
Clinical Characteristics and Outcomes in 314 Japanese Patients with Bacterial Endophthalmitis: A Multicenter Cohort Study from J-CREST

 ,
,  ,
,  , , , , , , , and add
Show full author list
, , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Better Vision Group versus Legal Blindness Group
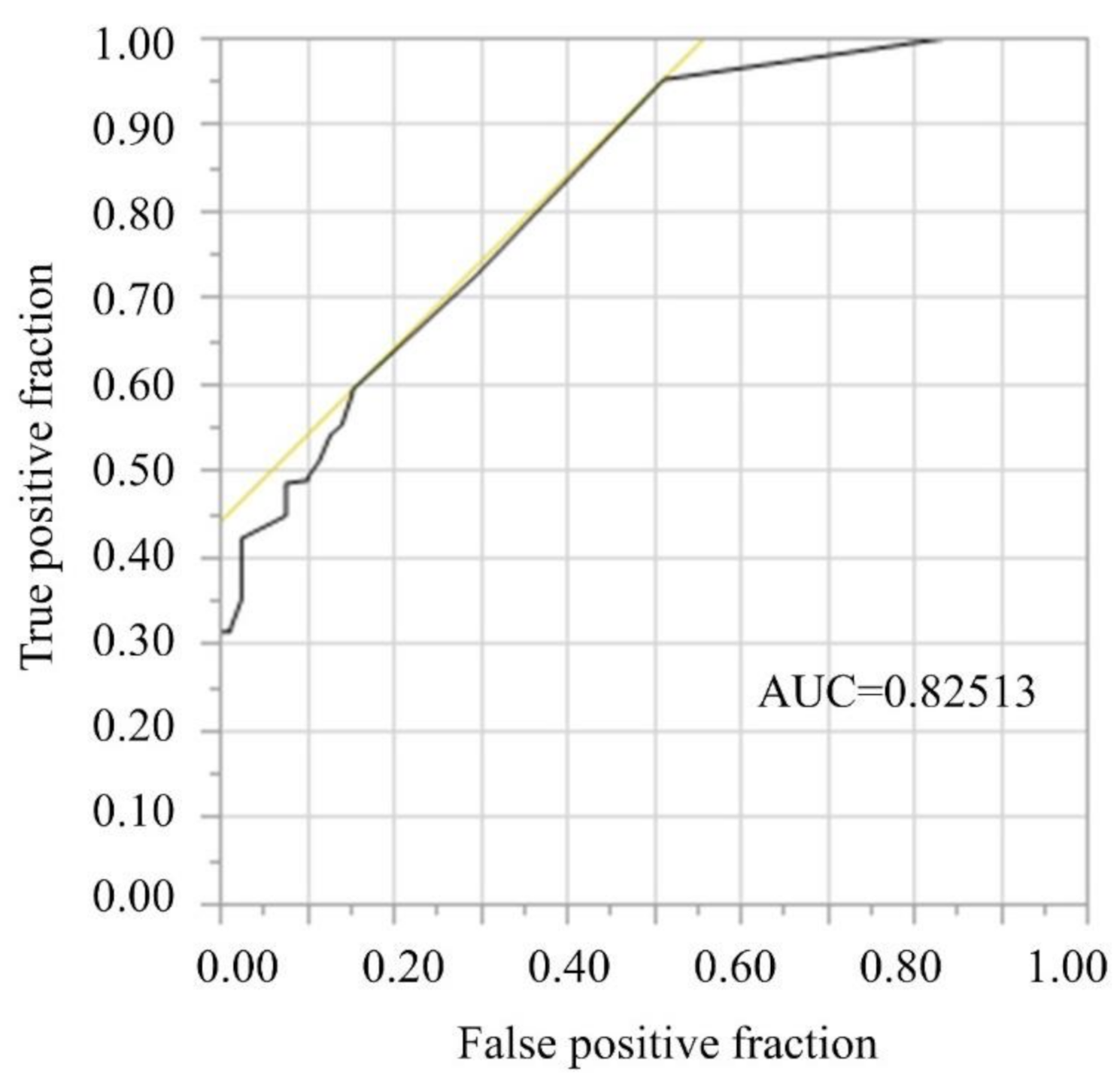
2.3. Primary Endpoint: Contribution of Initial BCVA to Visual Prognosis
2.4. Secondary Endpoints: Exogenous versus Endogenous Endophthalmitis
2.5. Secondary Endpoints: Analyses of pathogens
2.6. Secondary Endpoints: Analyses of Selected Treatments
3. Discussion
4. Materials and Methods
4.1. Study Design and Eligibility
4.2. Patients
4.3. Protocol
4.4. Endpoints
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lalwani, G.A.; Flynn, H.W., Jr.; Scott, I.U.; Quinn, C.M.; Berrocal, A.M.; Davis, J.L.; Murray, T.G.; Smiddy, W.E.; Miller, D. Acute-onset endophthalmitis after clear corneal cataract surgery (1996–2005). Clinical features, causative organisms, and visual acuity outcomes. Ophthalmology 2008, 115, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Pietras-Baczewska, A.; Jasińska, E.; Toro, M.D.; Bonfiglio, V.; Reibaldi, M.; Avitabile, T.; Nowomiejska, K.; Rejdak, R. Urgent Vitrectomy with Vancomycin Infusion, Silicone Oil Endotamponade, and General Antibiotic Treatment in Multiple Cases of Endophthalmitis from a Single Day of Intravitreal Injections—Case Series. J. Clin Med. 2021, 10, 1059. [Google Scholar] [CrossRef]
- Ben Artsi, E.; Katz, G.; Kinori, M.; Moisseiev, J. Endophthalmitis today: A multispecialty ophthalmology department perspective. Eur. J. Ophthalmol. 2016, 26, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Kitsche, M.; Herber, R.; Pillunat, L.E.; Terai, N. Clinical and visual outcome of endophthalmitis patients: A single-center experience. Graef. Arch. Clin. Exp. 2020, 258, 183–189. [Google Scholar] [CrossRef]
- Malmin, A.; Syre, H.; Ushakova, A.; Utheim, T.P.; Forsaa, V.A. Twenty years of endophthalmitis: Incidence, aetiology and clinical outcome. Acta Ophthalmol. 2021, 99, e62–e69. [Google Scholar] [CrossRef]
- Wong, J.S.; Chan, T.K.; Lee, H.M.; Chee, S.P. Endogenous bacterial endophthalmitis: An east Asian experience and a reappraisal of a severe ocular affliction. Ophthalmology. 2000, 107, 1483–1491. [Google Scholar] [CrossRef]
- Yang, X.B.; Liu, Y.Y.; Huang, Z.X.; Mao, Y.; Zhao, L.; Xu, Z.P. Clinical analysis of 1593 patients with infectious endophthalmitis: A 12-year study at a tertiary referral center in western China. Chin. Med. J. 2018, 131, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lin, L.; Li, Y.; Jiang, Z.; Li, C.; Liu, M.; Duan, F.; Lin, X. Etiology, microbiological isolates, and antibiotic susceptibilities in culture-proven pediatric endophthalmitis: A 9-year review. Graef. Arch. Clin. Exp. 2021, 259, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Ben Ghezala, I.; Mariet, A.S.; Benzenine, E.; Bron, A.M.; Baudin, F.; Daien, V.; Korobelnik, J.F.; Quantin, C.; Creuzot-Garcher, C. Incidence of acute postoperative endophthalmitis following macular surgery in France between 2006 and 2016. Acta Ophthalmol. 2020, 98, e333–e338. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.J.; El-Defrawy, S.R.; Gill, S.S.; Whitehead, M.; Campbell, E.; Hooper, P.L.; Bell, C.M.; Ten Hove, M.W. Association of cataract surgical outcomes with late surgeon career stages: A population-based cohort study. JAMA Ophthalmol. 2019, 137, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Li, Y.H.; Lin, Y.J.; Chen, Y.P.; Wang, N.K.; Chao, A.N.; Liu, L.; Wu, W.C.; Lai, C.C.; Chen, T.L.; et al. Prognostic factors and visual outcomes of pyogenic liver abscess-related endogenous Klebsiella pneumoniae endophthalmitis: A 20-year retrospective review. Sci. Rep. 2019, 9, 1071. [Google Scholar] [CrossRef]
- Inoue, T.; Uno, T.; Usui, N.; Kobayakawa, S.; Ichihara, K.; Ohashi, Y.; Japanese Prospective Multicenter Study Group for Postoperative Endophthalmitis after Cataract Surgery. Incidence of endophthalmitis and the perioperative practices of cataract surgery in Japan: Japanese Prospective Multicenter Study for Postoperative Endophthalmitis after Cataract Surgery. Jpn. J. Ophthalmol. 2018, 62, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Kannan, N.B.; Sen, S.; Mishra, C.; Lalitha, P.; Rameshkumar, G.; Rajan, R.P.; Arumugam, K.K.; Ramasamy, K. Comparative study of microbiological profile and management outcomes of acute endophthalmitis after microincision vitrectomy surgery versus intravitreal injections. Ocul. Immunol. Inflamm. 2020, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.C.; Tseng, W.C.; Pao, S.I.; Wong, C.S.; Huang, R.C.; Chan, W.H.; Wu, Z.F. Relationship between anesthesia and postoperative endophthalmitis: A retrospective study. Medicine. 2017, 96, e6455. [Google Scholar] [CrossRef] [PubMed]
- Madan, S.; Kapoor, M.; Pal, H.; Singh, P. Delayed-onset postoperative endophthalmitis. J. Cataract Refract. Surg. 2020, 46, 1064–1065. [Google Scholar] [CrossRef] [PubMed]
- Morioka, M.; Takamura, Y.; Nagai, K.; Yoshida, S.; Mori, J.; Takeuchi, M.; Sawada, T.; Sone, K.; Fukuyama, H.; Kusuhara, S.; et al. Incidence of endophthalmitis after intravitreal injection of an anti-VEGF agent with or without topical antibiotics. Sci. Rep. 2020, 10, 22122. [Google Scholar] [CrossRef] [PubMed]
- Oshima, Y.; Kadonosono, K.; Yamaji, H.; Inoue, M.; Yoshida, M.; Kimura, H.; Ohji, M.; Shiraga, F.; Hamasaki, T.; Japan Microincision Vitrectomy Surgery Study Group. Multicenter survey with a systematic overview of acute-onset endophthalmitis after transconjunctival microincision vitrectomy surgery. Am. J. Ophthalmol. 2010, 150, 716–725.e1. [Google Scholar] [CrossRef] [PubMed]
- Pershing, S.; Lum, F.; Hsu, S.; Kelly, S.; Chiang, M.F.; Rich, W.L., 3rd; Parke, D.W., 2nd. Endophthalmitis after cataract surgery in the United States: A report from the Intelligent Research in Sight Registry, 2013–2017. Ophthalmology 2020, 127, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Simonsz, H.J.; Rutar, T.; Kraft, S.; Thiadens, A.; Batstra, M.R.; Verdijk, R.M.; Loeffler, K.U.; Kommerell, G.; Endophthalmitis-after-Strabismus-Surgery Reporting Group. Endophthalmitis after strabismus surgery: Incidence and outcome in relation to age, operated eye muscle, surgical technique, scleral perforation and immune state. Acta Ophthalmol. 2021, 99, 37–51. [Google Scholar] [CrossRef]
- Stem, M.S.; Rao, P.; Lee, I.J.; Woodward, M.A.; Faia, L.J.; Wolfe, J.D.; Capone, A., Jr.; Covert, D.; Dass, A.B.; Drenser, K.A.; et al. Predictors of endophthalmitis after intravitreal injection: A multivariable analysis based on injection protocol and povidone iodine strength. Ophthalmol. Retina 2019, 3, 3–7. [Google Scholar] [CrossRef]
- Xu, K.; Chin, E.K.; Bennett, S.R.; Williams, D.F.; Ryan, E.H.; Dev, S.; Mittra, R.A.; Quiram, P.A.; Davies, J.B.; Parke, D.W., 3rd; et al. Endophthalmitis after intravitreal injection of vascular endothelial growth factor inhibitors: Management and visual outcomes. Ophthalmology 2018, 125, 1279–1286. [Google Scholar] [PubMed]
- Zhu, Y.; Chen, X.; Chen, P.; Wu, J.; Hua, H.; Yao, K. The occurrence rate of acute-onset postoperative endophthalmitis after cataract surgery in Chinese small- and medium-scale departments of ophthalmology. Sci. Rep. 2017, 7, 40776. [Google Scholar] [CrossRef]
- Dossarps, D.; Bron, A.M.; Koehrer, P.; Aho-Glele, L.S.; Creuzot-Garcher, C. FRCR net (FRenCh Retina specialists net). Endophthalmitis after intravitreal injections: Incidence, presentation, management, and visual outcome. Am. J. Ophthalmol. 2015, 160, 17–25.e1. [Google Scholar] [CrossRef] [PubMed]
- Danielescu, C.; Anton, N.; Stanca, H.T.; Munteanu, M. Endogenous endophthalmitis: A review of case series published between 2011 and 2020. J. Ophthalmol. 2020, 2020, 8869590. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Xia, H.; Jin, C.; Chen, W.; Siu-Chun Ng, D.; Yan, H.; Chen, H. Prognostic factors associated with visual outcome of salvageable eyes with posttraumatic endophthalmitis. Sci. Rep. 2019, 9, 12678. [Google Scholar] [PubMed]
- Okamoto, Y.; Morikawa, S.; Okamoto, F.; Inomoto, N.; Ishikawa, H.; Ueda, T.; Sakamoto, T.; Sugitani, K.; Oshika, T. Clinical characteristics and outcomes of open globe injuries in Japan. Jpn. J. Ophthalmol. 2019, 63, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, S.S.; la Cour, M. 59 eyes with endogenous endophthalmitis- causes, outcomes and mortality in a Danish population between 2000 and 2016. Graef. Arch. Clin. Exp. 2017, 255, 2023–2027. [Google Scholar] [CrossRef]
- Cunningham, E.T.; Flynn, H.W.; Relhan, N.; Zierhut, M. Endogenous endophthalmitis. Ocul. Immunol. Inflamm. 2018, 26, 491–495. [Google Scholar] [PubMed]
- Gounder, P.A.; Hille, D.M.; Khoo, Y.J.; Phagura, R.S.; Chen, F.K. Endogenous endophthalmitis in western Australia: A sixteen-year retrospective study. Retina 2020, 40, 908–918. [Google Scholar] [CrossRef]
- Hsieh, M.C.; Chen, S.N.; Cheng, C.Y.; Li, K.H.; Chuang, C.C.; Wu, J.S.; Lee, S.T.; Chiu, S.L. Clinicomicrobiological profile, visual outcome and mortality of culture-proven endogenous endophthalmitis in Taiwan. Sci. Rep. 2020, 10, 12481. [Google Scholar] [CrossRef]
- Maling, S.; King, C.; Davies, N. A British Ophthalmological Surveillance Unit Study on metastatic endogenous endophthalmitis. Eye. 2018, 32, 743–748. [Google Scholar] [PubMed]
- Silpa-Archa, S.; Ponwong, A.; Preble, J.M.; Foster, C.S. Culture-positive endogenous endophthalmitis: An eleven-year retrospective study in the central region of Thailand. Ocul. Immunol. Inflamm. 2018, 26, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Todokoro, D.; Mochizuki, K.; Nishida, T.; Eguchi, H.; Miyamoto, T.; Hattori, T.; Suzuki, T.; Inoue, T.; Nejima, R.; Hoshi, S.; et al. Isolates and antibiotic susceptibilities of endogenous bacterial endophthalmitis: A retrospective multicenter study in Japan. J. Infect. Chemother. 2018, 24, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Uppuluri, A.; Zarbin, M.A.; Budoff, G.; Bhagat, N. Risk factors for endogenous endophthalmitis in hospitalized patients with Candida Fungemia. Ophthalmol. Retina 2020. S2468-6530(20)30412-7. Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Mamah, C.C.; Anyalebechi, O.C.; Onwubiko, S.N.; Okoloagu, M.N.; Maduka-Okafor, F.C.; Ebede, S.O.; Umeh, R.E. Conjunctival bacterial flora and their antibiotic sensitivity among patients scheduled for cataract surgery in a tertiary hospital in south-east Nigeria. Graef. Arch. Clin. Exp. 2021, 259, 443–448. [Google Scholar] [CrossRef]
- Bruttini, C.; Pallone, C.; Verticchio Vercellin, A.; Acerbi, G.; Baschetti, S.; Bruttini, P.; Riva, I.; Quaranta, L. Pre-operative conjunctival flora in patients with local and/or systemic risk factors for post cataract surgery infection in Northern Italy. Eur. J. Ophthalmol. 2020, 1120672120934991, Advance online publication. [Google Scholar] [CrossRef]
- Reibaldi, M.; Avitabile, T.; Bandello, F.; Longo, A.; Bonfiglio, V.; Russo, A.; Castellino, N.; Rejdak, R.; Nowomiejska, K.; Toro, M.; et al. The effectiveness of 0.6% povidone iodine eye drops in reducing the conjunctival bacterial load and needle contamination in patients undergoing anti-VEGF intravitreal injection: A prospective, randomized study. J. Clin. Med. 2019, 8, 1031. [Google Scholar] [CrossRef] [PubMed]
- Chiquet, C.; Musson, C.; Aptel, F.; Boisset, S.; Maurin, M. Genetic and phenotypic traits of Staphylococcus epidermidis strains causing postcataract endophthalmitis compared to commensal conjunctival flora. Am. J. Ophthalmol. 2018, 191, 76–82. [Google Scholar] [CrossRef]
- Selva Pandiyan, A.; Siva Ganesa Karthikeyan, R.; Rameshkumar, G.; Sen, S.; Lalitha, P. Identification of bacterial and fungal pathogens by rDNA gene barcoding in vitreous fluids of endophthalmitis patients. Semin. Ophthalmol. 2021, 3, 1–7. [Google Scholar]
- Kosacki, J.; Boisset, S.; Maurin, M.; Cornut, P.L.; Thuret, G.; Hubanova, R.; Vandenesch, F.; Carricajo, A.; Aptel, F.; Chiquet, C.; et al. Specific PCR and quantitative real-time PCR in ocular samples from acute and delayed-onset postoperative endophthalmitis. Am. J. Ophthalmol. 2020, 212, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Chun, L.Y.; Dolle-Molle, L.; Bethel, C.; Dimitroyannis, R.C.; Williams, B.L.; Schechet, S.A.; Hariprasad, S.M.; Missiakas, D.; Schneewind, O.; Beavis, K.G.; et al. Rapid pathogen identification and antimicrobial susceptibility testing in in vitro endophthalmitis with matrix assisted laser desorption-ionization Time-of-Flight Mass Spectrometry and VITEK 2 without prior culture. PLoS ONE 2019, 14, e0227071. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Zhou, C.; Zhang, P.; Feng, C.; Zhang, T.; Sun, Z.; Zhuang, H.; Chen, H.; Chang, Q.; Jiang, R.; et al. Diagnostic performance of MALDI-TOF MS compared to conventional microbiological cultures in patients with suspected endophthalmitis. Ocul. Immunol. Inflamm. 2020, 28, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Yannuzzi, N.A.; Patel, N.A.; Relhan, N.; Tran, K.D.; Si, N.; Albini, T.A.; Berrocal, A.M.; Davis, J.L.; Smiddy, W.E.; Townsend, J.; et al. Clinical features, antibiotic susceptibilities, and treatment outcomes of endophthalmitis caused by Staphylococcus epidermidis. Ophthalmol. Retina 2018, 2, 396–400. [Google Scholar] [CrossRef]
- Dave, V.P.; Pathengay, A.; Braimah, I.Z.; Panchal, B.; Sharma, S.; Pappuru, R.R.; Mathai, A.; Tyagi, M.; Narayanan, R.; Jalali, S.; et al. ENTEROCOCCUS ENDOPHTHALMITIS: Clinical settings, antimicrobial susceptibility, and management outcomes. Retina 2020, 40, 898–902. [Google Scholar] [CrossRef]
- Soliman, M.K.; Gini, G.; Kuhn, F.; Parolini, B.; Ozdek, S.; Adelman, R.A.; Sallam, A.B.; European Vitreo-Retinal Society (EVRS) Endophthalmitis Study Group. Visual outcome of early vitrectomy and intravitreal antibiotics in acute postsurgical and postintravitreal injection endophthalmitis: European Vitreo-Retinal Society Endophthalmitis Study Report Two. Retina 2021, 41, 423–430. [Google Scholar] [CrossRef]
- Choi, E.Y.; Han, J.Y.; Lee, H.; Lee, S.C.; Koh, H.J.; Kim, S.S.; Kim, M. Impact of antibiotic resistance of pathogens and early vitrectomy on the prognosis of infectious endophthalmitis: A 10-year retrospective study. Graef. Arch. Clin. Exp. 2019, 257, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Crosby, N.J.; Westcott, M.; Michael, E.; Cunningham, W.J.; Welch, S.; Polkinghorne, P.J. Comparative outcomes of primary vitrectomy versus tap and inject for endophthalmitis following phacoemulsification cataract surgery. Ocul. Immunol. Inflamm. 2020, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Khan, M.; Patrie, J.; Bajwa, A.; Shildkrot, Y.E. Pars plana vitrectomy for endophthalmitis: Microbiologic spectrum and clinical outcomes. Ocul. Immunol. Inflamm. 2020, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, L.J.; Dawkins, R.C.H.; Sheorey, H.; McGuinness, M.B.; Hurley, A.H.; Allen, P.J. Gram-negative endophthalmitis: A prospective study examining the microbiology, clinical associations and visual outcomes following infection. Clin. Exper. Ophthalmol. 2020, 48, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Yokokura, S.; Nishida, T.; Mochizuki, K.; Suzuki, T.; Maruyama, K.; Otomo, T.; Nishiguchi, K.M.; Kunikata, H.; Nakazawa, T. Endogenous endophthalmitis caused by group B streptococcus; case reports and review of 35 reported cases. BMC Ophthalmol. 2020, 20, 126. [Google Scholar] [CrossRef]
- Mochizuki, Y.; Ishikawa, H.; Sato, A.; Yamada, K.; Takesue, Y.; Gomi, F. Pasteurella multocida-induced endophthalmitis after a cat scratch. Am. J. Ophthalmol. Case Rep. 2020, 18, 100711. [Google Scholar] [CrossRef] [PubMed]
- Congdon, N.; O’Colmain, B.; Klaver, C.C.; Klein, R.; Muñoz, B.; Friedman, D.S.; Kempen, J.; Taylor, H.R.; Mitchell, P.; Eye Diseases Prevalence Research Group. Causes and prevalence of visual impairment among adults in the United States. Arch. Ophthalmol. 2004, 122, 477–485. [Google Scholar] [PubMed]


{kind=link}
| Variables | Mean ± Standard Deviation or Number/Total (%) |
|---|---|
| Age, years | 68.3 ± 15.3 |
| Men | 154/314 (49.0%) |
| Unilateral cases | 278/314 (88.5%) |
| Left eye | 200/350 (57.1%) |
| Exogenous endophthalmitis | 242/350 (69.1%) |
| Duration from the onset to the initial treatment, days | 5.4 ± 18.2 (0–298) |
| Eye pain | 148/347 (42.7%) |
| Ciliary injection | 182/349 (52.1%) |
| Bacteria identified | 117/310 (37.7%) |
| Vitrectomy | 276/349 (79.1%) |
| Initial BCVA a (logMAR b) | 1.48 ± 0.96 |
| Final BCVA (logMAR) | 0.72 ± 0.93 |
| Final BCVA ≤ 1.0 logMAR (Snellen 6/60 or better) | 268/350 (76.6%) |
| Enucleation | 21/350 (6.0%) |
| Variables | Final BCVA a ≤ 1.0 logMAR b (Snellen 6/60 or Better) (Better Vison Group) | Final BCVA > logMAR (Snellen < 6/60) (Social Blindness Group) | p-Values; Univariate | p-Values; Multivariate |
|---|---|---|---|---|
| Age, years | 67.7 ± 15.2 | 69.7 ± 15.1 | 0.24 | |
| Men | 131/271 (48.3%) | 38/79 (48.1%) | 1.00 | |
| Left eye | 149/271 (55.0%) | 51/79 (64.1%) | 0.16 | |
| Exogenous endophthalmitis | 186/271 (68.6%) | 56/79 (70.9%) | 0.78 | |
| Duration from the onset to the initial treatment, days | 4.6 ± 8.6 | 8.1 ± 34.5 | 0.23 | |
| Eye pain | 94/268 (35.1%) | 54/79 (68.4%) | <0.0001 | 0.002 |
| Ciliary injection | 131/270 (48.5%) | 51/79 (64.6%) | 0.01 | 0.25 |
| Bacterial identification | 73/233 (31.3%) | 44/77 (57.1%) | <0.0001 | 0.04 |
| Initial BCVA (logMAR) | 1.25 ± 0.93 | 2.27 ± 0.58 | <0.0001 | <0.0001 |
| Variables | ExE | EnE | p-Values |
|---|---|---|---|
| Age, Years | 69.7 ± 15.2 | 64.8 ± 14.5 | 0.0004 |
| Men | 116/242 (47.9%) | 53/108 (49.1%) | 0.91 |
| Left Eye | 145/242 (59.9%) | 55/108 (50.9%) | 0.13 |
| Duration from the Onset to the Initial Treatment, Days | 4.6 ± 20.2 | 7.8 ± 11.3 | <0.0001 |
| Eye Pain | 123/240 (51.3%) | 25/107 (23.4%) | <0.0001 |
| Ciliary Injection | 146/241 (60.6%) | 36/108 (33.3%) | <0.0001 |
| Bacterial Identification | 82/236 (34.8%) | 35/74 (47.3%) | 0.056 |
| Initial BCVA a (logMAR b) | 1.61 ± 0.90 | 1.18 ± 1.04 | 0.0001 |
| Final BCVA ≤ 1.0 logMAR (Snellen 6/60 or Better) | 183/238 (76.9%) | 85/108 (78.7%) | 0.79 |
| Variables | CoNS a | S. aureusb | Genus Streptococcus | S. pneumoniaec | Enterobacteriaceae | Enterococcus | Other Bacteria | Fungus | p-Values |
|---|---|---|---|---|---|---|---|---|---|
| Age, years | 67.5 ± 2.8 | 67.5 ± 4.2 | 70.4 ± 4.8 | 63.3 ± 7.1 | 68.9 ± 6.5 | 75.8 ± 8.6 | 60.5 ± 5.0 | 70.0 ± 3.9 | 0.97 |
| Men | 21/39 (53.9%) | 8/17 (47.1%) | 5/13 (38.5%) | 4/6 (66.7%) | 3/7 (42.9%) | 1/4 (25.0%) | 7/12 (58.3%) | 11/20 (55.0%) | 0.88 |
| Exogenousendophthalmitis | 39/39 (100%) | 10/17 (58.8%) | 6/13 (46.2%) | 5/6 (83.3%) | 1/7 (14.3%) | 4/4 (100%) | 11/12 (91.7%) | 7/20 (35.0%) | <0.0001 |
| Eye pain | 21/38 (55.3%) | 9/17 (52.9%) | 9/13 (69.2%) | 5/6 (83.3%) | 4/7 (57.1%) | 2/4 (50.0%) | 7/12 (58.3%) | 5/20 (25.0%) | 0.17 |
| Ciliary injection | 20/38 (52.6%) | 11/17 (64.7%) | 10/13 (76.9%) | 4/6 (66.7%) | 4/7 (57.1%) | 2/4 (50.0%) | 10/12 (83.3%) | 10/20 (50.0%) | 0.48 |
| Initial BCVA d (logMAR e) | 1.84 | 2.04 | 2.47 | 2.45 | 2.51 | 2.60 | 1.86 | 1.11 | <0.0001 |
| Final BCVA ≤ 1.0 logMAR (Snellen 6/60 or better) | 34/39 (86.5%) | 12/17 (70.6%) | 4/13 (30.8%) | 1/6 (16.7%) | 3/7 (42.9%) | 0/4 (0%) | 7/12 (58.3%) | 13/20 (65.0%) | <0.0001 |
| Variables | (1) Antibiotics Administration via Eye Drops and/or Systemic (n = 52) | (2) Intravitreal Antibiotics and/or (1) (n = 21) | (3) Vitrectomy and/or (2) (n = 276) | p-Values |
|---|---|---|---|---|
| Age, Years | 62.5 ± 16.3 | 70.6 ± 12.7 | 69.0 ± 15.0 | 0.010 |
| Men | 25/52 (48.1%) | 12/21 (57.1%) | 132/276 (47.8%) | 0.74 |
| Left Eye | 27/52 (51.9%) | 14/21 (66.7%) | 159/276 (57.6%) | 0.51 |
| ExE a | 17/52 (32.7%) | 15/21 (71.4%) | 209/276 (75.7%) | <0.0001 |
| Duration from the Onset to the Initial Treatment, Days | 6.2 ± 9.1 | 7.8 ± 9.9 | 5.1 ± 19.6 | 0.019 |
| Eye Pain | 5/51 (9.8%) | 10/21 (47.6%) | 132/274 (48.2%) | <0.0001 |
| Ciliary Injection | 11/52 (21.2%) | 5/21 (23.8%) | 165/275 (60.0%) | <0.0001 |
| Bacterial Identification | 1/21 (4.8%) | 3/17 (17.7%) | 113/271 (41.7%) | 0.0002 |
| Initial BCVA b (logMAR c) | 0.39 ± 0.71 | 1.10 ± 1.10 | 1.71 ± 0.84 | <0.0001 |
| Final BCVA ≤ 1.0 logMAR (Snellen 6/60 or better) | 47/50 (94.0%) | 14/20 (70.0%) | 206/275 (77.4%) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, H.; Uchida, K.; Takesue, Y.; Mori, J.; Kinoshita, T.; Morikawa, S.; Okamoto, F.; Sawada, T.; Ohji, M.; Kanda, T.; et al. Clinical Characteristics and Outcomes in 314 Japanese Patients with Bacterial Endophthalmitis: A Multicenter Cohort Study from J-CREST. Pathogens 2021, 10, 390. https://doi.org/10.3390/pathogens10040390
Ishikawa H, Uchida K, Takesue Y, Mori J, Kinoshita T, Morikawa S, Okamoto F, Sawada T, Ohji M, Kanda T, et al. Clinical Characteristics and Outcomes in 314 Japanese Patients with Bacterial Endophthalmitis: A Multicenter Cohort Study from J-CREST. Pathogens. 2021; 10(4):390. https://doi.org/10.3390/pathogens10040390
Chicago/Turabian StyleIshikawa, Hiroto, Kazutaka Uchida, Yoshio Takesue, Junya Mori, Takamasa Kinoshita, Shohei Morikawa, Fumiki Okamoto, Tomoko Sawada, Masahito Ohji, Takayuki Kanda, and et al. 2021. "Clinical Characteristics and Outcomes in 314 Japanese Patients with Bacterial Endophthalmitis: A Multicenter Cohort Study from J-CREST" Pathogens 10, no. 4: 390. https://doi.org/10.3390/pathogens10040390