
In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering—Introducing a New Biocompatibility Scoring System

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Production of Composite Scaffolds
2.2. Polyurethane Scaffolds
2.3. Macroscopic Assessment of Scaffold Pore Structure
2.4. Interconnectivity of Scaffold Pores
2.5. Isolation and Culture of Human Mesenchymal Stem Cells
2.6. In Vitro Chondrogenesis
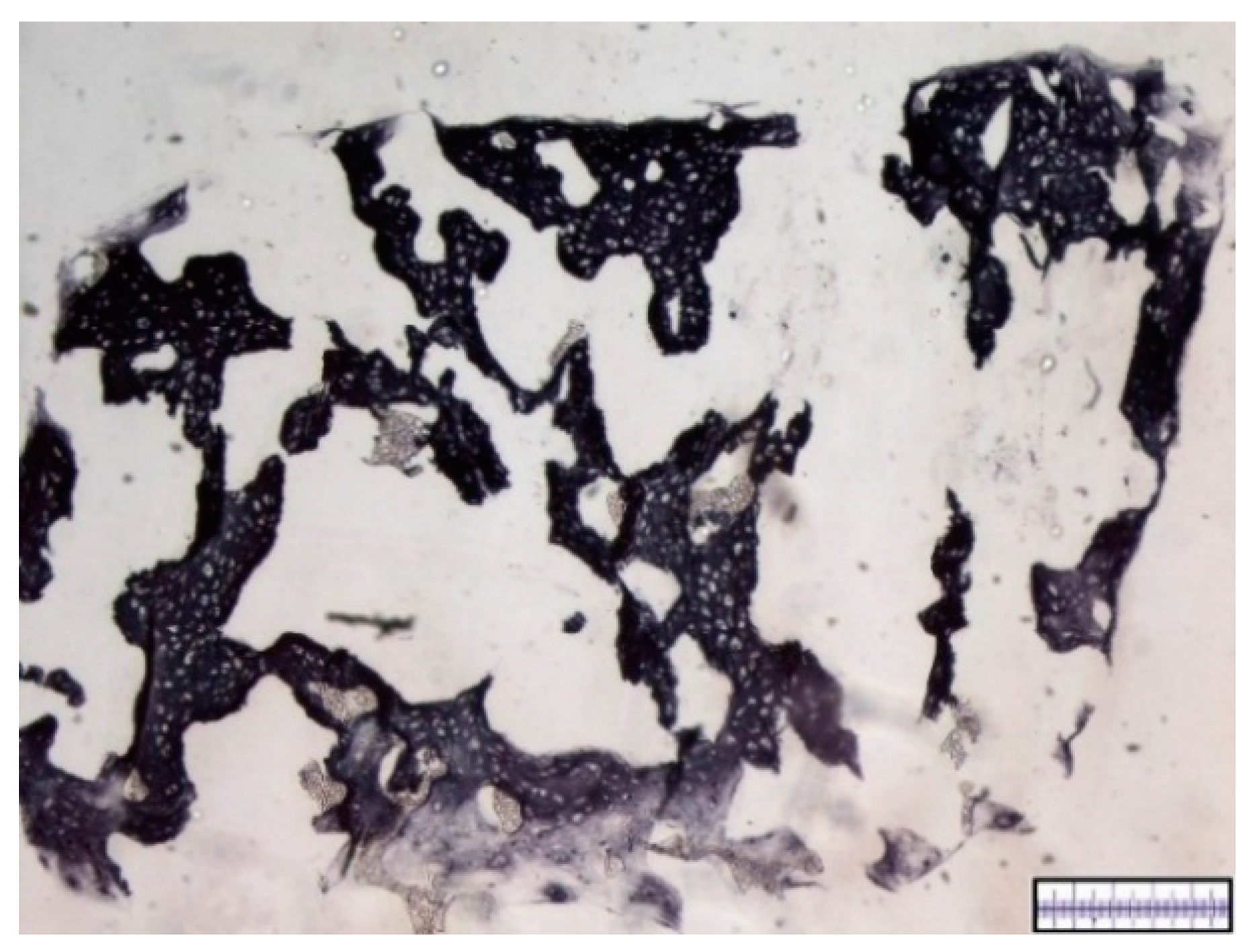
2.7. Histology
2.8. Immunohistochemistry
2.9. Score
2.10. Statistical Analysis
3. Results
3.1. Macroscopical Assessment of Scaffold Pore Structure
3.2. Interconnectivity of Scaffold Pores
3.3. In Vitro Chondrogenesis
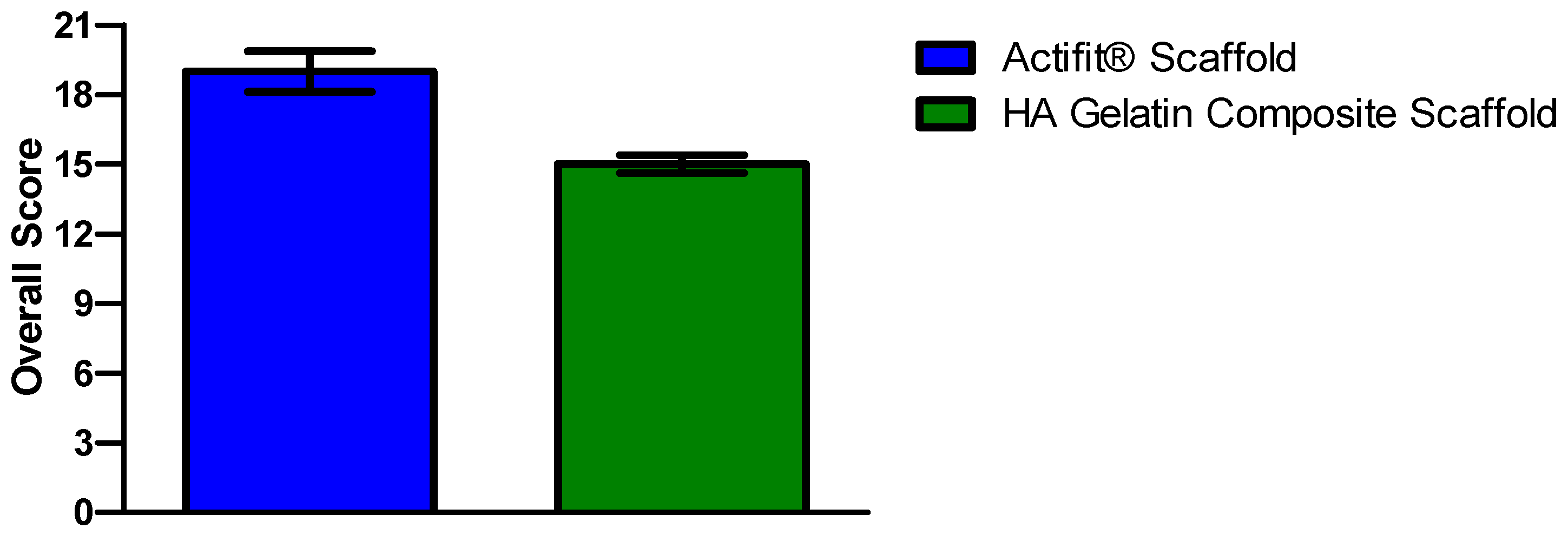
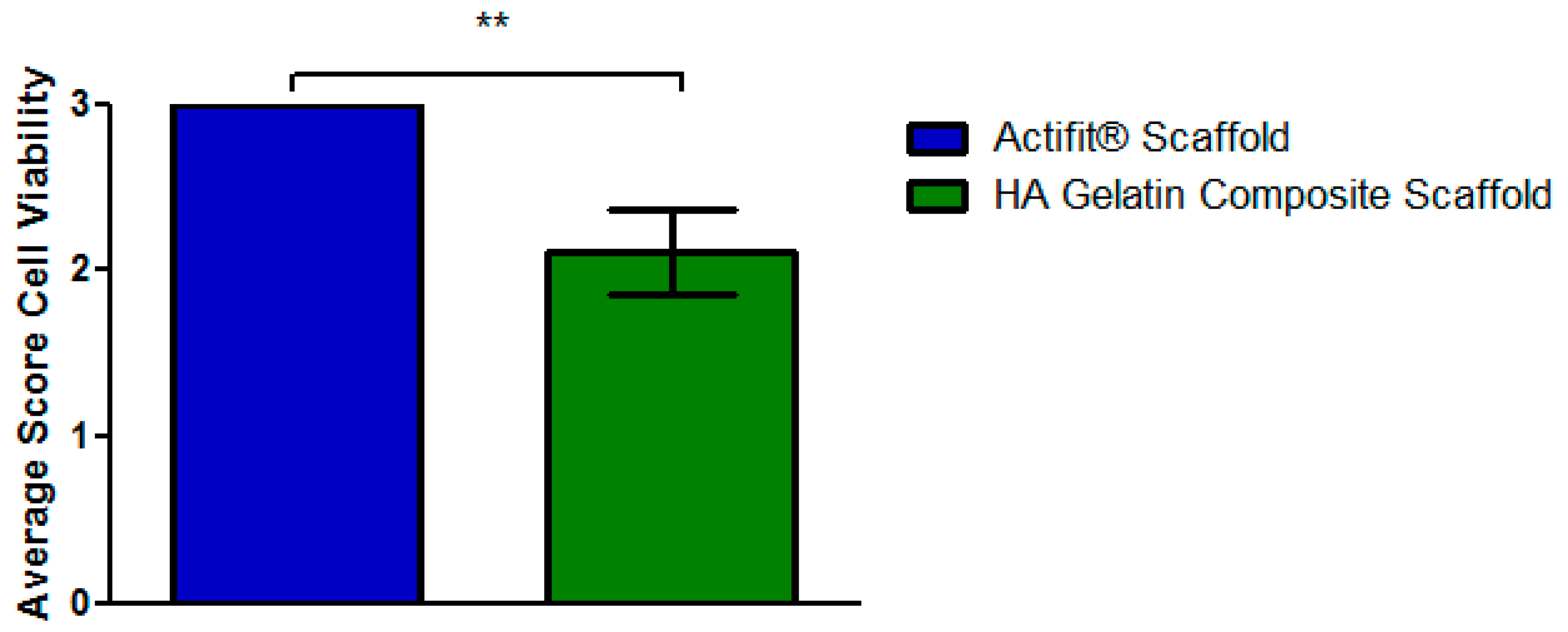
3.4. Scoring
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BSA | bovine albumin solution |
| DMMB | dimethylemethylene blue |
| MSCs | mesenchymal stem cells |
| HA | hyaluronic acid |
| TGF-beta | transforming growth factor beta |
References
- Verdonk, P.; Beaufils, P.; Bellemans, J.; Djian, P.; Heinrichs, E.-L.; Huysse, W.; Laprell, H.; Siebold, R.; Verdonk, R.; Colombet, P.; et al. Successful Treatment of Painful Irreparable Partial Meniscal Defects with a Polyurethane Scaffold: Two-Year Safety and Clinical Outcomes. Am. J. Sports Med. 2012, 40, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Brindle, T.; Nyland, J.; Johnson, D.L. The meniscus: Review of basic principles with application to surgery and rehabilitation. J. Athl. Train 2001, 36, 160–169. [Google Scholar] [PubMed]
- Petty, C.A.; Lubowitz, J.H. Does arthroscopic partial meniscectomy result in knee osteoarthritis? A systematic review with a minimum of 8 years’ follow-up. Arthroscopy 2011, 27, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Toma, I.C.; Mastrogiacomo, M.; Krettek, C.; Lewinski, G.; von Jagodzinski, M. Meniscus reconstruction: Today’s achievements and premises for the future. Arch. Orthop. Trauma. Surg. 2013, 133, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.M.; Torzilli, P.A.; Gould, J.D.; Warren, R.F. The effect of lateral meniscectomy on motion of the knee. J. Bone Joint Surg. Am. 1989, 71, 401–406. [Google Scholar] [PubMed]
- Renstrom, P.; Johnson, R.J. Anatomy and biomechanics of the menisci. Clin. Sports Med. 1990, 9, 523–538. [Google Scholar] [PubMed]
- Akgun, U.; Kocaoglu, B.; Orhan, E.K.; Baslo, M.B.; Karahan, M. Possible reflex pathway between medial meniscus and semimembranosus muscle: An experimental study in rabbits. Knee Surg. Sports Traumatol. Arthr. 2008, 16, 809–814. [Google Scholar] [CrossRef] [PubMed]
- McDermott, I.D.; Amis, A.A. The consequences of Meniscectomy. Bone Joint Surg. Br. 2006, 88, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, H.; Fukubayashi, T.; Nakajima, H. Load-bearing mode of the knee joint: Physical behavior of the knee joint with or without menisci. Clin. Orthop. Relat. Res. 1980, 149, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M.; Burke, D.L. In-vitro measurement of static pressure distribution in synovial joints—Part I: Tibial surface of the knee. J. Biomech. Eng. 1983, 105, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Vrancken, A.C.T.; Buma, P.; Tienen, T.G. Synthetic meniscus replacement: A review. Int. Orthop. 2013, 37, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Shirakura, K.; Hasegawa, A.; Kobuna, Y.; Niijima, M. Second look arthroscopy after meniscal repair: Factors affecting the healing rate. Clin. Orthop. Relat. Res. 1995, 314, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Rodkey, W.G.; de Haven, K.E.; Montgomery, W.H.; Baker, C.L.; Hormel, S.E.; Steadman, J.R.; Cole, B.J.; Briggs, K.K. Comparison of the collagen meniscus implant with partial meniscectomy: A prospective randomized trial. J. Bone Joint Surg. Am. 2008, 90, 1413–1426. [Google Scholar] [CrossRef] [PubMed]
- Abrams, G.D.; Frank, R.M.; Gupta, A.K.; Harris, J.D.; McCormick, F.M.; Cole, B.J. Trends in Meniscus Repair and Meniscectomy in the United States, 2005–2011. Am. J. Sports Med. 2013, 41, 2333–2339. [Google Scholar] [CrossRef] [PubMed]
- Efe, T.; Getgood, A.; Schofer, M.D.; Fuchs-Winkelmann, S.; Mann, D.; Paletta, J.R.J.; Heyse, T.J. The safety and short-term efficacy of a novel polyurethane meniscal scaffold for the treatment of segmental medial meniscus deficiency. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1822–1830. [Google Scholar] [CrossRef] [PubMed]
- Angele, P.; Kujat, R.; Koch, M.; Zellner, J. Role of mesenchymal stem cells in meniscal repair. J. Exp. Ortop. 2014, 1. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I.; Dennis, J.E. Mesenchymal stem cells as trophic mediators. J. Cell. Biochem. 2006, 98, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Zellner, J.; Hierl, K.; Mueller, M.; Pfeifer, C.; Berner, A.; Dienstknecht, T.; Krutsch, W.; Geis, S.; Gehmert, S.; Kujat, R.; et al. Stem cell-based tissue-engineering for treatment of meniscal tears in the avascular zone. J. Biomed. Mater. Res 2013, 101, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Zellner, J.; Mueller, M.; Berner, A.; Dienstknecht, T.; Kujat, R.; Nerlich, M.; Hennemann, B.; Koller, M.; Prantl, L.; Angele, M.; et al. Role of mesenchymal stem cells in tissue engineering of meniscus. J. Biomed. Mater. Res. 2010, 94, 1150–1161. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, B.; Perdisa, F.; Gostynska, N.; Kon, E.; Filardo, G.; Marcacci, M. Meniscal Scaffolds-Preclinical Evidence to Support their Use: A Systematic Review. Open Orthop. J. 2015, 9, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Zellner, J. Tissue Engineering mit mesenchymalen Stammzellen und Hyaluronsäure-Gelatine Kompositmatrices zur Reparatur avaskulärer Meniskusläsionen. Ph.D. Thesis, University Regensburg, Regensburg, Germany, 2006. [Google Scholar]
- Angele, P.; Kujat, R.; Nerlich, M.; Yoo, J.; Goldberg, V.; Johnstone, B. Engineering of osteochondral tissue with bone marrow mesenchymal progenitor cells in a derivatized hyaluronan-gelatin composite sponge. Tissue Eng. 1999, 5, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Angele, P.; Johnstone, B.; Kujat, R.; Zellner, J.; Nerlich, M.; Goldberg, V.; Yoo, J. Stem cell based tissue engineering for meniscus repair. J. Biomed. Mater. Res. 2008, 85, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Welsing, R.T.C.; van Tienen, T.G.; Ramrattan, N.; Heijkants, R.; Schouten, A.J.; Veth, R.P.H.; Buma, P. Effect on tissue differentiation and articular cartilage degradation of a polymer meniscus implant: A 2-year follow-up study in dogs. Am. J. Sports Med. 2008, 36, 1978–1989. [Google Scholar] [CrossRef] [PubMed]
- Bouyarmane, H.; Beaufils, P.; Pujol, N.; Bellemans, J.; Roberts, S.; Spalding, T.; Zaffagnini, S.; Marcacci, M.; Verdonk, P.; Womack, M.; et al. Polyurethane scaffold in lateral meniscus segmental defects: Clinical outcomes at 24 months follow-up. Orthop. Traumatol. Surg. Res. 2014, 100, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Maher, S.A.; Rodeo, S.A.; Potter, H.G.; Bonassar, L.J.; Wright, T.M.; Warren, R.F. A pre-clinical test platform for the functional evaluation of scaffolds for musculoskeletal defects: The meniscus. HSS J. 2011, 7, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Verdonk, R.; Espregueira-Mendes, J.; Monllau, J.C. Meniscal Transplantation; Springer: Heidelberg, NY, USA, 2013. [Google Scholar]
- Stone, K.R.; Steadman, J.R.; Rodkey, W.G.; Li, S.T. Regeneration of meniscal cartilage with use of a collagen scaffold: Analysis of preliminary data. J. Bone Joint Surg. Am. 1997, 79, 1770–1777. [Google Scholar] [PubMed]
- Freed, L.E.; Vunjak-Novakovic, G.; Biron, R.J.; Eagles, D.B.; Lesnoy, D.C.; Barlow, S.K.; Langer, R. Biodegradable polymer scaffolds for tissue engineering. Biotechnology 1994, 12, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Matsiko, A.; Gleeson, J.P.; O'Brien, F.J. Scaffold mean pore size influences mesenchymal stem cell chondrogenic differentiation and matrix deposition. Tissue Eng. 2015, 21, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Makris, E.A.; Hadidi, P.; Athanasiou, K.A. The knee meniscus: Structure-function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials 2011, 32, 7411–7431. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Romeo, G.; Maffulli, N.; Denaro, V. Histological scoring systems for tissue-engineered, ex vivo and degenerative meniscus. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Shemesh, M.; Asher, R.; Zylberberg, E.; Guilak, F.; Linder-Ganz, E.; Elsner, J.J. Viscoelastic properties of a synthetic meniscus implant. J. Mech. Behav. Biomed. Mater. 2014, 29, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Hoben, G.M.; Athanasiou, K.A. Meniscal repair with fibrocartilage engineering. Sports Med. Arthrosc. 2006, 14, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Desroches, A.; Queinnec, S.; Flouzat, L.; Charles, H.; Poignard, A.; Allain, J.; Chevallier, N.; Rouard, H. Morbidity of graft harvesting versus bone marrow aspiration in cell regenerative therapy. Int. Orthop. 2014, 38, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Krampera, M.; Franchini, M.; Pizzolo, G.; Aprili, G. Mesenchymal stem cells: From biology to clinical use. Blood Transfus. 2007, 5, 120–129. [Google Scholar] [PubMed]
- Johnstone, B.; Hering, T.M.; Caplan, A.I.; Goldberg, V.M.; Yoo, J.U. In vitro chondrogenesis of bone marrow-derived mesenchymal progenitor cells. Exp. Cell Res. 1998, 238, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. J. Cell Physiol. 2007, 213, 341–347. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scoring Value | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Quality of pore structure | Pore size varies more than 200% compared to the average pore size | Pore size varies 100%–200% compared to the average pore size | Pore size varies 50%–100% compared to the average pore size | Pore size varies less than 50% compared to the average pore size |
| Interconnectivity of pores, percentage of interconnect pores | 0% | 1%–25% | 26%–75% | More than 75% |
| Cell distribution in scaffolds (in vitro), percentage of cell-populated pores | 0% | 1%–25% | 26%–75% | More than 75% |
| Cell viability in scaffolds (in vitro) | 0% | 1%–25% | 26%–75% | More than 75% |
| Content of Proteoglycan (in vitro) | No staining for proteoglycan | <25% | 25%–75% | >75% |
| Percentage of Collagen I compared to total amount of extracellular matrix | More than 75% | 25%–75% | <25% | No staining for collagen I |
| Percentage of Collagen II content compared to total amount of extracellular matrix | No staining for collagen II | <25% | 25%–75% | >75% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Achatz, F.P.; Kujat, R.; Pfeifer, C.G.; Koch, M.; Nerlich, M.; Angele, P.; Zellner, J. In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering—Introducing a New Biocompatibility Scoring System. Materials 2016, 9, 276. https://doi.org/10.3390/ma9040276
Achatz FP, Kujat R, Pfeifer CG, Koch M, Nerlich M, Angele P, Zellner J. In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering—Introducing a New Biocompatibility Scoring System. Materials. 2016; 9(4):276. https://doi.org/10.3390/ma9040276
Chicago/Turabian StyleAchatz, Felix P., Richard Kujat, Christian G. Pfeifer, Matthias Koch, Michael Nerlich, Peter Angele, and Johannes Zellner. 2016. "In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering—Introducing a New Biocompatibility Scoring System" Materials 9, no. 4: 276. https://doi.org/10.3390/ma9040276