Rock Climbing Emergencies in the Austrian Alps: Injury Patterns, Risk Analysis and Preventive Measures

 , , and
, , and
Abstract
:1. Background
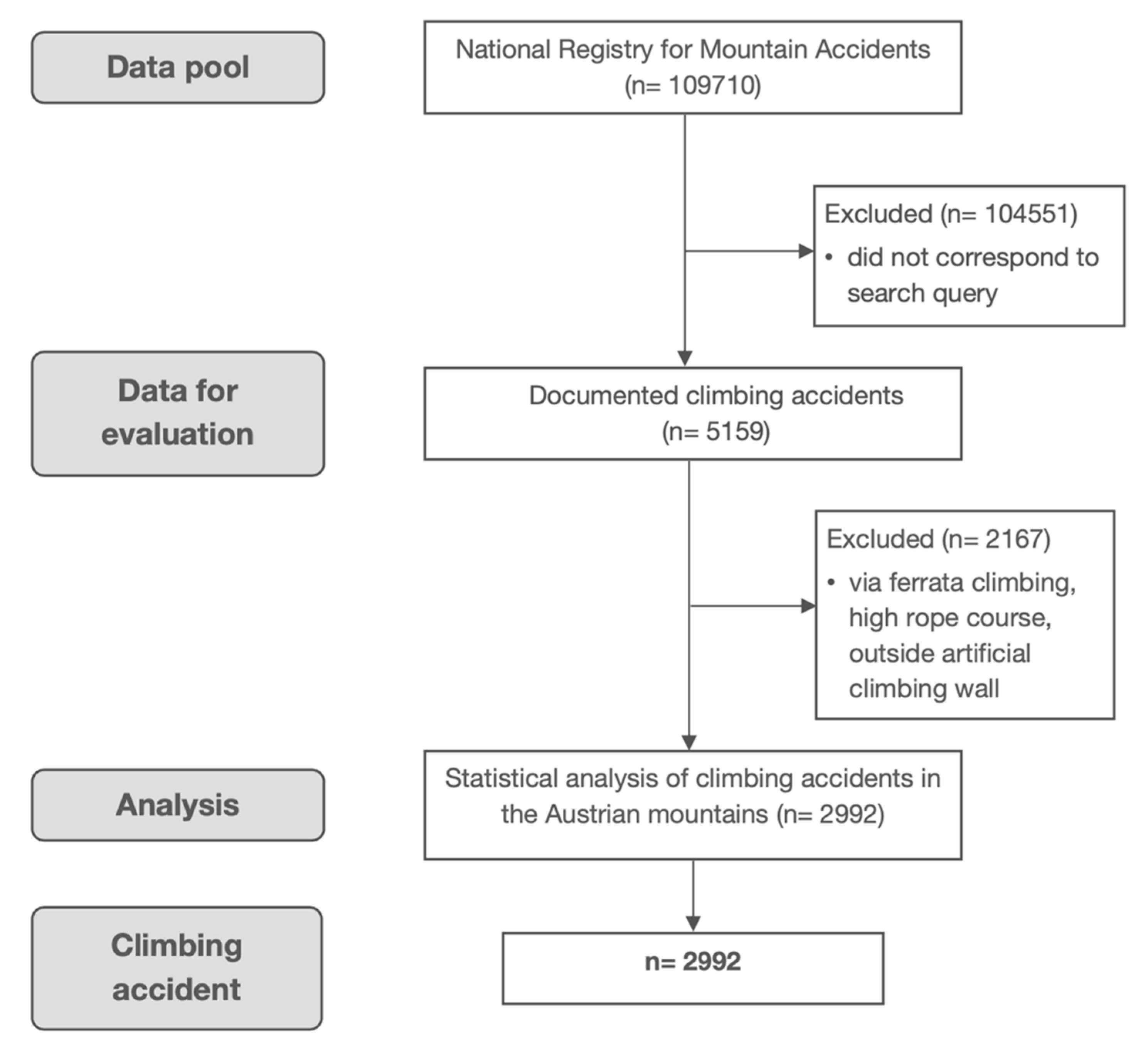
2. Methods
3. Results
3.1. Demographics and General Emergency Characteristics
3.2. Injury Severity and Localization
3.3. Risk Factors for Undesirable Outcome
4. Discussion
4.1. Demographics and General Emergency Characteristics
4.2. Injury Severity and Localization
4.3. Risk Factors for Undesirable Outcome
4.4. Overall Mortality Estimation
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Patient Consent for Publication
Patient and Public Involvement
Data Availability Statement
Abbreviations
Appendix A

{kind=link}
{kind=link}
| Category (n; Undesirable Outcome) | Most Frequent Injury Localization (n) | Most Frequent Causes of Undesirable Outcome (n) | Most Frequent Direct Consequences (n) | Most Frequently Performed Activities (n) | Most Frequently Performed Disciplines (n) |
|---|---|---|---|---|---|
| Age <18 years (n = 22) | Head (6) | Belaying error (7) | Fall with ground impact (15) | Ascent (11) | Alpine (10) |
| Stumble or fall (6) | Injury (3) | Abseiling (7) | Sport (5) | ||
| Rockfall (1) | Fall with rope impact (1) | Descent (2) | Bouldering (2) | ||
| 18–29 yrs. (n = 236) | Ankle (50) | Stumble or fall (35) | Fall with ground impact (89) | Ascent (147) | Alpine (140) |
| Belaying error (30) | Fall with rope impact (76) | Abseiling (48) | Sport (60) | ||
| Rockfall (26) | Injury (46) | Descent (25) | Bouldering (7) | ||
| 30–49 yrs. (n = 403) | Ankle (95) | Grip/Foothold break-out (62) | Fall with rope impact (178) | Ascent (296) | Alpine (269) |
| Stumble or fall (60) | Fall with ground impact (126) | Abseiling (50) | Sport (76) | ||
| Rockfall (50) | Injury (78) | Descent (23) | Ice (11) | ||
| 50–69 yrs. (n = 167) | Multiple trauma (42) | Stumble or fall (29) | Fall with ground impact (67) | Ascent (114) | Alpine (124) |
| Rockfall (20) | Fall with rope impact (51) | Abseiling (17) | Sport (21) | ||
| Belaying error (17) | Injury (33) | Descent (16) | Bouldering (1) | ||
| >70 yrs. (n = 19) | Multiple trauma (9) | Stumble or fall (5) | Fall with ground impact (12) | Ascent (9) | Alpine (12) |
| Grip/Foothold break-out (2) | Fall with rope impact (5) | Descent (5) | Sport (3) | ||
| Injury (2) | Traverse (2) | ||||
| Discipline Alpine (n = 556) | Ankle (115) | Grip/Foothold break-out (90) | Fall with rope impact (235) | Ascent (419) | - |
| Rockfall (76) | Fall with ground impact (179) | Abseiling (65) | |||
| Stumble or fall (66) | Injury (94) | Descent (42) | |||
| Sport (n = 165) | Ankle (43) | Belaying error (50) | Fall with ground impact (77) | Ascent (94) | - |
| Stumble or fall (21) | Fall with rope impact (53) | Abseiling (44) | |||
| Rockfall (13) | Injury (25) | Descent (8) | |||
| Ice (n = 16) | Head (4) | Avalanche (4) | Fall with ground impact (7) | Ascent (11) | - |
| Stumble or fall (4) | Fall with rope impact (4) | Descent (3) | |||
| Icefall (3) | Injury (4) | Abseiling (0) | |||
| Bouldering (n = 18) | Ankle (4) | Stumble or fall (14) | Injury (11) | Ascent (12) | - |
| Grip/Foothold break-out (1) | Fall with ground impact (6) | Descent (1) | |||
| Rockfall (1) | Traverse (1) | ||||
| Activity Ascent (n = 578) | Ankle (136) | Grip/Foothold break-out (86) | Fall with rope impact (291) | - | Alpine (419) |
| Stumble or fall (68) | Fall with ground impact (137) | Sport (94) | |||
| Rockfall (68) | Injury (100) | Bouldering (12) | |||
| Abseiling (n = 123) | Ankle (27) | Belaying error (63) | Fall with ground impact (84) | - | Alpine (65) |
| Malfunction belay point (17) | Injury (20) | Sport (44) | |||
| Stumble or fall (13) | Fall with rope impact (7) | Ice (0) | |||
| Descent (n = 71) | Multiple trauma (17) | Stumble or fall (37) | Fall with ground impact (52) | - | Alpine (42) |
| Grip/Foothold break-out (10) | Injury (14) | Sport (8) | |||
| Rockfall (5) | Fall with rope impact (5) | Ice (3) | |||
| Traverse (n = 16) | Head (6) | Stumble or fall (4) | Fall with ground impact (8) | - | Alpine (12) |
| Grip/Foothold break-out (2) | Fall with rope impact (3) | Bouldering (1) | |||
| Rockfall (2) | Injury (3) | Sport (1) | |||
| With helmet (n = 596) | Ankle (141) | Grip/Foothold break-out (82) | Fall with rope impact (267) | Ascent (447) | Alpine (467) |
| Rockfall (79) | Fall with ground impact (160) | Abseiling (71) | Sport (59) | ||
| Stumble or fall (64) | Injury (118) | Descent (34) | Ice (14) | ||
| Without helmet (n = 230) | Head (58) | Stumble or fall (65) | Fall with ground impact (144) | Ascent (118) | Sport (103) |
| Belaying error (49) | Fall with rope impact (38) | Abseiling (51) | Alpine (79) | ||
| Grip/Foothold break out (18) | Injury (37) | Descent (35) | Bouldering (15) | ||
| With rope (n = 639) | Ankle (159) | Belaying error (88) | Fall with rope impact (304) | Ascent (471) | Alpine (436) |
| Grip/Foothold break-out (74) | Fall with ground impact (157) | Abseiling (117) | Sport (142) | ||
| Rockfall (74) | Injury (119) | Descent (16) | Ice (12) | ||
| Without rope (n = 197) | Multiple trauma (58) | Stumble or fall (89) | Fall with ground impact (148) | Ascent (103) | Alpine (117) |
| Grip / Foothold break-out (26) | Injury (40) | Descent (54) | Sport (21) | ||
| Rockfall (22) | Traverse (7) | Bouldering (17) |
References
- Gatterer, H.; Niedermeier, M.; Pocecco, E.; Frühauf, A.; Faulhaber, M.; Menz, V.; Burtscher, J.; Posch, M.; Ruedl, G.; Burtscher, M. Mortality in Different Mountain Sports Activities Primarily Practiced in the Summer Season-A Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schöffl, V.; Morrison, A.; Schöffl, I.; Küpper, T. The epidemiology of injury in mountaineering, rock and ice climbing. Med. Sport Sci. 2012, 58, 17–43. [Google Scholar] [CrossRef] [PubMed]
- Schöffl, V.; Morrison, A.; Schwarz, U.; Schöffl, I.; Küpper, T. Evaluation of injury and fatality risk in rock and ice climbing. Sports Med. 2010, 40, 657–679. [Google Scholar] [CrossRef] [PubMed]
- Addiss, D.G.; Baker, S.P. Mountaineering and rock climbing injuries in US national parks. Ann. Emerg. Med. 1989, 18, 975–979. [Google Scholar] [CrossRef]
- Bowie, W.S.; Hunt, T.K.; Allen, H.A. Rock climbing injuries in Yosemite National Park. West. J. Med. 1988, 149, 172–177. [Google Scholar]
- Cole, K.P.; Uhl, R.L.; Rosenbaum, A.J. Comprehensive Review of Rock Climbing Injuries. J. Am. Acad. Orthop. Surg. 2020, 28, e501–e509. [Google Scholar] [CrossRef]
- Backe, S.; Ericson, L.; Janson, S.; Timpka, T. Rock climbing injury rates and associated risk factors in a general climbing population. Scand. J. Med. Sci. Sports 2009, 19, 850–856. [Google Scholar] [CrossRef]
- Buzzacott, P.; Schöffl, I.; Chimiak, J.; Schöffl, V. Rock Climbing Injuries Treated in US Emergency Departments, 2008–2016. Wilderness Environ. Med. 2019, 30, 121–128. [Google Scholar] [CrossRef]
- Wyatt, J.P.; McNaughton, G.W.; Grant, P.T. A prospective study of rock climbing injuries. Br. J. Sports Med. 1996, 30, 148–150. [Google Scholar] [CrossRef] [Green Version]
- Woollings, K.Y.; McKay, C.D.; Kang, J.; Meeuwisse, W.H.; Emery, C.A. Incidence, mechanism and risk factors for injury in youth rock climbers. Br. J. Sports Med. 2015, 49, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Schöffl, V.; Popp, D.; Küpper, T.; Schöffl, I. Injury trends in rock climbers: Evaluation of a case series of 911 injuries between 2009 and 2012. Wilderness Environ. Med. 2015, 26, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooks, M.D. Rock climbing injuries. Sports Med. 1997, 23, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Paige, T.E.; Fiore, D.C.; Houston, J.D. Injury in traditional and sport rock climbing. Wilderness Environ. Med. 1998, 9, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Neuhof, A.; Hennig, F.F.; Schöffl, I.; Schöffl, V. Injury risk evaluation in sport climbing. Int. J. Sports Med. 2011, 32, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.E.; Rayan, G.M.; Judd, D.I.; Ding, K.; Stoner, J.A. Survey of Hand and Upper Extremity Injuries Among Rock Climbers. Hand 2017, 12, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Maitland, M. Injuries associated with rock climbing. J. Orthop. Sports Phys. Ther. 1992, 16, 68–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutter, C.; Hotfiel, T.; Tischer, T.; Lenz, R.; Schöffl, V. Evaluation of Rock Climbing Related Injuries in Older Athletes. Wilderness Environ. Med. 2019, 30, 362–368. [Google Scholar] [CrossRef]
- Jones, G.; Asghar, A.; Llewellyn, D.J. The epidemiology of rock climbing injuries. Br. J. Sports Med. 2008, 42, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Gerdes, E.M.; Hafner, J.W.; Aldag, J.C. Injury patterns and safety practices of rock climbers. J. Trauma 2006, 61, 1517–1525. [Google Scholar] [CrossRef]
- Schussman, L.C.; Lutz, L.J. Mountaineering and Rock climbing Accidents. Phys. Sportsmed. 1982, 10, 52–61. [Google Scholar] [CrossRef]
- Lack, D.A.; Sheets, A.L.; Entin, J.M.; Christenson, D.C. Rock climbing rescues: Causes, injuries, and trends in Boulder County, Colorado. Wilderness Environ. Med. 2012, 23, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Rauch, S.; Wallner, B.; Ströhle, M.; Dal Cappello, T.; Brodmann Maeder, M. Climbing Accidents—Prospective Data Analysis from the International Alpine Trauma Registry and Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2019, 17, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- State of Austria Bundesgesetz vom 23. Jänner 1974 über die mit Gerichtlicher Strafe Bedrohten Handlungen (Strafgesetzbuch—StGB) StF: BGBl. Nr. 60/1974. Available online: https://www.ris.bka.gv.at/GeltendeFassung.wxe?Abfrage=Bundesnormen&Gesetzesnummer=10002296 (accessed on 10 June 2020).
- Schöffl, V.; Morrison, A.; Hefti, U.; Ullrich, S.; Küpper, T. The UIAA Medical Commission Injury Classification for Mountaineering and Climbing Sports. Wilderness Environ. Med. 2011, 22, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Bernard, M.; Wright, R.; Anderson, H.; Bernard, A. Wilderness Falls: An Analysis and Comparison of Rock Climbers and Nonclimbers. J. Surg. Res. 2019, 234, 149–154. [Google Scholar] [CrossRef] [Green Version]
- Bannister, P.; Foster, P. Upper limb injuries associated with rock climbing. Br. J. Sports Med. 1986, 20, 55. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.Y.; Torriani, M.; Huang, A.J. Rock Climbing Injuries: Acute and Chronic Repetitive Trauma. Curr. Probl. Diagn. Radiol. 2016, 45, 205–214. [Google Scholar] [CrossRef]
- McDonald, J.W.; Henrie, A.M.; Teramoto, M.; Medina, E.; Willick, S.E. Descriptive Epidemiology, Medical Evaluation, and Outcomes of Rock Climbing Injuries. Wilderness Environ. Med. 2017, 28, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Bollen, S.R. Soft tissue injury in extreme rock climbers. Br. J. Sports Med. 1988, 22, 145–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, A.E.; Troyer, J.L.; Kline, J.A. Cost-effectiveness of an emergency department-based early sepsis resuscitation protocol. Crit. Care Med. 2011, 39, 1306–1312. [Google Scholar] [CrossRef] [Green Version]
- Lutter, C.; Tischer, T.; Cooper, C.; Frank, L.; Hotfiel, T.; Lenz, R.; Schöffl, V. Mechanisms of Acute Knee Injuries in Bouldering and Rock Climbing Athletes. Am. J. Sports Med. 2020, 48, 730–738. [Google Scholar] [CrossRef]
- Schöffl, V.; Küpper, T. Feet injuries in rock climbers. World J. Orthop. 2013, 4, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Hasler, R.M.; Huttner, H.E.; Keel, M.J.; Durrer, B.; Zimmermann, H.; Exadaktylos, A.K.; Benneker, L.M. Spinal and pelvic injuries in airborne sports: A retrospective analysis from a major Swiss trauma centre. Injury 2012, 43, 440–445. [Google Scholar] [CrossRef]
- Locker, T.; Chan, D.; Cross, S. Factors predicting serious injury in rock climbing and non-rock climbing falls. J. Trauma 2004, 57, 1321–1323. [Google Scholar] [CrossRef]
- Goodacre, S.; Than, M.; Goyder, E.C.; Joseph, A.P. Can the distance fallen predict serious injury after a fall from a height? J. Trauma 1999, 46, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Steedman, D.J. Severity of free-fall injury. Injury 1989, 20, 259–261. [Google Scholar] [CrossRef]
- Isbister, E.S.; Roberts, J.A. Autokabalesis: A study of intentional vertical deceleration injuries. Injury 1992, 23, 119–122. [Google Scholar] [CrossRef]
- Ströhle, M.; Beeretz, I.; Rugg, C.; Woyke, S.; Rauch, S.; Paal, P. Canyoning Accidents in Austria from 2005 to 2018. Int. J. Environ. Res. Public Health 2019, 17, 102. [Google Scholar] [CrossRef] [Green Version]
- Ströhle, M.; Haselbacher, M.; Rugg, C.; Walpoth, A.; Konetschny, R.; Paal, P.; Mair, P. Mortality in Via Ferrata Emergencies in Austria from 2008 to 2018. Int. J. Environ. Res. Public Health 2019, 17, 103. [Google Scholar] [CrossRef] [Green Version]
- Forrester, J.D.; Tran, K.; Tennakoon, L.; Staudenmayer, K. Climbing-Related Injury Among Adults in the United States: 5-Year Analysis of the National Emergency Department Sample. Wilderness Environ. Med. 2018, 29, 425–430. [Google Scholar] [CrossRef] [Green Version]


| Emergency Characteristics (n = 2992) | Classification | n (%) |
|---|---|---|
| Cause of emergency | Unknown | 556 (18.6) |
| Lost or trapped | 517 (17.3) | |
| Uninjured companion * | 505 (16.9) | |
| Rockfall | 229 (7.7) | |
| Exhaustion | 187 (6.3) | |
| Stumble and fall | 146 (4.9) | |
| Grip or foothold break-out | 143 (4.8) | |
| Belaying error | 138 (4.6) | |
| Abseiling error | 121 (4.0) | |
| False alarm | 45 (1.5) | |
| Other | 405 (13.5) | |
| Direct consequence of preceding cause | Blockage | 1004 (33.6) |
| None | 550 (18.4) | |
| Fall with rope impact | 497 (16.6) | |
| Direct injury | 429 (14.3) | |
| Fall with ground impact | 379 (12.7) | |
| Unknown | 115 (3.8) | |
| Fall of entire rope team | 18 (0.6) |
| Injury Characteristics (n= 2992) | Classification | n (%) | |
|---|---|---|---|
| Injury severity | Uninjured | UIAA MedCom 0 | 1469 (49.1) |
| Mild | UIAA MedCom 1–2 | 368 (12.3) | |
| Severe | UIAA MedCom 3–5 | 709 (23.7) | |
| Dead | UIAA MedCom 6 | 140 (4.7) | |
| Unknown | Unknown | 306 (10.2) | |
| Emergency classification (1578 entries in n = 1450 patients) | Fracture | 566 (35.9) | |
| Contusion/Strain/Sprain | 264 (16.7) | ||
| Wound/Lesion/Laceration | 250 (15.8) | ||
| Multiple trauma | 150 (9.5) | ||
| Luxation | 97 (6.1) | ||
| Exhaustion | 48 (3.0) | ||
| Concussion | 47 (3.0) | ||
| Hypothermia | 46 (2.9) | ||
| Internal injury | 33 (2.1) | ||
| Unknown | 32 (2.0) | ||
| Burn injury | 12 (0.8) | ||
| Cardiovascular disorder | 12 (0.8) | ||
| Stroke | 1 (0.1) | ||
| Suffocation | 1 (0.1) | ||
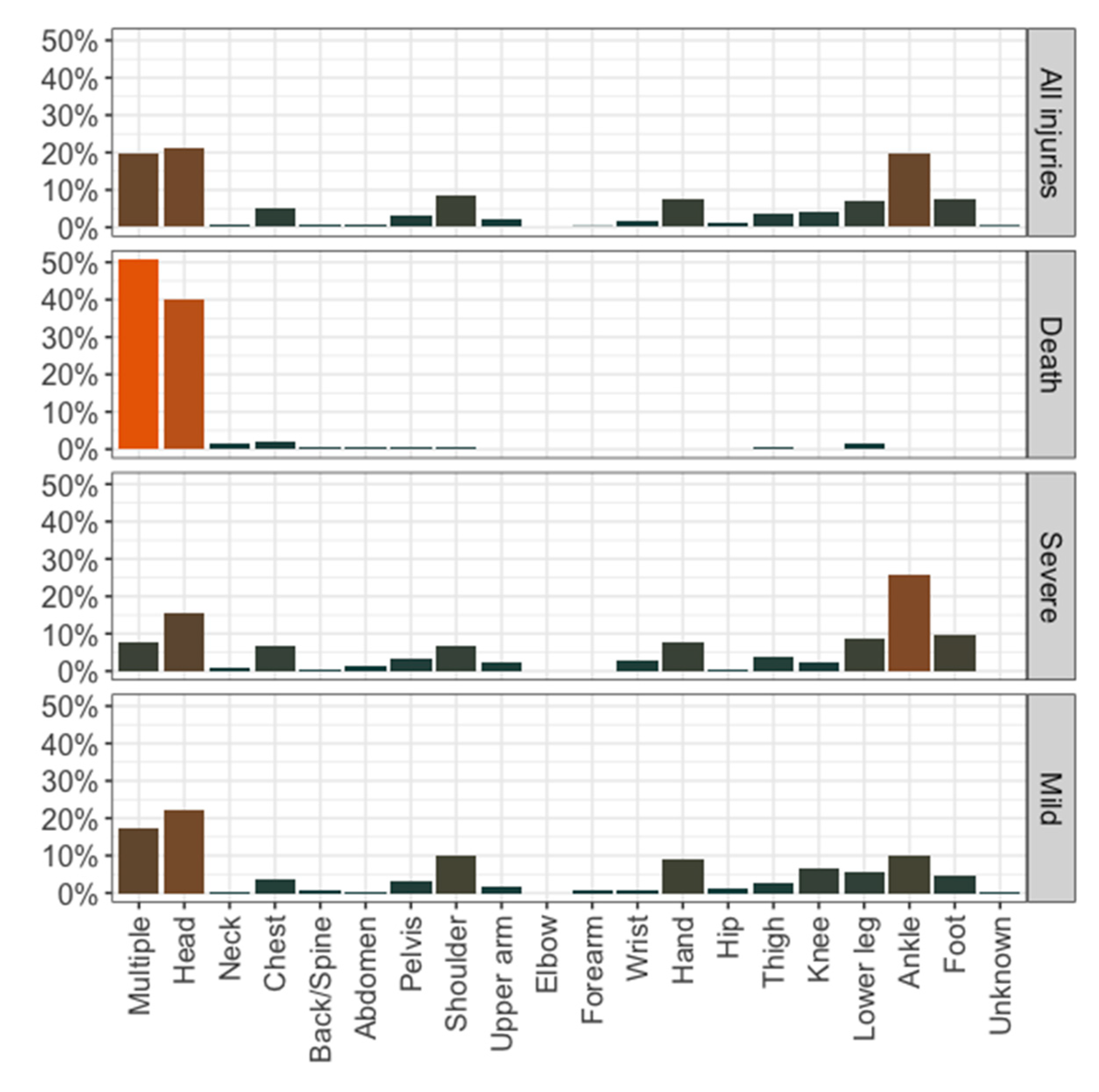
| Injury localization (1503 entries in n = 1315 patients) | Multiple | 257 (19.5) | |
| Head | 279 (21.2) | ||
| Neck | 11 (0.8) | ||
| Chest | 68 (5.2) | ||
| Back/Spine | 5 (0.4) | ||
| Abdomen | 11 (0.8) | ||
| Pelvis | 40 (3.0) | ||
| Shoulder | 114 (8.7) | ||
| Upper arm | 26 (2.0) | ||
| Elbow | 0 (0) | ||
| Forearm | 2 (0.2) | ||
| Wrist | 23 (1.7) | ||
| Hand | 101 (7.7) | ||
| Hip | 13 (1.0) | ||
| Thigh | 46 (3.5) | ||
| Knee | 53 (4.0) | ||
| Lower leg | 91 (6.9) | ||
| Ankle | 259 (19.7) | ||
| Foot | 97 (7.4) | ||
| Unknown | 7 (0.2) | ||
| Category | Total (n) | Severely Injured (%) | Fatally Injured (%) | Odds Ratio | |
|---|---|---|---|---|---|
| (99% CI) | |||||
| Age group § | 18–29 yrs.# | 1028 | 19.6 | 3.3 | |
| <18 yrs. | 93 | 20.4 | 3.2 | 0.97 (0.50–1.90) | |
| 30–49 yrs. | 1371 | 26.5 | 2.9 | 1.48 (1.15–1.89) | |
| 50–69 yrs. | 447 | 25.7 | 11.6 | 2.22 (1.61–3.06) | |
| >70 yrs. | 35 | 22.9 | 31.4 | 4.52 (1.83–11.13) | |
| Climbing discipline + | Alpine # | 2207 | 20.2 | 5 | |
| Sport | 394 | 39.6 | 2.3 | 2.33 (1.73–3.13) | |
| Ice | 36 | 41.7 | 2.8 | 2.56 (1.07–6.17) | |
| Bouldering | 33 | 54.5 | 0 | 4.16 (1.66–10.42) | |
| Activity | Ascent # | 1792 | 27.7 | 4.6 | |
| Abseiling | 506 | 20.9 | 3.4 | 0.65 (0.48–0.89) | |
| Descent | 331 | 15.1 | 6.3 | 0.59 (0.40–0.86) | |
| Traverse | 46 | 26.1 | 8.7 | 1.11 (0.48–2.54) | |
| Use of helmet | With helmet # | 2363 | 21.5 | 3.7 | |
| Without helmet | 549 | 33.2 | 8.7 | 1.81 (1.35–2.43) | |
| Use of rope | With rope # | 2410 | 24.1 | 2.4 | |
| Without rope | 502 | 23.5 | 15.7 | 1.67 (1.35–2.22) | |
| Time of emergency | 12:00–16:00 # | 1461 | 28.2 | 5.2 | |
| 17:00–21:00 | 808 | 10.4 | 1.9 | 0.30 (0.22–0.41) | |
| 22:0006:00 | 88 | 9.1 | 1.1 | 0.26 (0.10–0.65) | |
| 07:00–11:00 | 619 | 32,6 | 7.8 | 1.39 (1.07–1.81) | |
| Height of fall | <5 m # | 85 | 50.6 | 0 | |
| 5–9 m | 111 | 72.1 | 0 | 2.67 (1.20–5.94) | |
| 10–19 m | 101 | 65.3 | 7.9 | 3.07 (1.32–7.12) | |
| >20 m | 88 | 48.9 | 37.5 | 7.52 (2.72–20.74) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rugg, C.; Tiefenthaler, L.; Rauch, S.; Gatterer, H.; Paal, P.; Ströhle, M. Rock Climbing Emergencies in the Austrian Alps: Injury Patterns, Risk Analysis and Preventive Measures. Int. J. Environ. Res. Public Health 2020, 17, 7596. https://doi.org/10.3390/ijerph17207596
Rugg C, Tiefenthaler L, Rauch S, Gatterer H, Paal P, Ströhle M. Rock Climbing Emergencies in the Austrian Alps: Injury Patterns, Risk Analysis and Preventive Measures. International Journal of Environmental Research and Public Health. 2020; 17(20):7596. https://doi.org/10.3390/ijerph17207596
Chicago/Turabian StyleRugg, Christopher, Laura Tiefenthaler, Simon Rauch, Hannes Gatterer, Peter Paal, and Mathias Ströhle. 2020. "Rock Climbing Emergencies in the Austrian Alps: Injury Patterns, Risk Analysis and Preventive Measures" International Journal of Environmental Research and Public Health 17, no. 20: 7596. https://doi.org/10.3390/ijerph17207596