Geometric Analysis of Type B Aortic Dissections Shows Aortic Remodeling After Intervention Using Multilayer Stents


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design, Patient Selection, and Follow-Up
2.3. CTA Imaging Protocol
2.4. Measurement Protocol
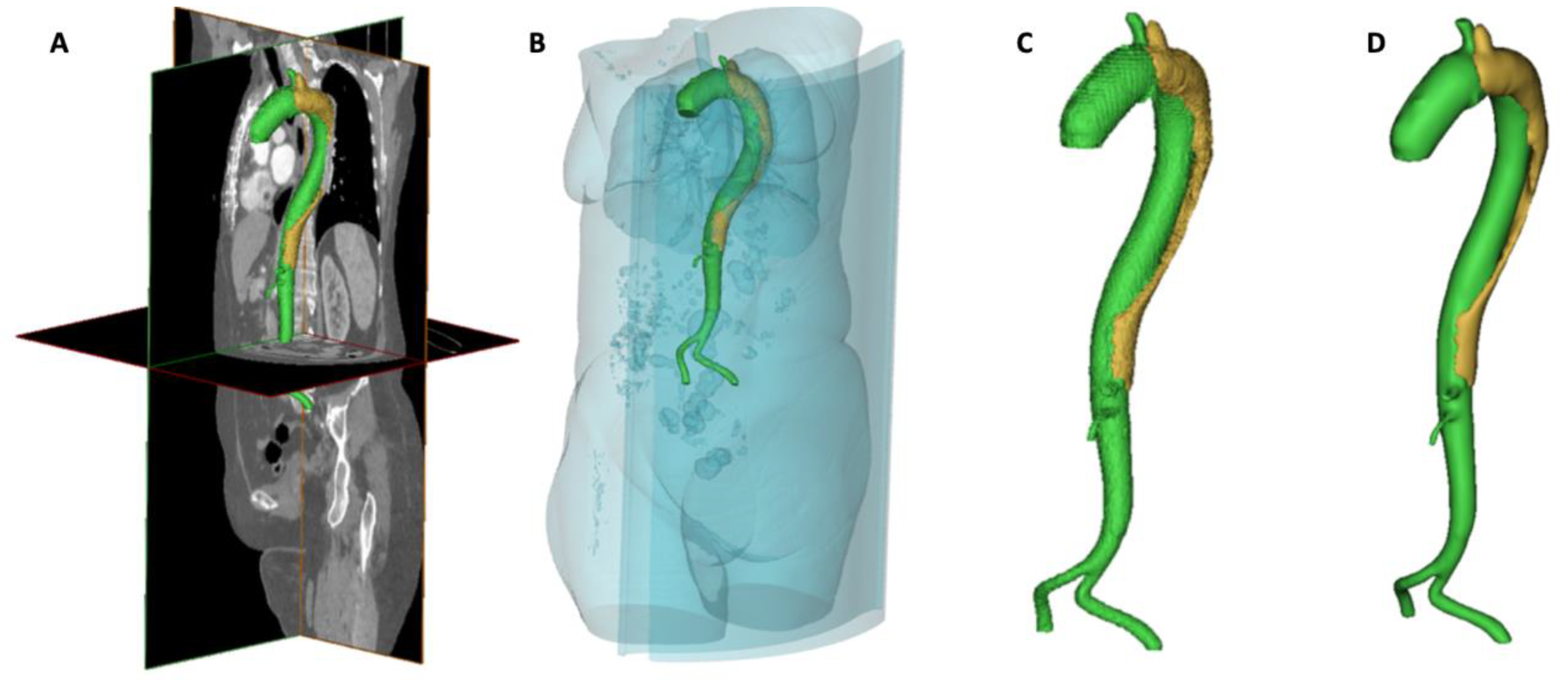
Segmentation and Geometrical Reconstruction of the Aorta
2.5. 3D Model Construction
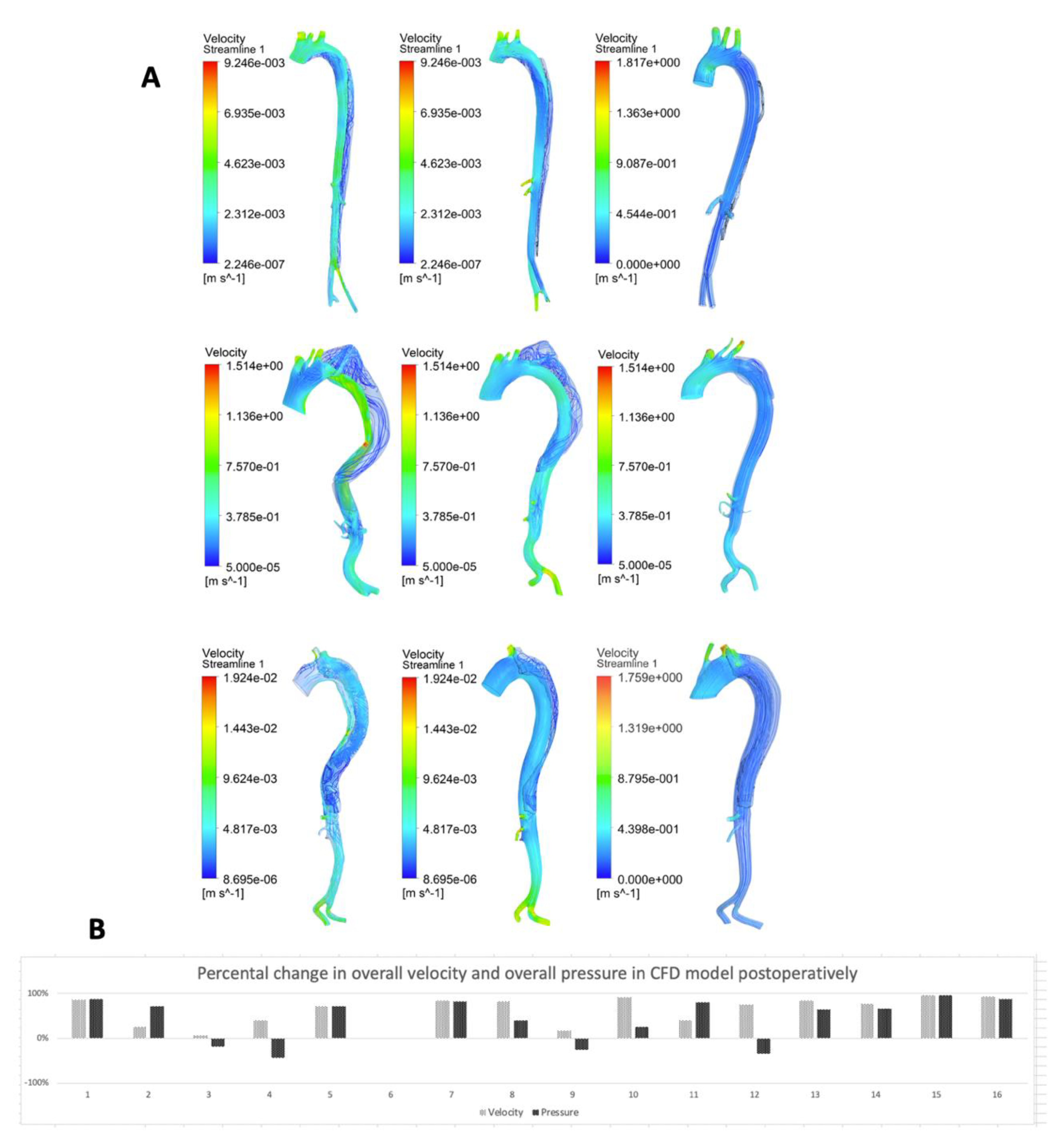
2.6. Computational Fluid Dynamics Modeling Protocol
2.7. Workstation
2.8. Statistical Analysis
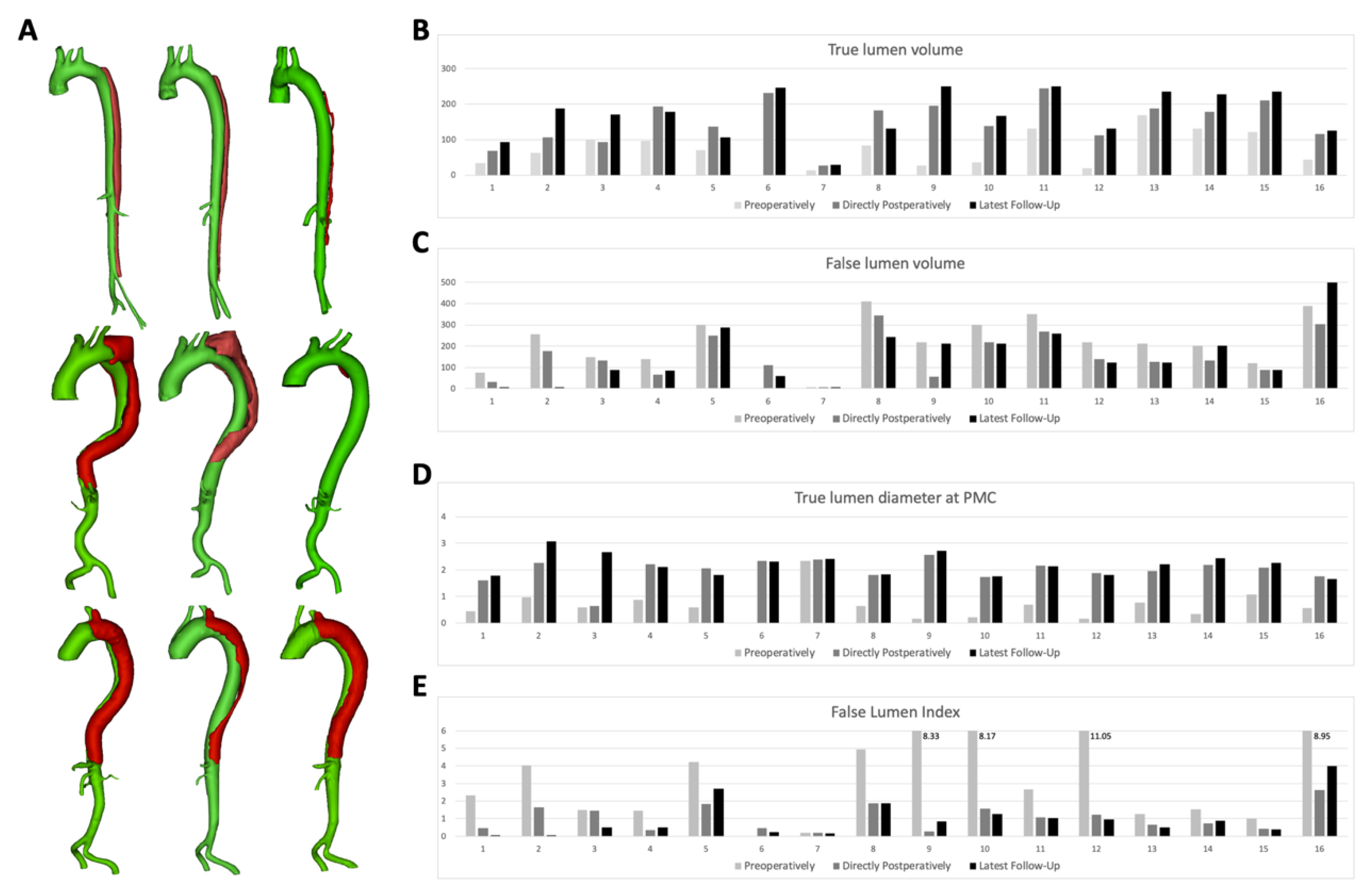
3. Results
MFM Cases Analysis
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schwartz, S.I.; Durham, C.; Clouse, W.D.; Patel, V.I.; Lancaster, R.T.; Cambria, R.; Conrad, M.F. Predictors of late aortic intervention in patients with medically treated type B aortic dissection. J. Vasc. Surg. 2018, 67, 78–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dake, M.D.; Thompson, M.; Van Sambeek, M.; Vermassen, F.; Morales, J.; DEFINE Investigators. DISSECT: A new mnemonic-based approach to the categorization of aortic dissection. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 175–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Z.; Fu, W.; Wang, Y.; Wang, C.; Yan, Z.; Guo, D.; Xu, X.; Chen, B. Stent graft-induced new entry after endovascular repair for Stanford type B aortic dissection. J. Vasc. Surg. 2010, 52, 1450–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jánosi, R.A.; Tsagakis, K.; Bettin, M.; Kahlert, P.; Horacek, M.; Al-Rashid, F.; Schlosser, T.; Jakob, H.; Eggebrecht, H.; Erbel, R. Thoracic aortic aneurysm expansion due to late distal stent graft-induced new entry. Catheter. Cardiovasc. Interv. 2015, 85, E43–E53. [Google Scholar] [CrossRef]
- Rodriguez-Lopez, J.A.; Olsen, D.M.; Lucas, L.; Wheatley, G.; Ramaiah, V.; Diethrich, E.B. Aortic remodeling after endografting of thoracoabdominal aortic dissection. J. Vasc. Surg. 2008, 47, 1188–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, M.F.; Carvalho, S.; Ergul, E.; Kwolek, C.J.; Lancaster, R.T.; Patel, V.I.; Cambria, R. Late aortic remodeling persists in the stented segment after endovascular repair of acute complicated type B aortic dissection. J. Vasc. Surg. 2015, 62, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Sayer, D.; Bratby, M.; Brooks, M.; Loftus, I.; Morgan, R.; Thompson, M. Aortic morphology following endovascular repair of acute and chronic type B aortic dissection: Implications for management. Eur. J. Vasc. Endovasc. Surg. 2008, 48, 1355. [Google Scholar] [CrossRef]
- Sobocinski, J.; Lombardi, J.V.; Dias, N.; Berger, L.; Zhou, Q.; Jia, F.; Resch, T.; Haulon, S. Volume analysis of true and false lumens in acute complicated type B aortic dissections after thoracic endovascular aortic repair with stent grafts alone or with a composite device design. J. Vasc. Surg. 2016, 63, 1216–1224. [Google Scholar] [CrossRef] [Green Version]
- Famularo, M.; Meyermann, K.; Lombardi, J.V. Aneurysmal degeneration of type B aortic dissections after thoracic endovascular aortic repair: A systematic review. J. Vasc. Surg. 2017, 66, 924–930. [Google Scholar] [CrossRef] [Green Version]
- Hynes, N.; Sultan, S.; Elhelali, A.; Diethrich, E.B.; Kavanagh, E.P.; Sultan, M.; Stefanov, F.; DeLassus, P.; Morris, L. Systematic Review and Patient-Level Meta-analysis of the Streamliner Multilayer Flow Modulator in the Management of Complex Thoracoabdominal Aortic Pathology. J. Endovasc. Ther. 2016, 23, 501–512. [Google Scholar] [CrossRef]
- Sultan, S.; Kavanagh, E.P.; Stefanov, F.; Sultan, M.; Elhelali, A.; Costache, V.; Diethrich, E.; Hynes, N.; Petrov, I.; Grozdinski, L.; et al. Endovascular management of chronic symptomatic aortic dissection with the Streamliner Multilayer Flow Modulator: Twelve-month outcomes from the global registry. J. Vasc. Surg. 2017, 65, 940–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaislic, C.D.; Fabiani, J.N.; Chocron, S.; Robin, J.; Costache, V.S.; Villemot, J.-P.; Alsac, J.-M.; Leprince, P.N.; Unterseeh, T.; Portocarrero, E.; et al. One-year outcomes following repair of thoracoabdominal aneurysms with the multilayer flow modulator: Report from the STRATO trial. J. Endovasc. Ther. 2014, 21, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Vaislic, C.D.; Fabiani, J.N.; Chocron, S.; Robin, J.; Costache, V.S.; Villemot, J.-P.; Alsac, J.M.; Leprince, P.N.; Unterseeh, T.; Portocarrero, E.; et al. Three-Year Outcomes with the Multilayer Flow Modulator for Repair of Thoracoabdominal Aneurysms: A Follow-up Report from the STRATO Trial. J. Endovasc. Ther. 2016, 23, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Schoder, M.; Czerny, M.; Cejna, M.; Rand, T.; Stadler, A.; Sodeck, G.H.; Gottardi, R.; Loewe, C.; Lammer, J. Endovascular repair of acute type B aortic dissection: Long-term follow-up of true and false lumen diameter changes. Ann. Thorac. Surg. 2007, 83, 1059–1066. [Google Scholar] [CrossRef]
- Gasparetto, A.; Park, K.B.; Sabri, S.S.; Park, A.W.; Matsumoto, A.H.; Angle, J.F. Factors Related to Late False Lumen Enlargement after Thoracic Stent-Graft Placement for Type B Aortic Dissection. J. Vasc. Interv. Radiol. 2017, 28, 44–49. [Google Scholar] [CrossRef]
- Finotello, A.; Faggiano, E.; Conti, M.; Spinella, G.; Pane, B.; Palombo, D.; Auricchio, F. Medical image analysis to measure the follow-up geometry of thoraco-abdominal aortic aneurysms treated with multilayer flow modulator stent. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2019, 8, 126–133. [Google Scholar] [CrossRef]
- Costache, V.S.; Yeung, K.K.; Solomon, C.; Popa, R.; Melnic, T.; Sandu, M.; Bucurenciu, C.; Candea, G.; Santa, A.; Costache, A. Aortic Remodeling After Total Endovascular Aortic Repair with Multilayer Stents: Computational Fluid Dynamics Analysis of Aortic Remodeling Over 3 Years of Follow-up. J. Endovasc. Ther. 2018, 25, 760–764. [Google Scholar] [CrossRef]
- Shin, E.; Kim, J.J.; Lee, S.; Ko, K.S.; Rhee, B.D.; Han, J.; Kim, N. Hemodynamics in diabetic human aorta using computational fluid dynamics. PLoS ONE 2018, 13, e0202671. [Google Scholar] [CrossRef]
- Van Bakel, T.M.; Romarowski, R.M.; Morganti, S.; Van Herwaarden, J.A.; Moll, F.L.; De Beaufort, H.W.; Marrocco-Trischitta, M.M.; Secchi, F.; Conti, M.; Auricchio, F.; et al. Blood Flow after Endovascular Repair in the Aortic Arch: A Computational Analysis. Aorta 2018, 6, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Eslami, P.; Seo, J.-H.; Lardo, A.C.; Chen, M.Y.; Mittal, R. Flow Dynamics in the Aortic Arch and Its Effect on the Arterial Input Function in Cardiac Computed Tomography. J. Biomech. Eng. 2019, 141, 104501. [Google Scholar] [CrossRef]
- Xu, H.; Piccinelli, M.; Leshnower, B.G.; Lefieux, A.; Taylor, W.R.; Veneziani, A. Coupled Morphological-Hemodynamic Computational Analysis of Type B Aortic Dissection: A Longitudinal Study. Ann. Biomed. Eng. 2018, 46, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Bonfanti, M.; Franzetti, G.; Maritati, G.; Homer-Vanniasinkam, S.; Balabani, S.; Diaz-Zuccarini, V. Patient-specific haemodynamic simulations of complex aortic dissections informed by commonly available clinical datasets. Med. Eng. Phys. 2019, 71, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Costache, V.; Ciobanu, E.; Hynes, N. Streamliner Multilayer Flow Modulator for subacute complicated type B dissection using the phantom technique. J. Vasc. Surg. 2016, 63, 1635–1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debing, E.; Aerden, D.; Gallala, S.; Vandenbroucke, F.; Brande, P.V.D. Stenting complex aorta aneurysms with the Cardiatis multilayer flow modulator: First impressions. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 604–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nezami, F.R.; Athanasiou, L.S.; Amrute, J.M.; Edelman, E.R. Multilayer flow modulator enhances vital organ perfusion in patients with type B aortic dissection. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1182–H1193. [Google Scholar] [CrossRef]
- Tombetti, E.; Godi, C.; Ambrosi, A.; Doyle, F.; Jacobs, A.; Kiprianos, A.P.; Youngstein, T.; Bechman, K.; Manfredi, A.A.; Ariff, B.; et al. Novel Angiographic Scores for evaluation of Large Vessel Vasculitis. Sci. Rep. 2018, 8, 15979. [Google Scholar] [CrossRef]
- Chocron, S.; Vaislic, C.; Kaili, D.; Bonneville, J.-F. Multilayer stents in the treatment of thoraco-abdominal residual type B dissection. Interact. Cardiovasc. Thorac. Surg. 2011, 12, 1057–1059. [Google Scholar] [CrossRef] [Green Version]
- Sultan, S.; Hynes, N.; Kavanagh, E.P.; Diethrich, E.B. How does the multilayer flow modulator work? The science behind the technical innovation. J. Endovasc. Ther. 2014, 21, 814–821. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Cases | Pre-Op Aorta Vol. (cm3) | Post-Op Aorta Vol. (cm3) | Latest Follow-Up Aorta Vol. (cm3) | No of Months-Follow-Up |
|---|---|---|---|---|
| 1 | 110.34 | 99.69 | 94.00 | 36 |
| 2 | 319.80 | 283.88 | 189.61 | 36 |
| 3 | 248.70 | 225.90 | 258.35 | 36 |
| 4 | 235.32 | 261.38 | 264.38 | 24 |
| 5 | 370.89 | 385.22 | 393.14 | 30 |
| 6 | n/a | 341.36 | 308.14 | 12 |
| 7 | 16.33 | 32.55 | 33.15 | 24 |
| 8 | 495.22 | 526.99 | 375.65 | 12 |
| 9 | 244.51 | 252.79 | 461.74 | 36 |
| 10 | 335.78 | 355.00 | 377.14 | 12 |
| 11 | 482.68 | 511.44 | 510.38 | 6 |
| 12 | 238.14 | 251.79 | 255.32 | 6 |
| 13 | 380.53 | 314.23 | 357.82 | 6 |
| 14 | 334.23 | 312.83 | 428.51 | 6 |
| 15 | 242.27 | 299.27 | 324.20 | 1 |
| 16 | 431.65 | 418.88 | 624.43 | 12 |
| Cases | Pre-Op | Post-Op | Latest Follow-Up | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TL vol. (cm3) | FL vol. (cm3) | TL at PMC 1 (cm) | FLI | TL vol. (cm3) | FL vol. (cm3) | TL at PMC 1 (cm) | FLI | TL vol. (cm3) | FL vol. (cm3) | TL at PMC 1 (cm) | FLI | |
| 1 | 33.29 | 77.05 | 0.44 | 2.31 | 68.29 | 31.4 | 1.61 | 0.46 | 93.32 | 0.68 | 1.79 | 0.01 |
| 2 | 63.4 | 256.4 | 0.96 | 4.04 | 106.71 | 177.17 | 2.25 | 1.66 | 187.08 | 2.53 | 3.08 | 0.01 |
| 3 | 100.17 | 148.53 | 0.6 | 1.48 | 92.6 | 133.3 | 0.64 | 1.44 | 170.38 | 87.97 | 2.67 | 0.52 |
| 4 | 96.33 | 138.99 | 0.87 | 1.44 | 194.11 | 67.27 | 2.2 | 0.35 | 177.95 | 86.43 | 2.11 | 0.49 |
| 5 | 71.09 | 299.8 | 0.6 | 4.22 | 136.24 | 248.98 | 2.06 | 1.83 | 106.4 | 286.74 | 1.8 | 2.69 |
| 6 | n/a | n/a | n/a | n/a | 231.74 | 109.62 | 2.34 | 0.47 | 246.75 | 61.39 | 2.32 | 0.25 |
| 7 | 13.34 | 2.99 | 2.33 | 0.22 | 26.96 | 5.59 | 2.39 | 0.21 | 28.49 | 4.66 | 2.4 | 0.16 |
| 8 | 83.18 | 412.04 | 0.65 | 4.95 | 182.56 | 344.43 | 1.8 | 1.89 | 130.76 | 244.89 | 1.84 | 1.87 |
| 9 | 26.21 | 218.3 | 0.16 | 8.33 | 195.93 | 56.86 | 2.56 | 0.29 | 250.1 | 211.64 | 2.71 | 0.85 |
| 10 | 36.61 | 299.17 | 0.2 | 8.17 | 138.12 | 216.88 | 1.72 | 1.57 | 166.44 | 210.7 | 1.75 | 1.27 |
| 11 | 131 | 351.68 | 0.68 | 2.68 | 244.19 | 267.25 | 2.17 | 1.09 | 250.65 | 259.73 | 2.13 | 1.04 |
| 12 | 19.77 | 218.37 | 0.15 | 11.05 | 112.84 | 138.95 | 1.87 | 1.23 | 131.08 | 124.24 | 1.8 | 0.95 |
| 13 | 168 | 212.53 | 0.76 | 1.27 | 188.16 | 126.07 | 1.95 | 0.67 | 235.22 | 122.6 | 2.22 | 0.52 |
| 14 | 131.5 | 202.73 | 0.35 | 1.54 | 178.75 | 134.08 | 2.19 | 0.75 | 227.4 | 201.11 | 2.45 | 0.88 |
| 15 | 121.61 | 120.66 | 1.08 | 0.99 | 210.45 | 88.82 | 2.08 | 0.42 | 234.9 | 89.3 | 2.25 | 0.38 |
| 16 | 43.4 | 388.25 | 0.56 | 8.95 | 115.63 | 303.25 | 1.76 | 2.62 | 124.95 | 499.48 | 1.65 | 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costache, V.S.; Meekel, J.P.; Costache, A.; Melnic, T.; Solomon, C.; Chitic, A.M.; Bucurenciu, C.; Moldovan, H.; Antoniac, I.; Candea, G.; et al. Geometric Analysis of Type B Aortic Dissections Shows Aortic Remodeling After Intervention Using Multilayer Stents. Materials 2020, 13, 2274. https://doi.org/10.3390/ma13102274
Costache VS, Meekel JP, Costache A, Melnic T, Solomon C, Chitic AM, Bucurenciu C, Moldovan H, Antoniac I, Candea G, et al. Geometric Analysis of Type B Aortic Dissections Shows Aortic Remodeling After Intervention Using Multilayer Stents. Materials. 2020; 13(10):2274. https://doi.org/10.3390/ma13102274
Chicago/Turabian StyleCostache, Victor S., Jorn P. Meekel, Andreea Costache, Tatiana Melnic, Crina Solomon, Anca M. Chitic, Cristian Bucurenciu, Horatiu Moldovan, Iulian Antoniac, Gabriela Candea, and et al. 2020. "Geometric Analysis of Type B Aortic Dissections Shows Aortic Remodeling After Intervention Using Multilayer Stents" Materials 13, no. 10: 2274. https://doi.org/10.3390/ma13102274