
The Role of IL-9 Polymorphisms and Serum IL-9 Levels in Carcinogenesis and Survival Rate for Laryngeal Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Population
2.3. Selection of Study Population
2.4. SNP Selection
2.5. DNA Extraction
2.6. Genotyping
2.7. Serum IL-9 Levels Measurement
2.8. Quality Control of Genotyping
2.9. Survival Rate
2.10. Statistical Analysis
3. Results
3.1. SNP Analysis
3.2. Haplotype Association with the Predisposition to LSCC Occurrence
3.3. Serum Concentrations of IL-9 in the Control and LSCC Groups
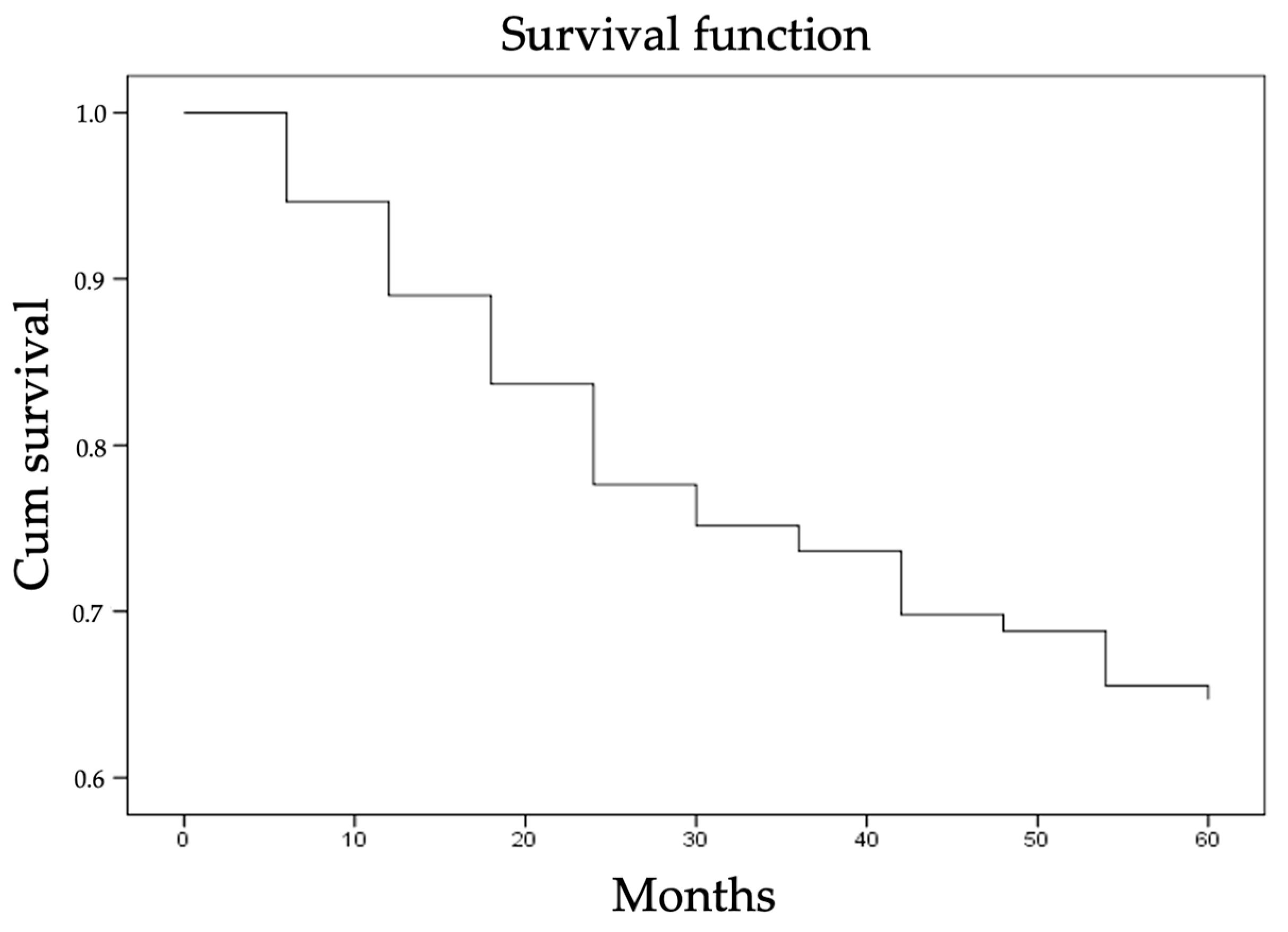
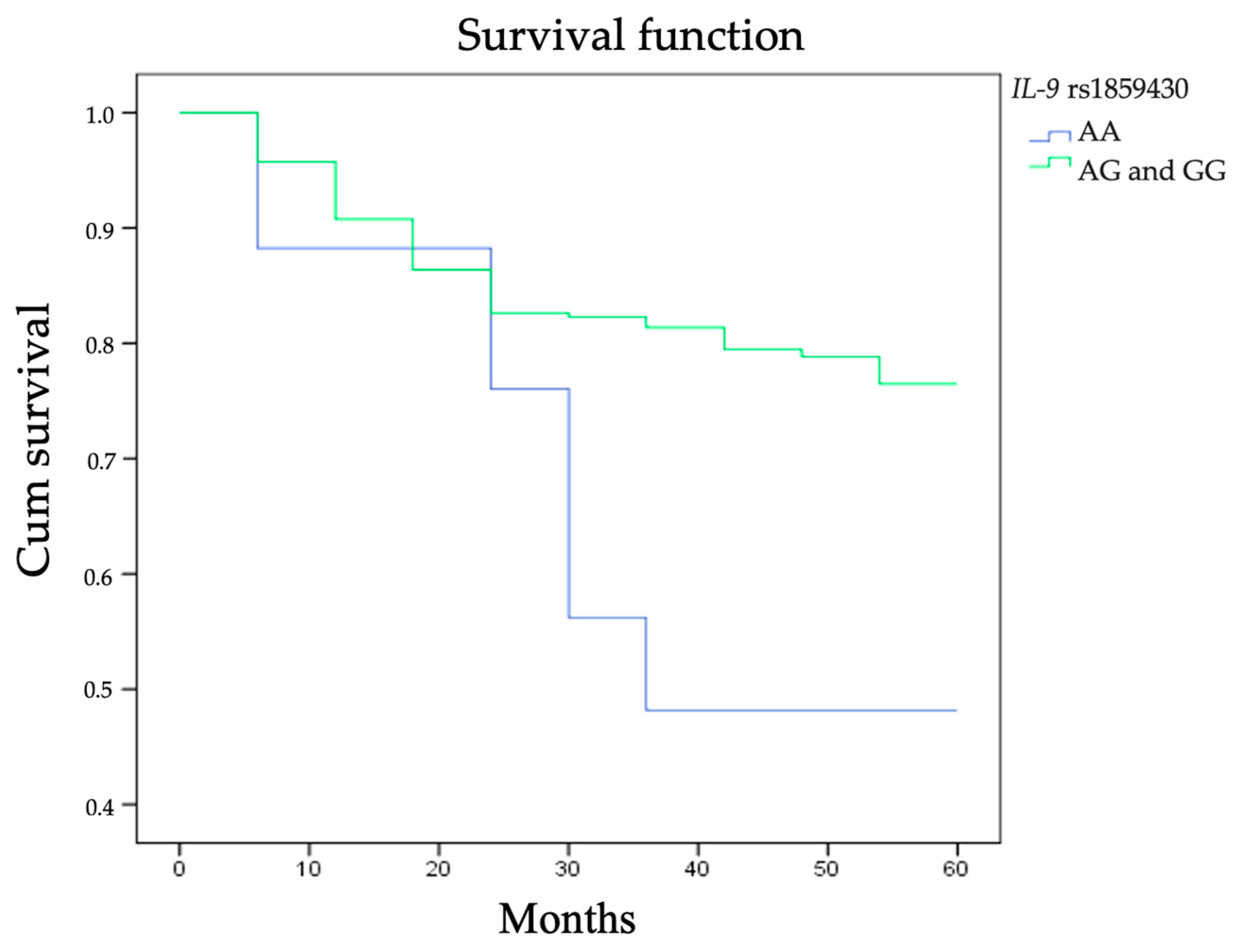
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deng, Y.; Wang, M.; Zhou, L.; Zheng, Y.; Li, N.; Tian, T.; Zhai, Z.; Yang, S.; Hao, Q.; Wu, Y.; et al. Global burden of larynx cancer, 1990–2017: Estimates from the global burden of disease 2017 study. Aging 2020, 12, 2545–2583. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- The Global Cancer Observatory (Globocan 2020): Cancer Fact Sheets. Larynx. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/14-Larynx-fact-sheet.pdf (accessed on 10 January 2021).
- Ciolofan, M.S.; Vlăescu, A.N.; Mogoantă, C.-A.; Ionită, I.; Căpitănescu, A.-N.; Mitroi, M.-R.; Anghelina, F. Clinical, histological and immunohistochemical evaluation of larynx cancer. Curr. Heal. Sci. J. 2017, 43, 367–375. [Google Scholar] [CrossRef]
- Nocini, R.; Molteni, G.; Mattiuzzi, C.; Lippi, G. Updates on larynx cancer epidemiology. Chin. J. Cancer Res. 2020, 32, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Gogarty, D.S.; Shuman, A.; O’Sullivan, E.M.; Sheahan, P.; Kinsella, J.; Timon, C.; O’Neill, J.P. Conceiving a national head and neck cancer screening programme. J. Laryngol. Otol. 2016, 130, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Zhang, S.; Yu, S.; Ma, F.; Bozhi, W.; Zhang, C.; Sun, J.; Mao, X.; Wei, L. Cellular heterogeneity landscape in laryngeal squamous cell carcinoma. Int. J. Cancer 2020, 147, 2879–2890. [Google Scholar] [CrossRef]
- Yang, Y.; Zhou, J.; Wu, H. Significance of cytokeratin-1 single-nucleotide polymorphism and protein level in susceptibility to vocal leukoplakia and laryngeal squamous cell carcinoma. Orl 2019, 81, 121–129. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, W.; Wang, Y.; Wang, N. The PLCE1 rs2274223 variant is associated with the risk of laryngeal squamous cell carcinoma. Int. J. Med. Sci. 2020, 17, 2826–2830. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Tang, D.; Li, S.J.; Zhou, J.; Hsueh, C.-Y.; Zhao, D.-D.; Heng, Y.; Tao, L.; Lu, L.-M. Link between CIITA rs3087456 polymorphism and the risk of laryngeal squamous cell carcinoma in a Chinese population. Pathol. Res. Pract. 2020, 216, 152793. [Google Scholar] [CrossRef]
- Lee, J.E.; Zhu, Z.; Bai, Q.; Brady, T.J.; Xiao, H.; Wakefield, M.R.; Fang, Y. The Role of Interleukin-9 in Cancer. Pathol. Oncol. Res. 2020, 26, 2017–2022. [Google Scholar] [CrossRef]
- Goswami, R.; Kaplan, M.H. A Brief History of IL-9. J. Immunol. 2011, 186, 3283–3288. [Google Scholar] [CrossRef] [Green Version]
- Gounni, A.S.; Nutku, E.; Koussih, L.; Aris, F.; Louahed, J.; Levitt, R.C.; Nicolaides, N.C.; Hamid, Q.H. lL-9 expression by human eosinophils: Regulation by IL-1β and TNF-α. J. Allergy Clin. Immunol. 2000, 106, 460–466. [Google Scholar] [CrossRef]
- Abdelilah, S.G.; Latifa, K.; Esra, N.; Cameron, L.; Bouchaid, L.; Nicolaides, N.C.; Levitt, R.C.; Hamid, Q. Functional expression of IL-9 receptor by human neutrophils from asthmatic donors: Role in IL-8 release. J. Immunol. 2001, 166, 2768–2774. [Google Scholar] [CrossRef]
- Turner, J.E.; Morrison, P.J.; Wilhelm, C.; Wilson, M.; Ahlfors, H.; Renauld, J.-C.; Panzer, U.; Hembly, H.; Stockinger, B. IL-9-mediated survival of type 2 innate lymphoid cells promotes damage control in helminth-induced lung inflammation. J. Exp. Med. 2013, 210, 2951–2965. [Google Scholar] [CrossRef] [Green Version]
- Lauwerys, B.R.; Garot, N.; Renauld, J.-C.; Houssiau, F.A. Cytokine production and killer activity of NK/T-NK cells derived with IL-2, IL-15, or the combination of IL-12 and IL-18. J. Immunol. 2000, 165, 1847–1853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, T.G.; Hallgren, J.; Humbles, A.; Burwell, T.; Finkelman, F.D.; Alcaide, P.; Austen, K.F.; Gurish, M.F. Antigen-induced increases in pulmonary mast cell progenitor numbers depend on IL-9 and CD1d-restricted NKT cells. J. Immunol. 2009, 183, 5251–5260. [Google Scholar] [CrossRef] [PubMed]
- Asao, H.; Okuyama, C.; Kumaki, S.; Ishii, N.; Tsuchiya, S.; Foster, D.; Sugamura, K. Cutting Edge: The common γ-chain is an indispensable subunit of the IL-21 receptor complex. J. Immunol. 2001, 167, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Bauert, J.H.; Lui, K.D.; You, Y.; Lai, S.Y.; Goldsmith, M.A. Heteromerization of the γ(c) chain with the interleukin-9 receptor subunit leads to STAT activation and prevention of apoptosis. J. Biol. Chem. 1998, 273, 9255–9260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerlach, K.; Weigmann, B. The dichotomous function of interleukin-9 in cancer diseases. J. Mol. Med. 2019, 97, 1377–1383. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, F.; Wilhelm, C. More is less: IL-9 in the resolution of inflammation. Immunity 2017, 47, 403–405. [Google Scholar] [CrossRef] [Green Version]
- Zheng, N.; Lu, Y. Targeting the IL-9 pathway in cancer immunotherapy. Hum. Vaccines Immunother. 2020, 16, 2333–2340. [Google Scholar] [CrossRef]
- Vargas, T.R.; Humblin, E.; Végran, F.; Ghiringhelli, F.; Apetoh, L. TH9 cells in anti-tumor immunity. Semin Immunopathol. 2017, 39, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.; Wang, S.; Zhao, L. A tumour-promoting role of Th9 cells in hepatocellular carcinoma through CCL20 and STAT3 pathways. Clin. Exp. Pharmacol. Physiol. 2017, 44, 213–221. [Google Scholar] [CrossRef]
- He, J.; Wang, L.; Zhang, C.; Shen, W.; Zhang, Y.; Liu, T.; Hu, H.; Xie, X.; Luo, F. Interleukin-9 promotes tumorigenesis through augmenting angiogenesis in non-small cell lung cancer. Int. Immunopharmacol. 2019, 75, 105766. [Google Scholar] [CrossRef]
- Hsieh, T.H.; Hsu, C.Y.; Tsai, C.F.; Chiu, C.-C.; Liang, S.-S.; Wang, T.-N.; Kuo, P.-L.; Long, C.-Y.; Tsai, E.-M. A novel cell-penetrating peptide suppresses breast tumorigenesis by inhibiting β-catenin/LEF-1 signaling. Sci. Rep. 2016, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hoelzinger, D.B.; Dominguez, A.L.; Cohen, P.A.; Gendler, S.J. Inhibition of adaptive immunity by IL9 can be disrupted to achieve rapid t-cell sensitization and rejection of progressive tumor challenges. Cancer Res. 2014, 74, 6845–6855. [Google Scholar] [CrossRef] [Green Version]
- Zivancevic-Simonovic, S.; Mihaljevic, O.; Majstorovic, I.; Popovic, S.; Markovic, S.; Milosevic-Djordjevic, O.; Jovanovic, Z.; Mijatovic-Teodorovic, L.; Mihajlovic, D.; Colic, M. Cytokine production in patients with papillary thyroid cancer and associated autoimmune Hashimoto thyroiditis. Cancer Immunol. Immunother. 2015, 64, 1011–1019. [Google Scholar] [CrossRef]
- Fang, Y.; Chen, X.; Bai, Q.; Qin, C.; Mohamoud, A.O.; Zhu, Z.; Ball, T.W.; Ruth, C.M.; Newcomer, D.R.; Herrick, E.J.; et al. IL-9 inhibits HTB-72 melanoma cell growth through upregulation of p21 and TRAIL. J. Surg. Oncol. 2015, 111, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Mateu-Jimenez, M.; Curull, V.; Pijuan, L.; Sanchez-Font, A.; Rivera-Ramos, H.; Rodríguez-Fuster, A.; Auiló, R.; Gea, J.; Barreiro, E. Systemic and tumor Th1 and Th2 inflammatory profile and macrophages in lung cancer: Influence of underlying chronic respiratory disease. J. Thorac. Oncol. 2017, 12, 235–248. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Sun, M.; Zhao, H.; Huang, Y.; Li, D.; Mao, D.; Zhang, Z.; Zhu, X.; Dong, X.; Zhao, X. IL-9 exerts antitumor effects in colon cancer and transforms the tumor microenvironment in vivo. Technol. Cancer Res. Treat. 2019, 18. [Google Scholar] [CrossRef] [Green Version]
- Grabauskas, V.; Klumbienė, J.; Petkevičienė, J.; Šakytė, E.; Kriaučiunionienė, V. Health Behavior among Lithuanian Adult Population, 2012 project. J. Chem. Inf. Model. 2013, 53, 1689–1699. [Google Scholar]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and neck cancers, version 2.2020. JNCCN J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- United Nations Human Rights: UN Treaty Body Database. Ratification Status by Country. Lithuania. Available online: https://tbinternet.ohchr.org/_layouts/15/TreatyBodyExternal/Treaty.aspx?CountryID=101&Lang=EN (accessed on 3 March 2021).
- Kuper, H.; Boffetta, P.; Adami, H.O. Tobacco use and cancer causation: Association by tumour type. J. Intern. Med. 2002, 252, 206–224. [Google Scholar] [CrossRef] [Green Version]
- Boffetta, P.; Hashibe, M. Alcohol and cancer. Lancet Oncol. 2006, 7, 149–156. [Google Scholar] [CrossRef]
- Stell, P.M.; Mcgill, T. Asbestos and laryngeal carcinoma. Lancet. 1973, 302, 416–417. [Google Scholar] [CrossRef]
- Paget-Bailly, S.; Cyr, D.; Luce, D. Occupational exposures and cancer of the larynx-systematic review and meta-analysis. J. Occup. Environ. Med. 2012, 54, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Di Maso, M.; Talamini, R.; Bosetti, C.; Montella, M.; Zucchetto, A.; Libra, M.; Negri, E.; Levi, F.; La Vecchia, C.; Franceschi, S. Red meat and cancer risk in a network of case-control studies focusing on cooking practices. Ann. Oncol. 2013, 24, 3107–3112. [Google Scholar] [CrossRef]
- Gama, R.R.; Carvalho, A.L.; Filho, A.L.; Scorsato, A.P.; Mendoza-Lopez, R.V.; Rautava, J.; Syrjänen, S.; Syrjänen, K. Detection of human papillomavirus in laryngeal squamous cell carcinoma: Systematic review and meta-analysis. Laryngoscope 2016, 126, 885–893. [Google Scholar] [CrossRef] [Green Version]
- Schuurhof, A.; Bont, L.; Siezen, C.L.E.; Hodemaekers, H.; van Houwelingen, H.C.; Kimman, T.G.; Hoebee, B.; Kimpen, J.L.L.; Janssen, R. Interleukin-9 polymorphism in infants with respiratory syncytial virus infection: An opposite effect in boys and girls. Pediatr. Pulmonol. 2010, 45, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Aschard, H.; Bouzigon, E.; Corda, E.; Ulgen, A.; Dizier, M.-H.; Gormand, F.; Lathrop, M.; Kauffmann, F.; Demenais, F.; EGEA cooperative group. Sex-specific effect of IL9 polymorphisms on lung function and polysensitization. Genes Immun. 2009, 10, 559–565. [Google Scholar] [CrossRef] [Green Version]
- Sordillo, J.E.; Kelly, R.; Bunyavanich, S.; McGeachie, M.; Qiu, W.; Croteau-Chonka, D.; Soto-Quiros, M.; Avila, L.; Celedón, J.C.; Brehm, J.M.; et al. Genome-wide expression profiles identify potential targets for gene-environment interactions in asthma severity. J. Allergy Clin. Immunol. 2015, 136, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatahi, F.; Chaleshtori, A.; Samani, K.G.; Mousavi, S.M.; Zandi, F.; Heydari, S.; Chaleshtori, M.H.; Amiri, M.; Khazraee, H. Assessment of the effects of IL9, IL9R, IL17A, and IL17F gene polymorphisms on women with allergic rhinitis in Shahrekord, Iran. Ann. Med. Health Sci. Res. 2016, 6, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Zhu, W.; Liu, N.; Zhao, Y.; Jia, H.; Cui, B.; Ning, G. Association analysis of polymorphisms in IL-3, IL-4, IL-5, IL-9, and IL-13 with Graves’ disease. J. Endocrinol. Invest. 2010, 33, 751–755. [Google Scholar] [CrossRef]
- Schürks, M.; Kurth, T.; Buring, J.E.; Zee, R.Y.L. A candidate gene association study of 77 polymorphisms in migraine. J. Pain 2009, 10, 759–766. [Google Scholar] [CrossRef] [Green Version]
- Mickevicius, T.; Vilkeviciute, A.; Glebauskiene, B.; Kriauciuniene, L.; Liutkeviciene, R. Do TRIB1 and IL-9 gene polymorphisms impact the development and manifestation of pituitary adenoma? In Vivo 2020, 34, 2499–2505. [Google Scholar] [CrossRef]
- Solé, X.; Guinó, E.; Valls, J.; Iniesta, R.; Moreno, V. SNPStats: A web tool for the analysis of association studies. Bioinformatics 2006, 22, 1928–1929. [Google Scholar] [CrossRef] [Green Version]
- Turner, S.; Armstrong, L.L.; Bradford, Y.; Carlsnon, C.C.; Crawford, D.C.; Crenshaw, A.T.; de Andrade, M.; Doheny, K.F.; Haines, J.L.; Hayes, G.; et al. Quality control procedures for genome wide association. Curr. Protoc. Hum. Genet. 2011, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradford, C.R.; Ferlito, A.; Devaney, K.O.; Mäkitie, A.A.; Rinaldo, A. Prognostic factors in laryngeal squamous cell carcinoma. Laryngoscope Investig. Otolaryngol. 2020, 5, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthiller, J.; Straif, K.; Agudo, A.; Ahrens, W.; dos Santos, A.B.; Boccia, S.; Cadoni, G.; Canova, C.; Castellsague, X.; Conway, D.; et al. Low frequency of cigarette smoking and the risk of head and neck cancer in the INHANCE consortium pooled analysis. Int. J. Epidemiol. 2016, 45, 835–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, M.; Bijman, M.; Molin, D.; Cormont, F.; Uyttenhove, C.; van Snick, J.; Sundström, C.; Enblad, G.; Nilsson, G. Increased serum levels of interleukin-9 correlate to negative prognostic factors in Hodgkin’s lymphoma. Leukemia 2003, 17, 2513–2516. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, W.D.; Geng, Q.R.; Wang, L.; Chen, X.-Q.; Liu, C.-C.; Lv, Y. Serum levels of interleukin-9 correlate with negative prognostic factors in extranodal NK/T-cell lymphoma. PLoS ONE 2014, 9, e94637. [Google Scholar] [CrossRef]
- Bussu, F.; Graziani, C.; Gallus, R.; Cittadini, A.; Galli, J.; de Corso, E.; di Cintio, G.; Corbi, M.; Almandori, G.; Boninsegna, A.; et al. IFN-γ and other serum cytokines in head and neck squamous cell carcinomas. Acta Otorhinolaryngol. Ital. 2018, 38, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Bu, X.N.; Zhou, Q.; Zhang, J.C.; Ye, Z.J.; Tong, Z.H.; Shi, H.Z. Recruitment and phenotypic characteristics of interleukin 9-Producing CD4+ T cells in malignant pleural effusion. Lung 2013, 191, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.K.; Kim, B.S.; Koh, C.H.; Seok, J.-W.; Park, J.-S.; Shin, K.-S.; Bae, E.-A.; Lee, G.-E.; Jeon, H.; Cho, J.; et al. Glucocorticoid-induced tumor necrosis factor receptor-related protein co-stimulation facilitates tumor regression by inducing IL-9-producing helper T cells. Nat. Med. 2015, 21, 1010–1017. [Google Scholar] [CrossRef] [PubMed]
- Sotirović, J.; Perić, A.; Vojvodić, D.; Baletić, N.; Zaletel, N.; Stanojević, I.; Erdoglija, M.; Milojević, M. Serum cytokine profile of laryngeal squamous cell carcinoma patients. J. Laryngol. Otol. 2017, 131, 455–461. [Google Scholar] [CrossRef]
- The Global Cancer Observatory (Globocan 2018): Cancer Fact Sheets. Larynx. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/14-Larynx-fact-sheet.pdf (accessed on 10 January 2021).
- Giraldi, L.; Leoncini, E.; Pastorino, R.; Wünsch-Filho, V.; de Carvalho, M.; Lopez, R.; Cadoni, G.; Arzani, D.; Petrelli, L.; Matsuo, K.; et al. Alcohol and cigarette consumption predict mortality in patients with head and neck cancer: A pooled analysis within the International Head and Neck Cancer Epidemiology (INHANCE) Consortium. Ann. Oncol. 2017, 28, 2843–2851. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.R. Head and neck cancer. In Goldman’s Cecil Med, 24th ed.; Elsevier: Amsterdam, The Netherlands, 2011; Volume 1, pp. 1257–1264. [Google Scholar] [CrossRef]
- Barber, B.; Dergousoff, J.; Slater, L.; Harris, J.; O’Connell, D.; El-Hakim, H.; Biron, V.L.; Mitchell, N.; Seikaly, H. Depression and survival in patients with head and neck cancer a systematic review. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Vossen, D.M.; Verhagen, C.V.M.; Verheij, M.; Wessels, L.F.A.; Vens, C.; van den Brekel, M.W.M. Comparative genomic analysis of oral versus laryngeal and pharyngeal cancer. Oral Oncol. 2018, 81, 35–44. [Google Scholar] [CrossRef]
- Cadoni, G.; Giraldi, L.; Petrelli, L.; Pandolfini, M.; Giuliani, M.; Paludetti, G.; Pastorino, R.; Leoncini, E.; Arzani, D.; Almadori, G.; et al. Prognostic factors in head and neck cancer: A 10-year retrospetice analysis in a single-institution in Italy. Acta Otorhinolaryngol. Ital. 2017, 37, 458–466. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Group | p-Value 7 | |
|---|---|---|---|
| LSCC 1 n = 300 | Control Group n = 533 | ||
| Male, n (%) | 287 (95.7) | 508 (95.3) | 0.813 * |
| Female, n (%) | 13 (4.3) | 25 (4.7) | |
| Age years; mean (SD) 2 | 62.4 (9.6) | 63.7 (9.6) | 0.054 ** |
| Smoking, n | <0.001 | ||
| Yes | 132 (44.0) | 36 (6.8) | |
| No | 5 (1.7) | 166 (31.1) | |
| Unknown | 163 (54.3) | 331 (62.1) | |
| Alcohol consumption ***, n | <0.001 | ||
| Yes | 107 (35.7) | 108 (20.3) | |
| No | 30 (10.0) | 94 (17.6) | |
| Unknown | 163 (54.3) | 331 62.1) | |
| Stage, n (%) | - | - | |
| I | 109(36.3) | ||
| II | 60 (20.0) | ||
| III | 50 (16.7) | ||
| IV | 81 (27.0) | ||
| T 3, n (%) | - | - | |
| 1 | 112 (37.3) | ||
| 2 | 58 (19.3) | ||
| 3 | 57 (19.1) | ||
| 4 | 73 (24.3) | ||
| N 4, n (%) | - | - | |
| 0 | 242 (80.7) | ||
| 1 | 18 (6.0) | ||
| 2 | 39 (13.0) | ||
| 3 | 1 (0.3) | ||
| M 5, n (%) | |||
| 0 | 297 (99.0) | ||
| 1 | 2 (0.7) | ||
| 2 | 1 (0.3) | ||
| G 6, n (%) | - | - | |
| 1 | 90 (30.0) | ||
| 2 | 183 (61.0) | ||
| 3 | 27 (9.0) | ||
| SNP 1 | Gene Location | Allele Frequencies | Genotype Distribution | p-Value 2 | |
|---|---|---|---|---|---|
| IL-9 rs1859430 | 0.78 G | 0.22 A | 28/183/322 | 0.764 | |
| IL-9 rs2069870 | 5q3 | 0.80 A | 0.20 G | 0/208/325 | <0.001 |
| IL-9 rs11741137 | 0.83 C | 0.17 T | 12/157/364 | 0.301 | |
| IL-9 rs2069885 | 1.1 | 0.83 G | 0.17 A | 1/155/367 | 0.248 |
| IL-9 rs2069884 | 0.83 G | 0.17 T | 1/155/367 | 0.248 | |
| Polymorphism | Control Group n (%) (n = 533) | LSCC 1 n (%) (n = 300) | p-Value 2 |
|---|---|---|---|
| IL-9 rs1859430 | 0.730 | ||
| G/G | 322 (60.4) | 188 (62.7) | |
| G/A | 183 (34.3) | 95 (31.7) | |
| A/A | 28 (5.3) | 17 (5.7) | |
| Total | 533 (100) | 300 (100) | |
| Allele | |||
| G | 827 (77.6) | 471 (78.5) | |
| A | 239 (22.4) | 129 (21.5) | |
| IL-9rs2069870 | 0.443 | ||
| A/A | 325 (61.0) | 191 (63.7) | |
| A/G | 208 (39.0) | 109 (36.3) | |
| G/G | - | - | |
| Total | 533 (100) | 300 (100) | |
| Allele | |||
| A | 858 (80.5) | 491 (81.8) | |
| G | 208 (19.5) | 109 (18.2) | |
| IL-9rs11741137 | 0.633 | ||
| C/C | 364 (68.3) | 210 (70.0) | |
| C/T | 157 (29.5) | 81 (27.0) | |
| T/T | 12 (2.3) | 9 (3.0) | |
| Total | 533 (100) | 300 (100) | |
| Allele | |||
| C | 885 (83.0) | 501 (83.5) | |
| T | 181 (17.0) | 99 (16.5) | |
| IL-9rs2069885 | 0.744 | ||
| G/G | 367 (68.9) | 213 (71.0) | |
| G/A | 155 (29.1) | 78 (26.0) | |
| A/A | 11 (2.1) | 9 (3.0) | |
| Total | 533 (100) | 300 (100) | |
| Allele | |||
| G | 889 (83.4) | 504 (84.0) | |
| A | 177 (16.6) | 96 (16.0) | |
| IL-9rs2069884 | 0.744 | ||
| G/G | 367 (68.9) | 213 (71.0) | |
| G/T | 155 (29.1) | 78 (26.0) | |
| T/T | 11 (2.1) | 9 (3.0) | |
| Total | 533 (100) | 300 (100) | |
| Allele | |||
| G | 889 (83.4) | 504 (84.0) | |
| T | 177 (16.6) | 96 (16.0) |
| IL-9 rs1859430 (D’; r2) 1,2 | IL-9 rs2069870 (D’; r2) 1,2 | IL-9 rs11741137 (D’; r2) 1,2 | IL-9 rs2069885 (D’; r2) 1,2 | IL-9 rs2069884 (D’; r2) 1,2 | |
|---|---|---|---|---|---|
| IL-9 rs1859430 (D’; r2) 1,2 | 0.9236; 0.7071 | 0.8768; 0.5477 | 0.8987; 0.5583 | 0.8987 0.5583 | |
| IL-9 rs2069870 (D’; r2) 1,2 | 0.7937; 0.5417 | 0.8273; 0.5708 | 0.8273; 0.5708 | ||
| IL-9 rs11741137 (D’; r2) 1,2 | 0.9777; 0.9272 | 0.9777; 0.9272 | |||
| IL-9 rs2069885 (D’; r2) 1,2 | 0.9995; 0.999 | ||||
| IL-9 rs2069884 (D’; r2) 1,2 |
| IL-9 rs1859430 | IL-9 rs2069870 | IL-9 rs11741137 | IL-9 rs2069885 | IL-9 rs2069884 | Frequency | OR 2 (95 % CI 3) | p-Value 4 | |
|---|---|---|---|---|---|---|---|---|
| 1 | A | G | T | A | T | 0.1332 | 1.01 (0.72–1.41) | 0.95 |
| 2 | A | G | C | G | G | 0.0439 | 0.53 (0.30–0.95) | 0.035 |
| 3 | A | A | C | G | G | 0.0237 | 1.26 (0.65–2.45) | 0.49 |
| 4 | A | A | T | A | T | 0.017 | 0.78 (0.33–1.85) | 0.57 |
| 5 (Rare) 1 | * | * | * | * | * | 0.0266 | 0.74 (0.37–1.49) | 0.40 |
| Polymorphism | Genotype | N = 300 (%) | Survival Rate (%) | p-Value 2,* | ||
|---|---|---|---|---|---|---|
| 1-Year LSCC 1-Specific Survival (%) | 3-Year LSCC 1-Specific Survival (%) | 5-Year LSCC 1-Specific Survival (%) | ||||
| IL-9 rs1859430 | AA | 17 (5.7) | 88 | 45 | 45 | 0.188 0.026 ** |
| AG | 95 (31.7) | 81 | 74 | 69 | ||
| GG | 188 (62.6) | 85 | 71 | 65 | ||
| IL-9 rs2069870 | AA | 191 (63.7) | 84 | 71 | 64 | 0.853 |
| AG | 109 (63.7) | 83 | 68 | 66 | ||
| IL-9 rs1174113 | CC | 210 (70.0) | 85 | 71 | 65 | 0.619 |
| CT | 81 (27.0) | 79 | 67 | 64 | ||
| TT | 9 (3.0) | 100 | 76 | 76 | ||
| IL-9 rs2069885 | AA | 9 (3.0) | 100 | 76 | 76 | 0.640 |
| GA | 78 (26.0) | 79 | 67 | 64 | ||
| GG | 213 (71.0) | 85 | 71 | 65 | ||
| IL-9 rs2069884 | GG | 213 (71.0) | 85 | 71 | 65 | 0.640 |
| GT | 782 (26.0) | 79 | 67 | 64 | ||
| TT | 9 (3.0) | 100 | 76 | 76 | ||
| Variable | HR 1 | Univariate 95% CI 2 | p-Value 6 | |
|---|---|---|---|---|
| T 3 | T2 vs. T1 | 6.879 | 2.747–17.228 | 0.000 |
| T3 vs. T1 | 6.575 | 2.592–16.681 | 0.000 | |
| T4 vs. T1 | 7.644 | 3.134–18.644 | 0.000 | |
| N 4 | N≥1 vs. N = 0 | 2.969 | 1.808–4.877 | 0.000 |
| G 5 | G3 vs. G1 | 0.383 | 0.181–0.812 | 0.023 |
| G3 vs. G2 | 0.418 | 0.213–0.818 | 0.011 | |
| Stage | II vs. I | 6.569 | 2.623–16.454 | 0.000 |
| III vs. I | 6.423 | 2.491–16.559 | 0.000 | |
| IV vs. I | 7.169 | 2.959–17.371 | 0.000 | |
| Smoking ≥25 years vs. <25 years | 2.372 | 0.915–6.147 | 0.046 | |
| Alcohol Users vs. Non-drinkers | 1.670 | 0.644–4.328 | 0.291 | |
| IL-9 rs1859430 AA vs. AG and GG | 2.503 | 1.194–5.246 | 0.015 | |
| Variable | HR 1 | Multivariable 95% CI 2 | p-Value 5 | |
|---|---|---|---|---|
| T 3 | T2 vs. T1 | 6.687 | 2.645–16.904 | 0.000 |
| T3 vs. T1 | 5.941 | 2.313–15.259 | 0.000 | |
| T4 vs. T1 | 6.466 | 2.563–16.313 | 0.000 | |
| N 4 | N ≥ 1 vs. N = 0 | 1.850 | 1.099–3.113 | 0.021 |
| IL-9 rs1859430 AA vs. AG and GG | 2.964 | 1.397–6.285 | 0.005 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasvenskaite, A.; Liutkeviciene, R.; Gedvilaite, G.; Vilkeviciute, A.; Liutkevicius, V.; Uloza, V. The Role of IL-9 Polymorphisms and Serum IL-9 Levels in Carcinogenesis and Survival Rate for Laryngeal Squamous Cell Carcinoma. Cells 2021, 10, 601. https://doi.org/10.3390/cells10030601
Pasvenskaite A, Liutkeviciene R, Gedvilaite G, Vilkeviciute A, Liutkevicius V, Uloza V. The Role of IL-9 Polymorphisms and Serum IL-9 Levels in Carcinogenesis and Survival Rate for Laryngeal Squamous Cell Carcinoma. Cells. 2021; 10(3):601. https://doi.org/10.3390/cells10030601
Chicago/Turabian StylePasvenskaite, Agne, Rasa Liutkeviciene, Greta Gedvilaite, Alvita Vilkeviciute, Vykintas Liutkevicius, and Virgilijus Uloza. 2021. "The Role of IL-9 Polymorphisms and Serum IL-9 Levels in Carcinogenesis and Survival Rate for Laryngeal Squamous Cell Carcinoma" Cells 10, no. 3: 601. https://doi.org/10.3390/cells10030601