The Contribution of Geogenic Particulate Matter to Lung Disease in Indigenous Children

 , , ,
, , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Studies
2.1.1. Data Sources
2.1.2. Ethics
2.1.3. Data Linkage
2.1.4. Study Sample
2.1.5. Dust Levels
2.1.6. Health Outcomes
2.2. In Vitro Studies
2.2.1. Community Sampled Dust
2.2.2. Cell Culture and Bacteria
2.2.3. Cell and Bacterial Interactions in Response to PM
2.2.4. Statistical Analysis
3. Results
3.1. Epidemiological Studies
3.1.1. Carer-Reported Health Outcomes
3.1.2. Hospitalisation
3.2. In Vitro Studies
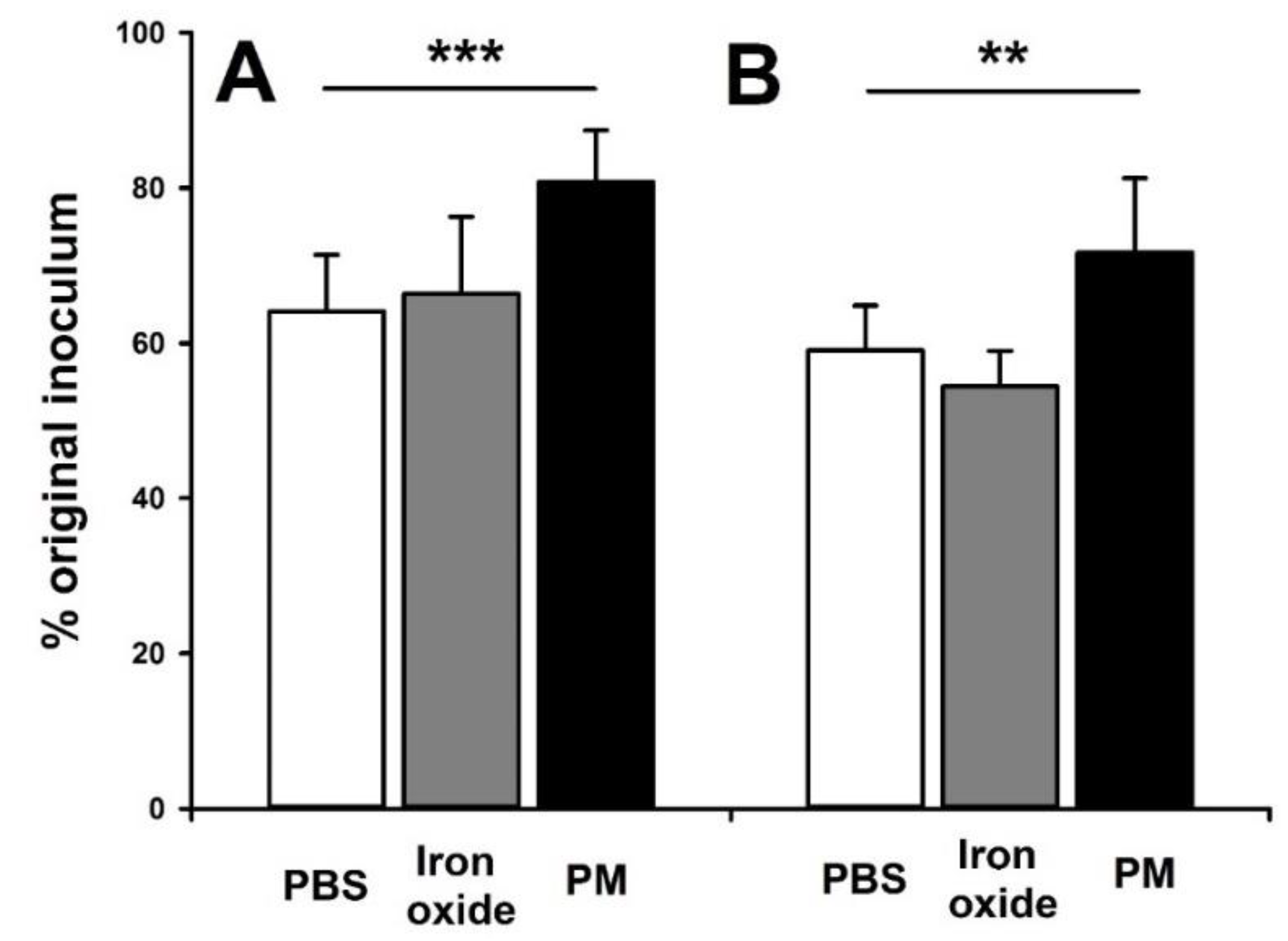
NTHi Adhesion and Invasion
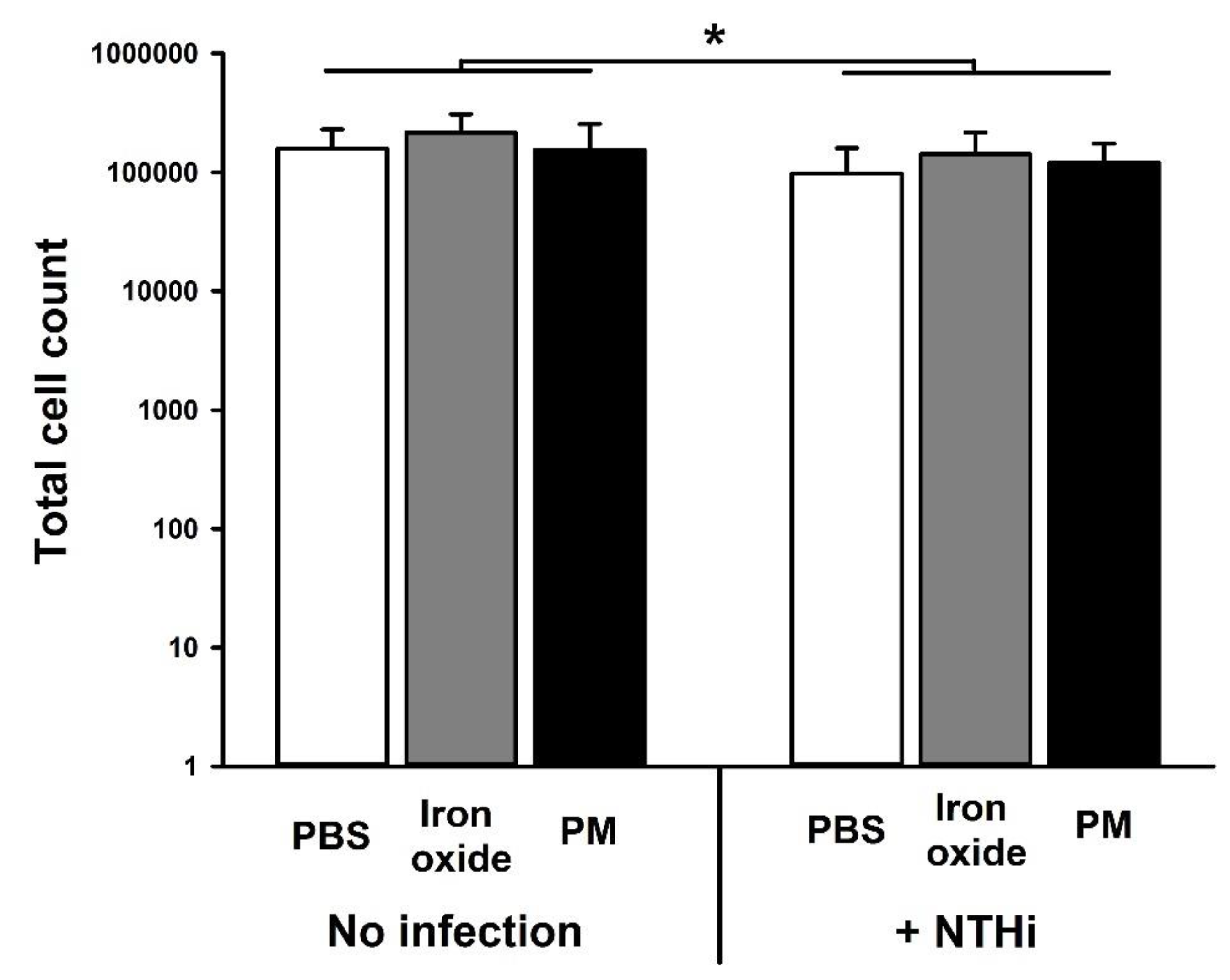
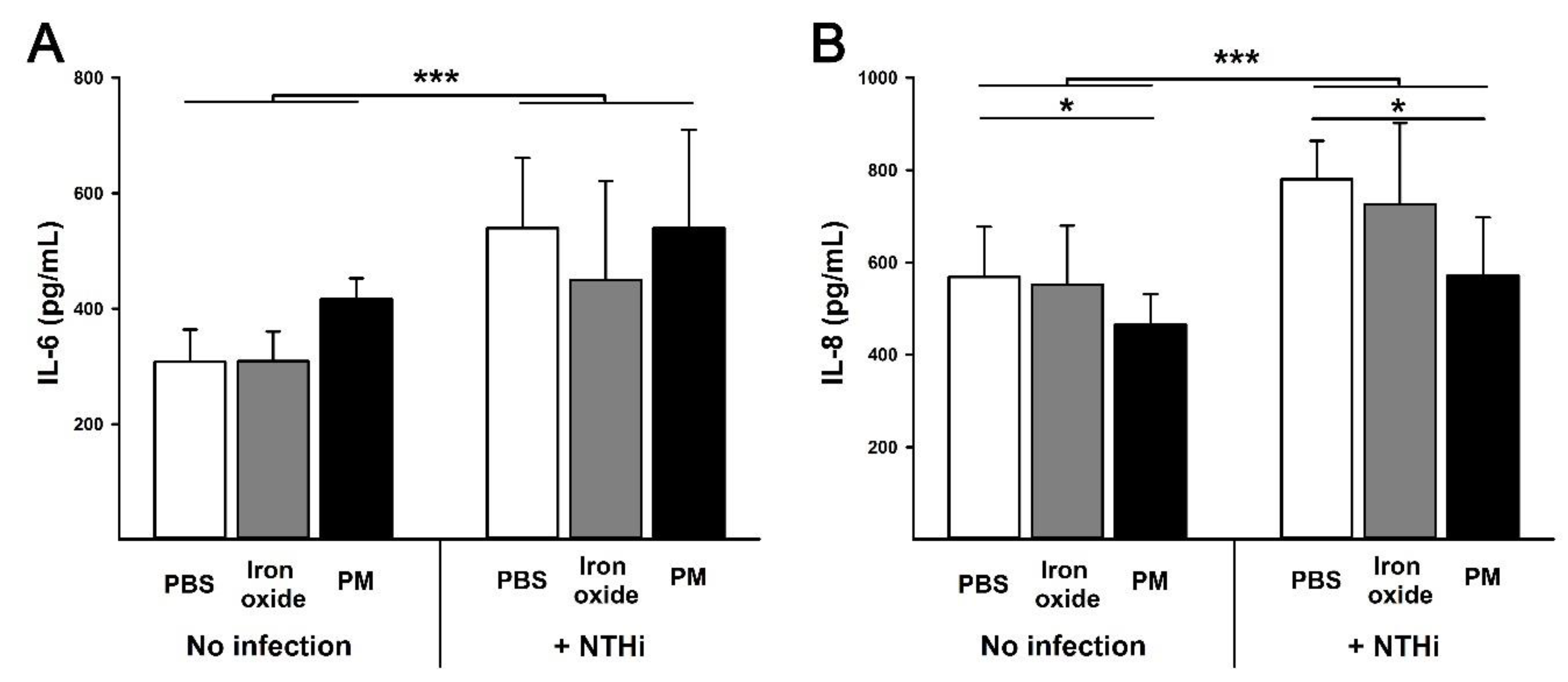
3.3. Cell Viability and Cytokine Production
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- King, M.; Smith, A.; Gracey, M. Indigenous health part 2: The underlying causes of the health gap. Lancet 2009, 374, 76–85. [Google Scholar] [CrossRef]
- Shepherd, C.C.J.; Li, J.; Zubrick, S.R. Social Gradients in the Health of Indigenous Australians. Am. J. Public Health 2012, 102, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Rowley, K.G.; O’Dea, K.; Anderson, I.; McDermott, R.; Saraswati, K.; Tilmouth, R.; Roberts, I.; Fitz, J.; Wang, Z.; Jenkins, A.; et al. Lower than expected morbidity and mortality for an Australian Aboriginal population: 10-year follow-up in a decentralised community. Med. J. Aust. 2008, 188, 238–287. [Google Scholar]
- Morrissey, M.J. Poverty and Indigenous health. Health Sociol. Rev. 2003, 12, 17–30. [Google Scholar] [CrossRef]
- McDonald, E.L. Closing the Gap and Indigenous housing. Med. J. Aust. 2011, 195, 652–653. [Google Scholar] [CrossRef]
- Cullinane, J.; Gracey, M. Gastroenteritis and environmental health among Aboriginal infants and children in Western Australia. J. Paediatr. Child. Health 2003, 39, 427–431. [Google Scholar]
- Torzillo, P.J.; Chang, A.B. Acute respiratory infections among Indigenous children. Med. J. Aust. 2014, 200, 559–560. [Google Scholar] [CrossRef] [Green Version]
- Morris, P.S.; Leach, A.J.; Silberberg, P.; Mellon, G.; Wilson, C.; Hamilton, E.; Beissbarth, J. Otitis media in young Aboriginal children from remote communities in Northern and Central Australia: A cross-sectional survey. BMC Pediatr. 2005, 5, 27. [Google Scholar] [CrossRef]
- O’Grady, K.A.F.; Torzillo, P.J.; Chang, A.B. Hospitalisation of Indigenous children in the Northern Territory for lower respiratory illness in the first year of life. Med. J. Aust. 2010, 192, 586–590. [Google Scholar]
- Clifford, H.D.; Pearson, G.; Franklin, P.; Walker, R.; Zosky, G.R. Environmental health challenges in remote Aboriginal Australian communities: Clean air, clean water and safe housing. Aust. Indig. Health Bull. 2015, 15, 2. [Google Scholar]
- O’Grady, K.A.F.; Taylor-Thomson, D.M.; Chang, A.B.; Torzillo, P.J.; Morris, P.S.; Mackenzie, A.G.; Wheaton, G.R.; Bauert, A.P.; De Campo, M.P.; De Campo, J.F.; et al. Rates of radiologically confirmed pneumonia as defined by the World Health Organization in Northern Territory Indigenous children. Med. J. Aust. 2010, 192, 592–595. [Google Scholar] [PubMed]
- Chien, L.C.; Yang, C.H.; Yu, H.L. Estimated effects of Asian dust storms on spatiotemproal distributions of clinic visits for respiratory disease in Taipei children. Environ. Health Perspect. 2012, 120, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Zosky, G.R.; Boylen, C.E.; Wong, R.S.; Smirk, M.N.; Gutierrez, L.; Woodward, R.C.; Shan Siah, W.; Devine, B.; Maley, F.; Cook, A. Variability and consistency in lung inflammatory responses to particles with a geogenic origin. Respirology 2014, 19, 58–66. [Google Scholar] [CrossRef] [PubMed]
- South Australian Department of Health. Whyalla Health Impact Study Report; Government of South Australia: Adelaide, Australia, 2007. [Google Scholar]
- Western Australian Department of Health. Impact of Dust on Port Hedland; Government of Western Australia: Perth, Australia, 2010. [Google Scholar]
- Zosky, G.R.; Iosifidis, T.; Perks, K.; Ditcham, W.G.F.; Devadason, S.G.; Siah, W.S.; Devine, B.; Maley, F.; Cook, A. The Concentration of Iron in Real-World Geogenic PM10 Is Associated with Increased Inflammation and Deficits in Lung Function in Mice. PLoS ONE 2014, 9, e90609. [Google Scholar] [CrossRef]
- Clifford, H.D.; Perks, K.L.; Zosky, G.R. Geogenic PM10 exposure exacerbates responses to influenza infection. Sci. Total Environ. 2015, 533, 275–282. [Google Scholar] [CrossRef]
- Melody, S.M.; Bennett, E.; Clifford, H.D.; Johnston, F.H.; Shepherd, C.C.; Alach, Z.; Lester, M.; Wood, L.J.; Franklin, P.; Zosky, G.R.; et al. A cross-sectional survey of environmental health in remote Aboriginal communities in Western Australia. Int. J. Environ. Health Res. 2016, 26, 1–11. [Google Scholar] [CrossRef]
- Hare, K.M.; Grimwood, K.; Leach, A.J.; Smith-Vaughan, H.; Torzillo, P.J.; Morris, P.S.; Chang, A.B. Respiratory Bacterial Pathogens in the Nasopharynx and Lower Airways of Australian Indigenous Children with Bronchiectasis. J. Pediatr. 2010, 157, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Jacoby, P.; Riley, T.V.; Bowman, J.; Leach, A.J.; Coates, H.; Weeks, S.; Cripps, A.; Lehmann, D. Association between early bacterial carriage and otitis media in Aboriginal and non-Aboriginal children in a semi-arid area of Western Australia: A cohort study. BMC Infect. Dis. 2012, 12, 366. [Google Scholar] [CrossRef]
- Silburn, S.R.; Zubrick, S.R.; De Maio, J.A.; Shepherd, C.; Griffin, J.A.; Mitrou, F.G.; Dalby, R.B.; Hayward, C.; Pearson, G. The Western Australian Aboriginal Child Health Survey: Strengthening the Capacity of Aboriginal Children, Families and Communities; Telethon Kids Institute: Perth, Australia, 2006. [Google Scholar]
- Holman, C.D.; Bass, A.J.; Rosman, D.L.; Smith, M.B.; Semmens, J.B.; Glasson, E.J.; Brook, E.L.; Trutwein, B.; Rouse, I.L.; Watson, C.R.; et al. A decade of data linkage in Western Australia: Strategic design, applications and benefits of the W.A. data linkage system. Aust. Health Rev. 2008, 32, 766–777. [Google Scholar] [CrossRef]
- Pickering, J.L.; Prosser, A.; Corscadden, K.J.; de Gier, C.; Richmond, P.C.; Zhang, G.; Thornton, R.B.; Kirkham, L.-A.S. Haemophilus haemolyticus interaction with host cells is different to nontypeable Haemophilus influenzae and prevents NTHi association with epithelial cells. Front. Cell. Infect. Microbiol. 2016, 6, 50. [Google Scholar] [CrossRef]
- Pfeffermann, D.; Skinner, C.J.; Holmes, D.J.; Goldstein, H.; Rasbash, J. Weighting for unequal selection probabilities in multilevel models. J. R. Stat. Soc. Ser. B Stat. Methodol. 1998, 60, 23–40. [Google Scholar] [CrossRef]
- Jones, H.L. Jackknife Estimation of Functions of Stratum Means. Biometrika 1974, 61, 343. [Google Scholar] [CrossRef]
- Ikeda, M.; Enomoto, N.; Hashimoto, D.; Fujisawa, T.; Inui, N.; Nakamura, Y.; Suda, T.; Nagata, T. Nontypeable Haemophilus influenzar exploits the interaction between protein-E and vitronectin for the adherence and invasion to bronchial epithelial cells. BMC Microbiol. 2015, 15, 263. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, S.W.; Kuehn, M.J.; Mason, K.M. Elicitation of epithelial cell-derived immune effectors by outer membarne vesicles of nontypeable Haemophilus influenzae. Infect. Immun. 2011, 79, 4361–4369. [Google Scholar] [CrossRef] [PubMed]
- Unger, B.L.; Faris, A.N.; Ganesan, S.; Comstock, A.T.; Hershenson, M.B.; Sajjan, U.S. Rhinovirus attenuates non-typeable Haemophilus influenzae-stimulated IL-8 response via TLR2-dependent degradation of IRAK-1. PLoS Pathog. 2012, 8, e1002969. [Google Scholar] [CrossRef] [PubMed]
- Foxwell, A.R.; Kyd, J.M.; Cripps, A.W. Characteristics of the immunological response in the clearance of non-typeable Haemophilus influenzae from the lung. Immunol. Cell Biol. 1998, 76, 323–331. [Google Scholar] [CrossRef]
- Williams, L.J.; Zosky, G.R. The inflammatory effect of irono oxide and silica particles on lung epithelial cells. Lung 2019, 197, 199–207. [Google Scholar] [CrossRef]
- Ormstad, H.; Johansen, B.V.; Gaarder, P.I. Airborne house dust particles and diesel exhaust particles as allergen carriers. Clin. Exp. Allergy 1998, 28, 702–708. [Google Scholar] [CrossRef]
- Steering Committee for the Review of Government Service Provision. Overcoming Indigenous Disadvantage: Key Indicators 2016; Productivity Commission: Canberra, Australia, 2016. [Google Scholar]
- Kouis, P.; Kakkoura, M.; Ziogas, K.; Paschalidou, A.Κ.; Papatheodorou, S.I. The effect of ambient air temperature on cardiovascular and respiratory mortality in Thessaloniki, Greece. Sci. Total Environ. 2019, 647, 1351–1358. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Dust Level | OR | 95% CI | p-value c |
|---|---|---|---|
| Asthma | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 0.68 | 0.29–1.59 | 0.375 |
| High/Excessive | 1.40 | 0.63–3.12 | 0.411 |
| Any respiratory conditionb | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 0.89 | 0.49–1.64 | 0.719 |
| High/Excessive | 1.37 | 0.87–2.17 | 0.178 |
| Recurring chest infections | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 0.60 | 0.19–1.86 | 0.372 |
| High/Excessive | 1.05 | 0.43–2.53 | 0.920 |
| Ear infections | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 0.73 | 0.41–1·28 | 0.269 |
| High/Excessive | 0.60 | 0.36–1·01 | 0.054 |
| Recurring skin conditions | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 1.00 | 0.43–2.32 | 0.995 |
| High/Excessive | 1.37 | 0.58–3.24 | 0.477 |
| Allergies and hay fever | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 1.08 | 0.46–2.52 | 0.865 |
| High/Excessive | 2.24 | 1.09–4.60 | 0.030 |
| Recurring gastrointestinal infections | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 1.44 | 0.47–4.40 | 0.520 |
| High/Excessive | 1.11 | 0.48–2.56 | 0.814 |
| Dust Level | OR | 95% CI | p-value d |
|---|---|---|---|
| Any respiratory conditionb | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 2.90 | 1.42–5.93 | 0.004 |
| High/Excessive | 2·56 | 1.34–4.91 | 0.005 |
| Selected ear diseasesc | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 3.06 | 1.20–7.80 | 0.020 |
| High/Excessive | 1.90 | 0.88–4.13 | 0.105 |
| Selected eye diseasese | |||
| Low/None | 1.00 | ||
| Moderate | 1.37 | 0.43–4.36 | 0.598 |
| High/Excessive | 1.20 | 0.42–3.41 | 0.734 |
| Selected skin conditionsf | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 1.13 | 0.63–2.02 | 0.673 |
| High/Excessive | 0.99 | 0.61–1.62 | 0.976 |
| Selected gastrointestinal diseasesg | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 0.79 | 0.42–1.50 | 0.476 |
| High/Excessive | 1.01 | 0.61–1.66 | 0.971 |
| Upper respiratory tract infectionsh | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 1.73 | 0.77–3.91 | 0.188 |
| High/Excessive | 1.77 | 1.02–3.06 | 0.043 |
| Acute lower respiratory tract infectioni | |||
| Low/None | 1.00 | .. | .. |
| Moderate | 2.04 | 1.15–3.63 | 0.016 |
| High/Excessive | 1.99 | 1.08–3.68 | 0.028 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shepherd, C.C.J.; Clifford, H.D.; Mitrou, F.; Melody, S.M.; Bennett, E.J.; Johnston, F.H.; Knibbs, L.D.; Pereira, G.; Pickering, J.L.; Teo, T.H.; et al. The Contribution of Geogenic Particulate Matter to Lung Disease in Indigenous Children. Int. J. Environ. Res. Public Health 2019, 16, 2636. https://doi.org/10.3390/ijerph16152636
Shepherd CCJ, Clifford HD, Mitrou F, Melody SM, Bennett EJ, Johnston FH, Knibbs LD, Pereira G, Pickering JL, Teo TH, et al. The Contribution of Geogenic Particulate Matter to Lung Disease in Indigenous Children. International Journal of Environmental Research and Public Health. 2019; 16(15):2636. https://doi.org/10.3390/ijerph16152636
Chicago/Turabian StyleShepherd, Carrington C. J., Holly D. Clifford, Francis Mitrou, Shannon M. Melody, Ellen J. Bennett, Fay H. Johnston, Luke D. Knibbs, Gavin Pereira, Janessa L. Pickering, Teck H. Teo, and et al. 2019. "The Contribution of Geogenic Particulate Matter to Lung Disease in Indigenous Children" International Journal of Environmental Research and Public Health 16, no. 15: 2636. https://doi.org/10.3390/ijerph16152636