
Right Ventricular Global and Regional Remodeling in American-Style Football Athletes: A Longitudinal 3D Echocardiographic Study

 , , ,
, , ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Echocardiographic Acquisitions and Image Processing
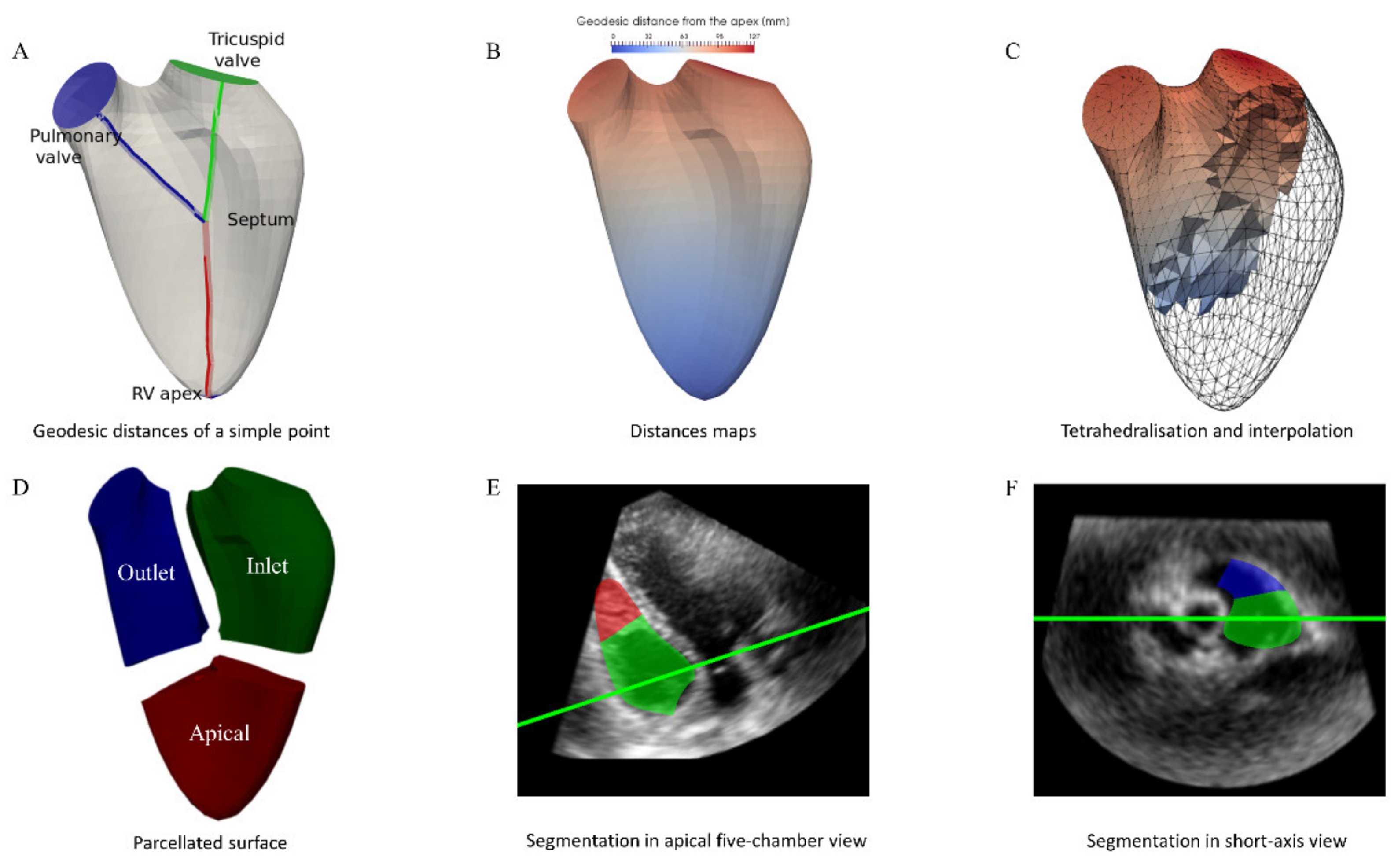
2.3. Parcellation of the Right Ventricle
2.4. Statistical Analysis
3. Results
3.1. Clinical Data
3.2. Impact of Inter-Seasonal Training on Cardiac Morphology and Function
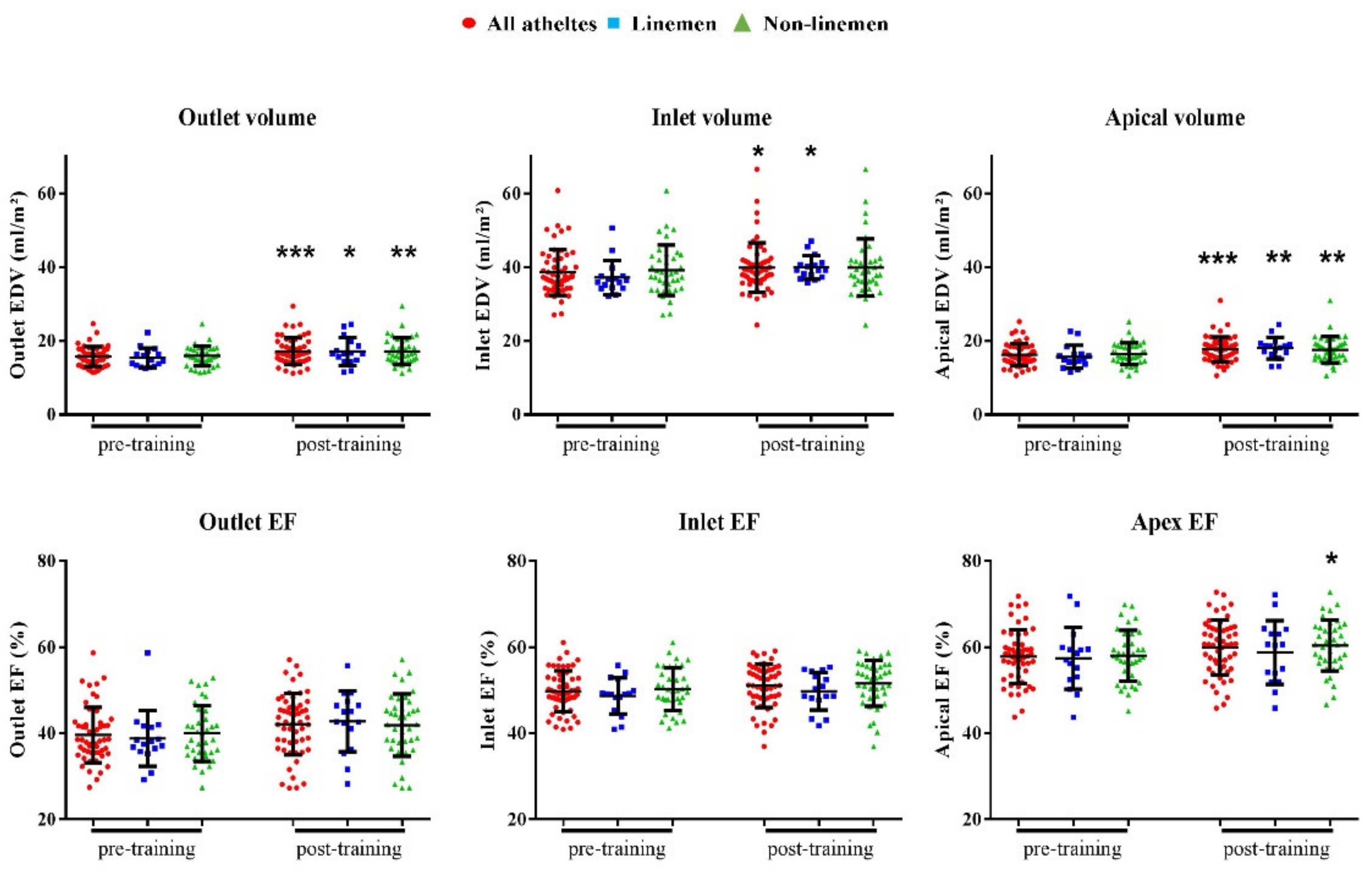
3.3. Assessment of the Regional RV Changes Using 3D Parcellation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weiner, R.B.; Wang, F.; Isaacs, S.K.; Malhotra, R.; Berkstresser, B.; Kim, J.H.; Hutter, A.M.; Picard, M.H.; Wang, T.J.; Baggish, A.L. Blood Pressure and Left Ventricular Hypertrophy during American-Style Football Participation. Circulation 2013, 128, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Wang, F.; Weiner, R.B.; DeLuca, J.R.; Wasfy, M.M.; Berkstresser, B.; Lewis, G.D.; Hutter, A.M.; Picard, M.H.; Baggish, A.L. Blood Pressure and LV Remodeling Among American-Style Football Players. JACC Cardiovasc. Imaging 2016, 9, 1367–1376. [Google Scholar] [CrossRef]
- Kim, J.H.; Hollowed, C.; Irwin-Weyant, M.; Patel, K.; Hosny, K.; Aida, H.; Gowani, Z.; Sher, S.; Gleason, P.; Shoop, J.L.; et al. Sleep-Disordered Breathing and Cardiovascular Correlates in College Football Players. Am. J. Cardiol. 2017, 120, 1410–1415. [Google Scholar] [CrossRef]
- Kim, J.H.; Hollowed, C.; Patel, K.; Hosny, K.; Aida, H.; Gowani, Z.; Sher, S.; Shoop, J.L.; Galante, A.; Clark, C.; et al. Temporal Changes in Cardiovascular Remodeling Associated with Football Participation. Med. Sci. Sports Exerc. 2018, 50, 1892–1898. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Hollowed, C.; Liu, C.; Al-Badri, A.; Alkhoder, A.; Dommisse, M.; Gowani, Z.; Miller, A.; Nguyen, P.; Prabakaran, G.; et al. Weight Gain, Hypertension, and the Emergence of a Maladaptive Cardiovascular Phenotype Among US Football Players. JAMA Cardiol. 2019, 4, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Zafonte, R.; Pascuale-Leon, A.; Nadler, L.M.; Weisskopf, M.; Speizer, F.E.; Taylor, H.A.; Baggish, A.L. American-Style Football and Cardiovascular Health. J. Am. Heart. Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, A.; Ghani, S.; Sharma, R.; Oxborough, D.; Panoulas, V.F.; Sheikh, N.; Gati, S.; Papadakis, M.; Sharma, S. Physiological Right Ventricular Adaptation in Elite Athletes of African and Afro-Caribbean Origin. Circulation 2013, 127, 1783–1792. [Google Scholar] [CrossRef] [Green Version]
- D’Ascenzi, F.; Pisicchio, C.; Caselli, S.; Di Paolo, F.M.; Spataro, A.; Pelliccia, A. RV Remodeling in Olympic Athletes. JACC Cardiovasc. Imaging 2017, 10, 385–393. [Google Scholar] [CrossRef]
- D’Andrea, A.; Riegler, L.; Golia, E.; Cocchia, R.; Scarafile, R.; Salerno, G.; Pezzullo, E.; Nunziata, L.; Citro, R.; Cuomo, S.; et al. Range of Right Heart Measurements in Top-Level Athletes: The Training Impact. Int. J. Cardiol. 2013, 164, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Wang, F.; Weiner, R.B.; Elinoff, J.M.; Tournoux, F.; Boland, A.; Picard, M.H.; Hutter, A.M.; Wood, M.J. Training-Specific Changes in Cardiac Structure and Function: A Prospective and Longitudinal Assessment of Competitive Athletes. J. Appl. Physiol. 2008, 104, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Riegler, L.; Morra, S.; Scarafile, R.; Salerno, G.; Cocchia, R.; Golia, E.; Martone, F.; Di Salvo, G.; Limongelli, G.; et al. Right Ventricular Morphology and Function in Top-Level Athletes: A Three-Dimensional Echocardiographic Study. J. Am. Soc. Echocardiogr. 2012, 25, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzi, F.; Solari, M.; Corrado, D.; Zorzi, A.; Mondillo, S. Diagnostic Differentiation Between Arrhythmogenic Cardiomyopathy and Athlete’s Heart by Using Imaging. JACC Cardiovasc. Imaging 2018, 11, 1327–1339. [Google Scholar] [CrossRef]
- Prior, D. Differentiating Athlete’s Heart from Cardiomyopathies—The Right Side. Heart Lung Circ. 2018, 27, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Bernardino, G.; Hodzic, A.; Langet, H.; Legallois, D.; de Craene, M.; González Ballester, M.A.; Saloux, E.; Bijnens, B. Volumetric parcellation of the cardiac right ventricle for regional geometric and functional assessment. Med. Image Anal. 2021, in press. [Google Scholar] [CrossRef]
- Croft, L.B.; Belanger, A.; Miller, M.A.; Roberts, A.; Goldman, M.E. Comparison of National Football League Linemen versus Nonlinemen of Left Ventricular Mass and Left Atrial Size. Am. J. Cardiol. 2008, 102, 343–347. [Google Scholar] [CrossRef]
- Mosteller, R.D. Simplified Calculation of Body-Surface Area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Utomi, V.; Oxborough, D.; Whyte, G.P.; Somauroo, J.; Sharma, S.; Shave, R.; Atkinson, G.; George, K. Systematic Review and Meta-Analysis of Training Mode, Imaging Modality and Body Size Influences on the Morphology and Function of the Male Athlete’s Heart. Heart 2013, 99, 1727–1733. [Google Scholar] [CrossRef]
- Bohm, P.; Schneider, G.; Linneweber, L.; Rentzsch, A.; Krämer, N.; Abdul-Khaliq, H.; Kindermann, W.; Meyer, T.; Scharhag, J. Right and Left Ventricular Function and Mass in Male Elite Master Athletes: A Controlled Contrast-Enhanced Cardiovascular Magnetic Resonance Study. Circulation 2016, 133, 1927–1935. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Anselmi, F.; Piu, P.; Fiorentini, C.; Carbone, S.F.; Volterrani, L.; Focardi, M.; Bonifazi, M.; Mondillo, S. Cardiac Magnetic Resonance Normal Reference Values of Biventricular Size and Function in Male Athlete’s Heart. JACC Cardiovasc. Imaging 2019, 12, 1755–1765. [Google Scholar] [CrossRef]
- Spence, A.L.; Carter, H.H.; Murray, C.P.; Oxborough, D.; Naylor, L.H.; George, K.P.; Green, D.J. Magnetic Resonance Imaging-Derived Right Ventricular Adaptations to Endurance versus Resistance Training. Med. Sci. Sports Exerc. 2013, 45, 534–541. [Google Scholar] [CrossRef]
- Fagard, R.H. Athlete’s Heart: A Meta-Analysis of the Echocardiographic Experience. Int. J. Sports Med. 1996, 17 (Suppl. S3), S140–S144. [Google Scholar] [CrossRef] [PubMed]
- Sitges, M.; Merino, B.; Butakoff, C.; de la Garza, M.S.; Paré, C.; Montserrat, S.; Vidal, B.; Azqueta, M.; Sarquella, G.; Gutierrez, J.A.; et al. Characterizing the Spectrum of Right Ventricular Remodelling in Response to Chronic Training. Int. J. Cardiovasc. Imaging 2017, 33, 331–339. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Pelliccia, A.; Corrado, D.; Cameli, M.; Curci, V.; Alvino, F.; Natali, B.M.; Focardi, M.; Bonifazi, M.; Mondillo, S. Right Ventricular Remodelling Induced by Exercise Training in Competitive Athletes. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 301–307. [Google Scholar] [CrossRef]
- Gülan, U.; Saguner, A.M.; Akdis, D.; Gotschy, A.; Tanner, F.C.; Kozerke, S.; Manka, R.; Brunckhorst, C.; Holzner, M.; Duru, F. Hemodynamic Changes in the Right Ventricle Induced by Variations of Cardiac Output: A Possible Mechanism for Arrhythmia Occurrence in the Outflow Tract. Sci. Rep. 2019, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- La Gerche, A.; Robberecht, C.; Kuiperi, C.; Nuyens, D.; Willems, R.; de Ravel, T.; Matthijs, G.; Heidbüchel, H. Lower than Expected Desmosomal Gene Mutation Prevalence in Endurance Athletes with Complex Ventricular Arrhythmias of Right Ventricular Origin. Heart 2010, 96, 1268–1274. [Google Scholar] [CrossRef]
- Bernardino, G.; Sanz de la Garza, M.; Domenech-Ximenos, B.; Prat-Gonzàlez, S.; Perea, R.J.; Blanco, I.; Burgos, F.; Sepulveda-Martinez, A.; Rodriguez-Lopez, M.; Crispi, F.; et al. Three-Dimensional Regional Bi-Ventricular Shape Remodeling Is Associated with Exercise Capacity in Endurance Athletes. Eur. J. Appl. Physiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lewicka-Potocka, Z.; Dąbrowska-Kugacka, A.; Lewicka, E.; Kaleta, A.M.; Dorniak, K.; Daniłowicz-Szymanowicz, L.; Fijałkowski, M.; Nabiałek-Trojanowska, I.; Ratkowski, W.; Potocki, W.; et al. The “Athlete’s Heart” Features in Amateur Male Marathon Runners. Cardiol. J. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| All Athletes (n = 59) | Non-Linemen (n = 39) | Linemen (n = 20) | ||||
|---|---|---|---|---|---|---|
| Pre-T | Post-T | Pre-T | Post-T | Pre-T | Post-T | |
| Age, y | 21.9 ± 1.4 | 21.8 ± 1.4 | 22 ± 1.5 | |||
| Caucasian | 40 (68%) | 26 (67%) | 14 (70%) | |||
| Afro-Caribbean | 19 (32%) | 13 (33%) | 6/ (30%) | |||
| Prior university ASF seasons | 1.6 ± 1.1 | 1.6 ± 1.1 | 1.7 ± 1.1 | |||
| Height, cm | 183.6 ± 7.2 | 181.2 ± 6.1 | 188.3 ± 7.1 † | |||
| Weight, kg | 102.3 ± 22.6 | 101 ± 20.4 | 88.7 ± 9.8 | 89.3 ± 9.7 | 128.4 ± 16.9 ††† | 123.9 ± 16 ***, ††† |
| BMI, kg/m2 | 30.1 ± 5.5 | 29 ± 4.8 | 27.1 ± 3 | 27.2 ± 2.9 | 36.1 ± 4.1 ††† | 34.8 ± 3.8 ***, ††† |
| BSA, m2 | 2.28 ± 0.28 | 2.26 ± 0.25 | 2.1 ± 0.1 | 2.1 ± 0.1 | 2.6 ± 0.2 ††† | 2.5 ± 0.2 ***, ††† |
| Body fat, % | 19 ± 7.4 | 18.2 ± 6.6 | 15.3 ± 4.7 | 15.2 ± 4 | 26.2 ± 6.4 ††† | 24.2 ± 6.7 ††† |
| HR, beats/min | 58.9 ± 7.9 | 60.2 ± 8.1 | 57.8 ± 7.8 | 60.4 ± 8.4 * | 60.4 ± 8.2 | 59.7 ± 7.7 |
| SBP, mmHg | 121.6 ± 10.6 | 122.4 ± 9.4 | 118.2 ± 8.8 | 122.5 ±9.5 | 128.2 ± 11.1 ††† | 121.8 ± 9.5 * |
| DBP, mmHg | 67 ± 8.3 | 73.9 ± 8 *** | 64.5 ± 7.3 | 74.1 ± 7 *** | 72.2 ± 7.8 ††† | 73.6 ± 9.8 |
| Variable | All Athletes (n = 59) | Non-Linemen (n = 39) | Linemen (n = 20, 15 for 3D Data) | |||
|---|---|---|---|---|---|---|
| Pre-T | Post-T | Pre-T | Post-T | Pre-T | Post-T | |
| RV Dimensions | ||||||
| 3D-RV EDV, mL | 163.4 ± 31.4 | 174.3 ± 33.7 *** | 155 ± 28.2 | 164.7 ± 30 *** | 185.6 ± 29 †† | 197.7 ± 32 ***, †† |
| 3D-RV EDVi, mL/m2 | 72.7 ±1 2.3 | 77.8 ± 12.7 *** | 73.4 ± 13.2 | 77.8 ± 13.6 *** | 71.4 ± 9.6 | 77.7 ± 10.6 *** |
| 3D-RV ESV, mL | 80.1 ± 16.9 | 81.8 ± 19.2 | 75.4 ± 14.2 | 76.8 ± 17.1 | 93 ± 18.2 †† | 93.7 ± 19 †† |
| 3D-RV ESVi, mL/m2 | 35.6 ± 6.3 | 36.4 ± 7.4 | 35.7 ± 6.5 | 36.2 ± 7.8 | 35.7 ± 6.1 | 36.9 ± 6.5 |
| RV basal diameter, mm | 47.2 ± 4.9 | 48.2 ± 4.7 | 45.4 ± 4.1 | 46.3 ± 4 | 50.9 ± 4.1 ††† | 52 ± 3.7 ††† |
| RV basal diameter i, mm/m2 | 20.9 ± 2.4 | 21.4 ± 2 | 21.5 ± 2 | 21.9 ± 2 | 19.8 ± 2.7 | 20.5 ± 1.6 |
| RV mid diameter, mm | 40 ± 4.6 | 41 ± 4.3 | 38.8 ± 4 | 39.6 ± 3.3 | 42.5 ± 4.8 † | 43.7 ± 4.8 †† |
| RV mid diameter i, mm/m2 | 17.8 ± 2.4 | 18.3 ± 2.2 | 18.4 ± 2 | 18.8 ± 1.8 | 16.6 ± 2.8 | 17.3 ± 2.6 |
| RVOT PLAX diameter, mm | 31.3 ± 4.8 | 31.2 ± 5 | 29.7 ± 1.9 | 29.5 ± 4.6 | 33.7 ± 4.4 † | 33.9 ± 4.4 † |
| RVOT PLAX diameter i, mm/m2 | 13.7 ± 1.8 | 13.6 ± 1.8 | 14 ± 2 | 13.9 ± 1.9 | 13 ± 1.2 | 13.3 ± 1.6 |
| RV longitudinal diameter, mm | 95.4 ± 7.3 | 97 ± 62 * | 93.8 ± 6.7 | 95.6 ± 6.2 * | 99.3 ± 7.1 †† | 100.5 ± 4.8 †† |
| RV longitudinal diameter i, mm/m2 | 42.9 ± 4.5 | 43.8 ± 4.2 * | 44.6 ± 3.7 | 45.3 ± 3.5 | 38.5 ± 3.5 †† | 39.9 ± 3.3 *, †† |
| RV wall thickness, mm | 2.7 ± 0.6 | 2.6 ± 0.6 | 2.5 ± 0.5 | 2.4 ± 0.6 | 3 ± 0.7 | 2.8 ± 0.6 † |
| RV Function | ||||||
| 3D-RV global EF, % | 51 ± 4 | 53.2 ± 3.7 ** | 51.2 ± 4 | 53.6 ± 3.5 ** | 50.1 ± 3.8 | 52.3 ± 4.2 |
| 3D-RV FW strain, % | −27.3 ± 3.6 | −27.7 ± 2.8 | −27.4 ± 3.6 | −28 ± 3 | −27.5 ± 3.3 | −27.1 ± 2.3 |
| TDI RV lateral peak s’, cm/s | 13.9 ± 2.6 | 13.8 ± 2 | 14 ± 2.6 | 14 ± 2 | 13.7 ± 2.6 | 13.6 ± 2.1 |
| TDI RV lateral peak e’, cm/s | 13.4 ± 2.1 | 12.7 ± 2.9 | 13.5 ± 2 | 12.7 ± 2.9 | 13.5 ± 2.3 | 12.5 ± 3 |
| TAPSE, mm | 25.3 ± 4.4 | 25.9 ± 3.5 | 24.2 ± 3.7 | 25.7 ± 3.5 | 27.5 ± 4.5 | 26.2 ± 3.4 |
| RA Dimensions | ||||||
| RA ESV volume, mL | 51.9 ± 13.2 | 58.1 ± 14 *** | 50.3 ± 13.5 | 54.6 ± 13 *** | 55.1 ± 12.5 | 65 ± 13.7 ***, † |
| RA ESV volume i, mL/m2 | 23 ± 6 | 25.7 ± 5.6 *** | 23.9 ± 6.6 | 25.8 ± 6 *** | 21.3 ± 4.5 | 25.5 ± 4.7 *** |
| Variable | Intra-Observer | Inter-Observer |
|---|---|---|
| RV global | ||
| RV EDV, mL | 5 (3.3%) | 11 (7%) |
| RV ESV, mL | 4.1 (5.4%) | 10.6 (15.3%) |
| RV EF, % | 2.4 (4.9%) | 5.2 (10.2%) |
| RV Inlet | ||
| RV inlet EDV, mL | 3.3 (4.1%) | 9.3 (12.2%) |
| RV inlet ESV, mL | 3.2 (7.8%) | 6.1 (16.2%) |
| RV Inlet EF, % | 3.3 (7%) | 5.1 (10.6%) |
| RV Apex | ||
| RV apex EDV, mL | 1.8 (5.3%) | 3.5 (9%) |
| RV apex ESV, mL | 1.8 (12.9%) | 3.4 (23.7%) |
| RV apex EF, % | 5.2 (9.3%) | 8.7 (14.8%) |
| RV Outlet | ||
| RV outlet EDV, mL | 3.4 (10%) | 9 (22.2%) |
| RV outlet ESV, mL | 2.1 (10.9%) | 4.1 (20.4%) |
| RV outlet EF, % | 3.2 (7.9%) | 10.7 (23.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodzic, A.; Bernardino, G.; Legallois, D.; Gendron, P.; Langet, H.; De Craene, M.; González Ballester, M.A.; Milliez, P.; Normand, H.; Bijnens, B.; et al. Right Ventricular Global and Regional Remodeling in American-Style Football Athletes: A Longitudinal 3D Echocardiographic Study. Appl. Sci. 2021, 11, 3357. https://doi.org/10.3390/app11083357
Hodzic A, Bernardino G, Legallois D, Gendron P, Langet H, De Craene M, González Ballester MA, Milliez P, Normand H, Bijnens B, et al. Right Ventricular Global and Regional Remodeling in American-Style Football Athletes: A Longitudinal 3D Echocardiographic Study. Applied Sciences. 2021; 11(8):3357. https://doi.org/10.3390/app11083357
Chicago/Turabian StyleHodzic, Amir, Gabriel Bernardino, Damien Legallois, Patrick Gendron, Hélène Langet, Mathieu De Craene, Miguel A. González Ballester, Paul Milliez, Hervé Normand, Bart Bijnens, and et al. 2021. "Right Ventricular Global and Regional Remodeling in American-Style Football Athletes: A Longitudinal 3D Echocardiographic Study" Applied Sciences 11, no. 8: 3357. https://doi.org/10.3390/app11083357