Rehabilitative Ultrasound Imaging Features of the Abdominal Wall Muscles in Elite and Amateur Basketball Players

 ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Sample Size Calculation
2.3. Participants
2.4. Ethical Considerations
2.5. Sociodemographic and Respiratory Distress Data
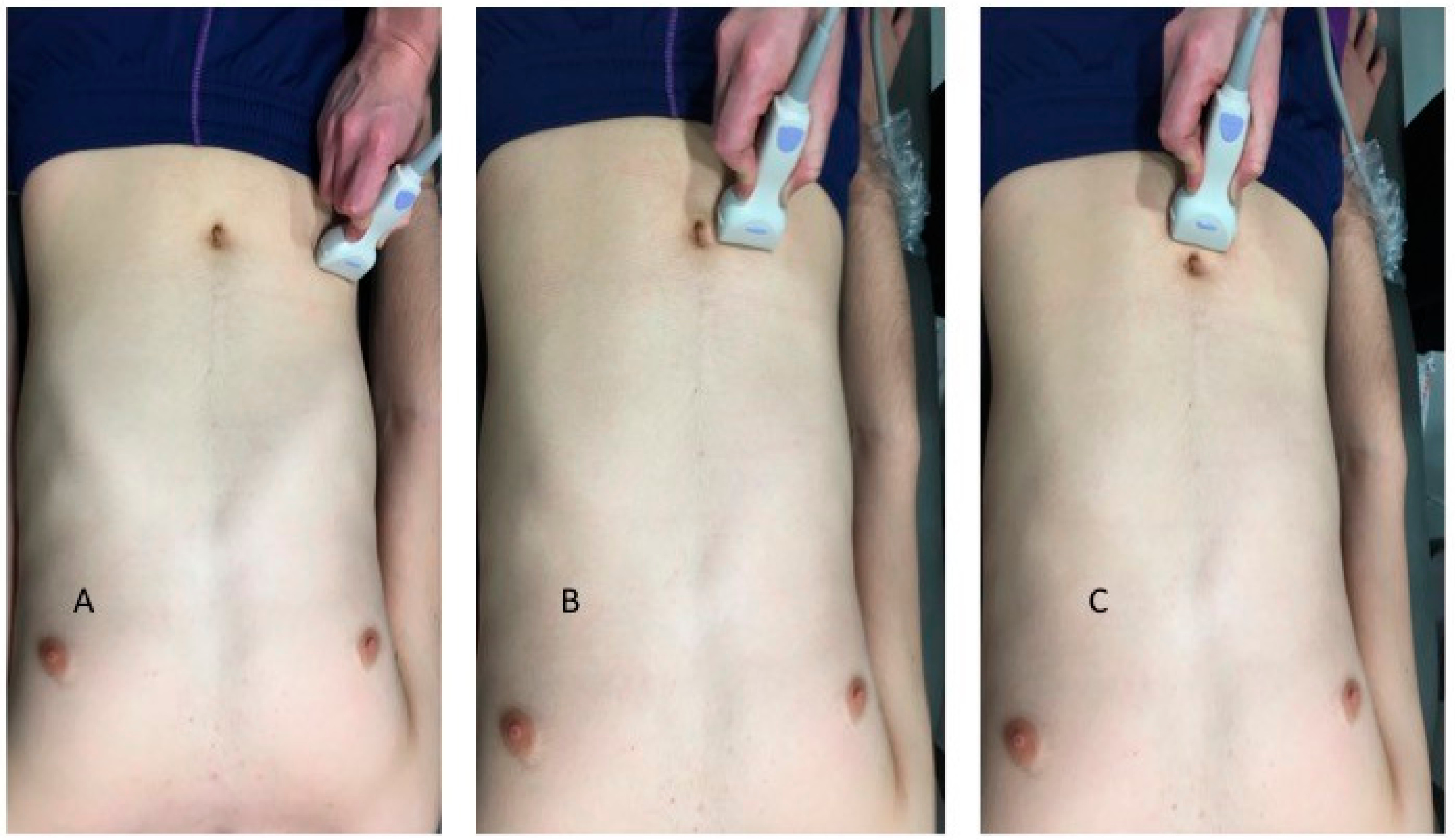
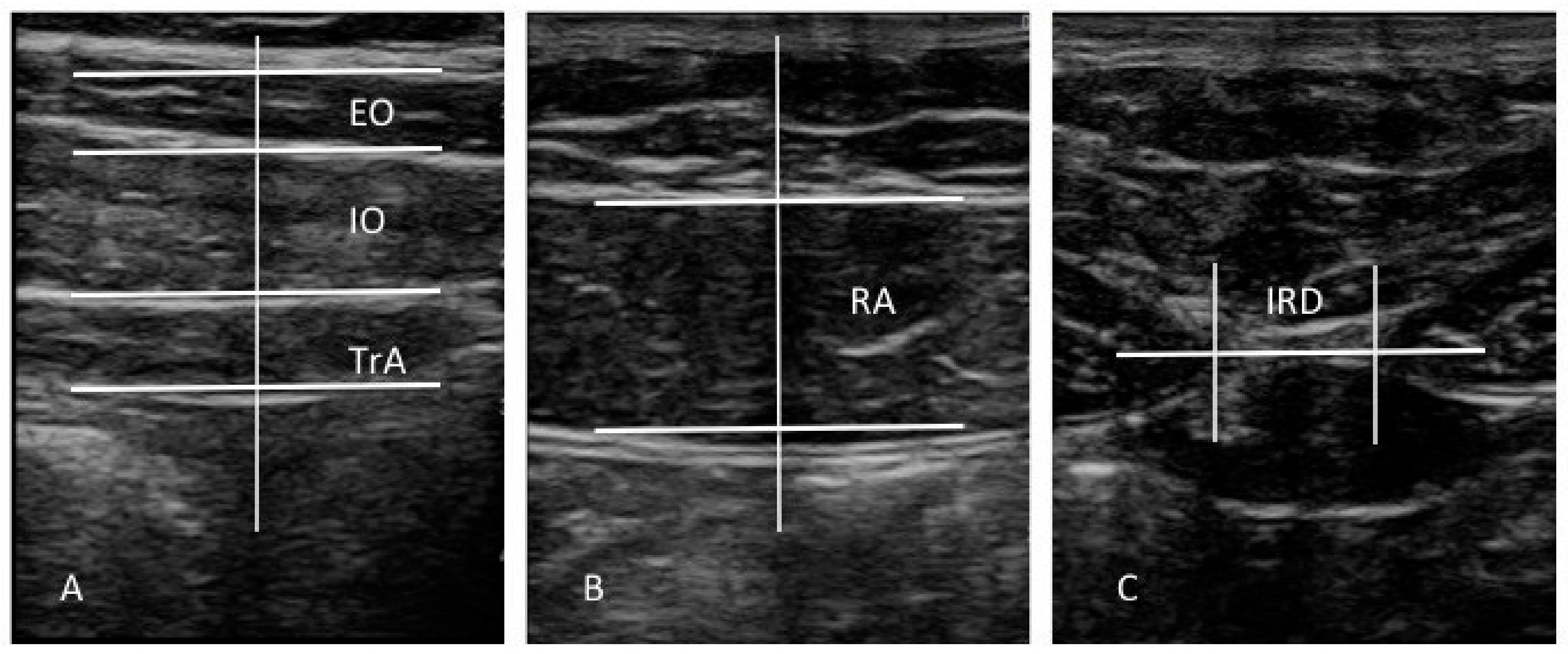
2.6. Ultrasound Imaging of the Abdominal Wall
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Potter, C.L.; Cairns, M.C.; Stokes, M. Use of ultrasound imaging by physiotherapists: A pilot study to survey use, skills and training. Man. Ther. 2012, 17, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Teyhen, D.S. Rehabilitative ultrasound imaging: The roadmap ahead. J. Orthop. Sports Phys. Ther. 2007, 37, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.; Wang, S.S. Comparison of changes in supraspinatus muscle thickness in persons with subacromial impingement syndrome and asymptomatic adults. Physiother. Theory Pract. 2014, 30, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Mohseny, B.; Nijhuis, T.H.; Hundepool, C.A.; Janssen, W.G.; Selles, R.W.; Coert, J.H. Ultrasonographic quantification of intrinsic hand muscle cross-sectional area; reliability and validity for predicting muscle strength. Arch. Phys. Med. Rehabil. 2015, 96, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, M.; Fukumoto, Y.; Kobayashi, M.; Kawasaki, T.; Maegawa, S.; Ibuki, S.; Ichihashi, N. Quantity and Quality of the Lower Extremity Muscles in Women with Knee Osteoarthritis. Ultrasound Med. Biol. 2015, 41, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Lobo, C.C.; Morales, C.R.; Sanz, D.R.; Corbalán, I.S.; Marín, A.G.; López, D.L. Ultrasonography Comparison of Peroneus Muscle Cross-sectional Area in Subjects With or Without Lateral Ankle Sprains. J. Manipulative Physiol. Ther. 2016, 39, 635–644. [Google Scholar] [CrossRef] [PubMed]
- Lobo, C.C.; Marín, A.G.; Sanz, D.R.; López, D.L.; López, P.P.; Morales, C.R.; Corbalán, I.S. Ultrasound evaluation of intrinsic plantar muscles and fascia in hallux valgus: A case-control study. Medicine 2016, 95, e5243. [Google Scholar] [CrossRef] [PubMed]
- Strini, P.J.; Strini, P.J.; Barbosa, T.d.S.; Gavião, M.B. Assessment of thickness and function of masticatory and cervical muscles in adults with and without temporomandibular disorders. Arch. Oral Biol. 2013, 58, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Javanshir, K.; Rezasoltani, A.; Mohseni-Bandpei, M.A.; Amiri, M.; Ortega-Santiago, R.; Fernández-de-Las-Peñas, C. Ultrasound Assessment of Bilateral Longus Colli Muscles in Subjects with Chronic Bilateral Neck Pain. Am. J. Phys. Med. Rehabil. 2011, 90, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Javanshir, K.; Amiri, M.; Mohseni Bandpei, M.A.; De las Penas, C.F.; Rezasoltani, A. The effect of different exercise programs on cervical flexor muscles dimensions in patients with chronic neck pain. J. Back Musculoskelet. Rehabil. 2015, 28, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, K.B.; Underwood, F.B.; Mattacola, C.G.; Matacolla, C.; Nitz, A.J.; Malone, T.R. A comparison of select trunk muscle thickness change between subjects with low back pain classified in the treatment-based classification system and asymptomatic controls. J. Orthop. Sports Phys. Ther. 2007, 37, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L.; Warner, M.B.; Stokes, M. Comparison of the Sonographic Features of the Abdominal Wall Muscles and Connective Tissues in Individuals With and Without Lumbopelvic Pain. J. Orthop. Sport. Phys. Ther. 2013, 43, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.H.M.; Ward, S.R.; Cook, M.S.; Lieber, R.L. Architectural analysis of human abdominal wall muscles: Implications for mechanical function. Spine 2011, 36, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Rankin, G.; Stokes, M.; Newham, D.J. Abdominal muscle size and symmetry in normal subjects. Muscle Nerve 2006, 34, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Teyhen, D.S.; Gill, N.W.; Whittaker, J.L.; Henry, S.M.; Hides, J.A.; Hodges, P. Rehabilitative ultrasound imaging of the abdominal muscles. J. Orthop. Sports Phys. Ther. 2007, 37, 450–466. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.; Wilson, S.; Stanton, W.; McMahon, S.; Keto, H.; McMahon, K.; Bryant, M.; Richardson, C. An MRI Investigation Into the Function of the Transversus Abdominis Muscle During “Drawing-In” of the Abdominal Wall. Spine 2006, 31, E175–E178. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.H.M.; McGill, S.M. A comparison of ultrasound and electromyography measures of force and activation to examine the mechanics of abdominal wall contraction. Clin. Biomech. 2010, 25, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.H.; Ferreira, M.L.; Nascimento, D.P.; Pinto, R.Z.; Franco, M.R.; Hodges, P.W. Discriminative and reliability analyses of ultrasound measurement of abdominal muscles recruitment. Man. Ther. 2011, 16, 463–469. [Google Scholar] [CrossRef] [PubMed]
- John, E.K.; Beith, I.D. Can activity within the external abdominal oblique be measured using real-time ultrasound imaging? Clin. Biomech. 2007, 22, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.A.; Stanton, W.R. Can Motor Control Training Lower the Risk of Injury for Professional Football Players? Med. Sci. Sport. Exerc. 2014, 46, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Olivier, B.; Benjamin, N. Asymmetrical abdominal muscle morphometry is present in injury free adolescent cricket pace bowlers: A prospective observational study. Phys. Ther. Sport 2017, 28, 34–42. [Google Scholar] [CrossRef] [PubMed]
- White, R.G.; Hakim, A.J.; Salganik, M.J.; Spiller, M.W.; Johnston, L.G.; Kerr, L.; Kendall, C.; Drake, A.; Wilson, D.; Orroth, K.; et al. Strengthening the Reporting of Observational Studies in Epidemiology for respondent-driven sampling studies: "STROBE-RDS" statement. J. Clin. Epidemiol. 2015, 68, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.L. Ultrasound imaging of the lateral abdominal wall muscles in individuals with lumbopelvic pain and signs of concurrent hypocapnia. Man. Ther. 2008, 13, 404–410. [Google Scholar] [CrossRef] [PubMed]
- van Dixhoorn, J.; Duivenvoorden, H.J. Efficacy of Nijmegen Questionnaire in recognition of the hyperventilation syndrome. J. Psychosom. Res. 1985, 29, 199–206. [Google Scholar] [CrossRef]
- Holt, G.R. Declaration of Helsinki-The World’s Document of Conscience and Responsibility. South. Med. J. 2014, 107, 407. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.A.; Stanton, W.R.; Mendis, M.D.; Franettovich Smith, M.M.; Sexton, M.J. Small Multifidus Muscle Size Predicts Football Injuries. Orthop. J. Sport. Med. 2014, 2, 232596711453758. [Google Scholar] [CrossRef] [PubMed]
- Leung, F.T.; Mendis, M.D.; Stanton, W.R.; Hides, J.A. The relationship between the piriformis muscle, low back pain, lower limb injuries and motor control training among elite football players. J. Sci. Med. Sport 2015, 18, 407–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, P.; Pascoal, A.G.; Sancho, F.; Carita, A.I.; Bø, K. Reliability of the inter-rectus distance measured by palpation. Comparison of palpation and ultrasound measurements. Man. Ther. 2013, 18, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Bunce, S.M.; Hough, A.D.; Moore, A.P. Measurement of abdominal muscle thickness using M-mode ultrasound imaging during functional activities. Man. Ther. 2004, 9, 41–44. [Google Scholar] [CrossRef]
- Ferreira, P.H.; Ferreira, M.L.; Hodges, P.W. Changes in recruitment of the abdominal muscles in people with low back pain: Ultrasound measurement of muscle activity. Spine 2004, 29, 2560–2566. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Lobo, C.; Diez-Vega, I.; Martínez-Pascual, B.; Fernández-Martínez, S.; de la Cueva-Reguera, M.; Garrosa-Martín, G.; Rodríguez-Sanz, D. Tensiomyography, sonoelastography, and mechanosensitivity differences between active, latent, and control low back myofascial trigger points. Medicine 2017, 96, e6287. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Data | Amateur (n = 16) | Elite (n = 16) | p-Value |
|---|---|---|---|
| Age, y | 23.0 ± 7.0 † | 21.5 ± 8.75 † | 0.590 ‡ |
| Weight, kg | 79.98 ± 8.97 * | 93.56 ± 15.24 * | 0.004 ** |
| Height, m | 1.83 ± 0.07 * | 1.94 ± 0.10 * | 0.002 ** |
| BMI, kg/m2 | 21.89 ± 2.03 * | 23.83 ± 2.88 * | 0.036 ** |
| Nijmegen test * | 2.0 ± 2.76 † | 12.43 ± 3.24 * | <0.001 ‡ |
| Measurement | Amateur (n = 16) * | Elite (n = 16) * | p-Value |
|---|---|---|---|
| Distance (cm) | |||
| IRD | 1.03 ± 0.41 (0.58–1.96) * | 1.50 ± 1.01 (0.90–3.64) † | 0.001 ‡ |
| Thickness (cm) | |||
| Right RA | 1.44 ± 0.30 (0.93–2.02 * | 1.57 ± 0.33 (1.10–2.26) * | 0.260 ** |
| Right EO | 1.44 ± 0.30 (0.93–2.02 * | 0.50 ± 0.13 (0.34–0.89) * | 0.026 ** |
| Right IO | 1.10 ± 0.20 (0.82–1.57 * | 1.04 ± 0.27 (0.36–1.38) * | 0.484 ** |
| Right TrAb | 0.38 ± 0.10 (0.26–0.65) † | 0.42 ± 0.19 (0.29–1.15) † | 0.149 ‡ |
| Left RA | 1.41 ± 0.27 (1.02–1.84) * | 1.54 ± 0.36 (1.06–2.37) * | 0.247 ** |
| Left EO | 0.70 ± 0.16 (0.48–0.94) * | 0.51 ± 0.14 (0.30–0.89) * | 0.002 ** |
| Left IO | 1.13 ± 0.20 (0.87–1.47) * | 1.08 ± 0.22 (0.70–1.41) * | 0.487 ** |
| Left TrAb | 0.40 ± 0.07 (0.29–0.54) * | 0.47 ± 0.09 (0.31–0.65) * | 0.034 ** |
| Parameter | Model | R2 Change † | Model R2 |
|---|---|---|---|
| IRD (cm) | 0.841 +0.068 * Nijmegen test | 0.322 | 0.322 |
| Right EO (cm) | 0.748 −0.019 * Nijmegen test | 0.196 | 0.196 |
| Left TrAb (cm) | 0.773 +0.025 * BMI −0.005 * height +0.007 * Nijmegen test | 0.219 0.106 0.157 | 0.482 |
| Left EO (cm) | −0.573 +0.258 * group +0.035 * BMI | 0.286 0.220 | 0.507 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Morales, C.; Almazán-Polo, J.; Rodríguez-Sanz, D.; Palomo-López, P.; López-López, D.; Vázquez-González, S.; Calvo-Lobo, C. Rehabilitative Ultrasound Imaging Features of the Abdominal Wall Muscles in Elite and Amateur Basketball Players. Appl. Sci. 2018, 8, 809. https://doi.org/10.3390/app8050809
Romero-Morales C, Almazán-Polo J, Rodríguez-Sanz D, Palomo-López P, López-López D, Vázquez-González S, Calvo-Lobo C. Rehabilitative Ultrasound Imaging Features of the Abdominal Wall Muscles in Elite and Amateur Basketball Players. Applied Sciences. 2018; 8(5):809. https://doi.org/10.3390/app8050809
Chicago/Turabian StyleRomero-Morales, Carlos, Jaime Almazán-Polo, David Rodríguez-Sanz, Patricia Palomo-López, Daniel López-López, Sergio Vázquez-González, and César Calvo-Lobo. 2018. "Rehabilitative Ultrasound Imaging Features of the Abdominal Wall Muscles in Elite and Amateur Basketball Players" Applied Sciences 8, no. 5: 809. https://doi.org/10.3390/app8050809