L | R | L | R | L | ||
| Spatial parameters [m] | |||||||
| Stride length | 1.31 ± 0.1 | 1.29 ± 0.1 | 1.21 ± 0.1 | 1.2 ± 0.1 | 0.71 ± 0.1 | 0.71 ± 0.1 | |
| Step width | 0.29 | 0.26 | 0.24 | ||||
| Step | 0.66 ± 0.1 | 0.57 ± 0.1 | 0.62 ± 0.1 | 0.54 ± 0.1 | 0.32 ± 0.1 | 0.34 ± 0.1 | |
| Speeds [m/s] | |||||||
| Velocity | 0.83 ± 0.02 | 0.69 ± 0.06 | 0.75 ± 0.06 | ||||
| Cad | 1.51 | 1.3 | 2.14 | ||||
| Scalar parameters [%GC] | |||||||
| Stance | 0.63 ± 0.01 | 0.69 ± 0.03 | 0.65 ± 0.03 | 0.7 ± 0.03 | 0.65 ± 0.02 | 0.66 ± 0.03 | |
| Double Stance | 0.18 ± 0.03 | 0.17 ± 0.02 | 0.19 ± 0.03 | 0.18 ± 0.03 | 0.14 ± 0.03 | 0.16 ± 0.01 | |
| Swing | 0.36 ± 0.01 | 0.31 ± 03 | 0.34 ± 0.03 | 0.30 ± 0.03 | 0.35 ± 0.02 | 0.34 ± 0.03 | |
| Temporal parameters [s] | |||||||
| Stride | 1.55 ± 0.1 | 1.33 ± 0.1 | 1.55 ± 0.2 | 1.55 ± 0.1 | 0.94 ± 0.1 | 0.94 ± 0.1 | |
| Stance | 0.84 ± 0.1 | 0.92 ± 0.1 | 1.02 ± 0.1 | 1.01 ± 0.1 | 0.61 ± 0.1 | 0.61 ± 0.1 | |
| Double Stance | 0.23 ± 0.1 | 0.22 ± 0.1 | 0.29 ± 0.1 | 0.27 ± 0.1 | 0.13 ± 0.1 | 0.14 ± 0.1 | |
| Swing | 0.48 ± 0.1 | 0.41 ± 0.1 | 0.52 ± 0.1 | 0.46 ± 0.1 | 0.32 ± 0.1 | 0.34 ± 0.1 | |
| Angle [°] | ||||||
|---|---|---|---|---|---|---|
| Fast | Self-Selected | Stubby Prostheses | ||||
| R | L | R | L | R | L | |
| Shoulder girdle tilt | ||||||
| ROMmax | 52.6 | 51.4 | 51.3 | 51.4 | 42.2 | 51.4 |
| ROMmin | 38.2 | 39 | 44.5 | 46.1 | 33 | 30.6 |
| ROMrange | 14.4 | 12.4 | 6.8 | 5.8 | 9.2 | 11.3 |
| Shoulder girdle obliquity | ||||||
| ROMmax | 4.2 | 2.5 | 2.6 | 0.2 | 4.4 | −0.8 |
| ROMmin | −1.9 | −5.2 | −0.3 | −3.1 | 1.3 | −4.3 |
| ROMrange | 6.1 | 7.7 | 2.9 | 3.3 | 3.1 | 3.5 |
| Shoulder girdle rotation | ||||||
| ROMmax | 3.3 | 15.2 | −0.6 | 18 | 5.4 | 11.4 |
| ROMmin | −15.8 | −2.6 | −18.6 | 1 | −13.5 | −5 |
| ROMrange | 19.1 | 17.8 | 18 | 17 | 18.9 | 16.4 |
| Pelvic tilt | ||||||
| ROMmax | 22.9 | 23 | 22.2 | 22.1 | 16.9 | 17.3 |
| ROMmin | 18.4 | 19.2 | 17.4 | 17.8 | 13.4 | 13.4 |
| ROMrange | 4.5 | 3.8 | 4.8 | 4.3 | 3.5 | 3.9 |
| Pelvic obliquity | ||||||
| ROMmax | 6.2 | 2.4 | 8.1 | 4 | 11.2 | 2.6 |
| ROMmin | −2.6 | −6.4 | −4.2 | −7.6 | −2.2 | −11.5 |
| ROMrange | 8.8 | 8.8 | 12.3 | 11.6 | 13.4 | 14.1 |
| Pelvic rotation | ||||||
| ROMmax | 11.9 | 12.7 | 11.8 | 15.6 | 5.2 | 16.6 |
| ROMmin | −12.8 | −12 | −16.6 | −11.3 | −16.2 | −7.4 |
| ROMrange | 24.7 | 24.5 | 28.4 | 26.9 | 21.4 | 24 |
| Hip flexion/extension | ||||||
| ROMmax | 46.4 | 55.8 | 42.5 | 50 | 31.1 | 50.9 |
| ROMmin | −1.1 | 0.5 | −0.4 | 0.8 | −22.2 | −5.7 |
| ROMrange | 47.5 | 55.3 | 42.9 | 49.2 | 53.3 | 56.6 |
| Knee flexion/extension | ||||||
| ROMmax | 50.4 | 58.2 | 40.4 | 53.8 | ||
| ROMmin | −8.3 | 0.5 | −10.4 | −1.7 | ||
| ROMrange | 58.7 | 57.7 | 50.8 | 55.5 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiodorenko-Dumas, Ż.; Dumas, I.; Kowal, M.; Machnikowska, A.; Gieysztor, E.; Winiarski, S.; Paprocka-Borowicz, M. Using Stubby Prosthesis after Bilateral Transfemoral Amputation: A Biomechanical Case Study. Appl. Sci. 2021, 11, 3671. https://doi.org/10.3390/app11083671
Fiodorenko-Dumas Ż, Dumas I, Kowal M, Machnikowska A, Gieysztor E, Winiarski S, Paprocka-Borowicz M. Using Stubby Prosthesis after Bilateral Transfemoral Amputation: A Biomechanical Case Study. Applied Sciences. 2021; 11(8):3671. https://doi.org/10.3390/app11083671
Chicago/Turabian StyleFiodorenko-Dumas, Żanna, Ilias Dumas, Mateusz Kowal, Adrianna Machnikowska, Ewa Gieysztor, Sławomir Winiarski, and Małgorzata Paprocka-Borowicz. 2021. "Using Stubby Prosthesis after Bilateral Transfemoral Amputation: A Biomechanical Case Study" Applied Sciences 11, no. 8: 3671. https://doi.org/10.3390/app11083671