Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
- P—Children (age < 18) with ASD
- I—VR-based treatment
- C—(versus) non-VR-based treatment, children’s condition before VR-based treatment, without treatment.
- O—Main outcomes obtained, no significant improvement is needed.
2.3. Selection Process
2.4. Data Extraction
3. Results
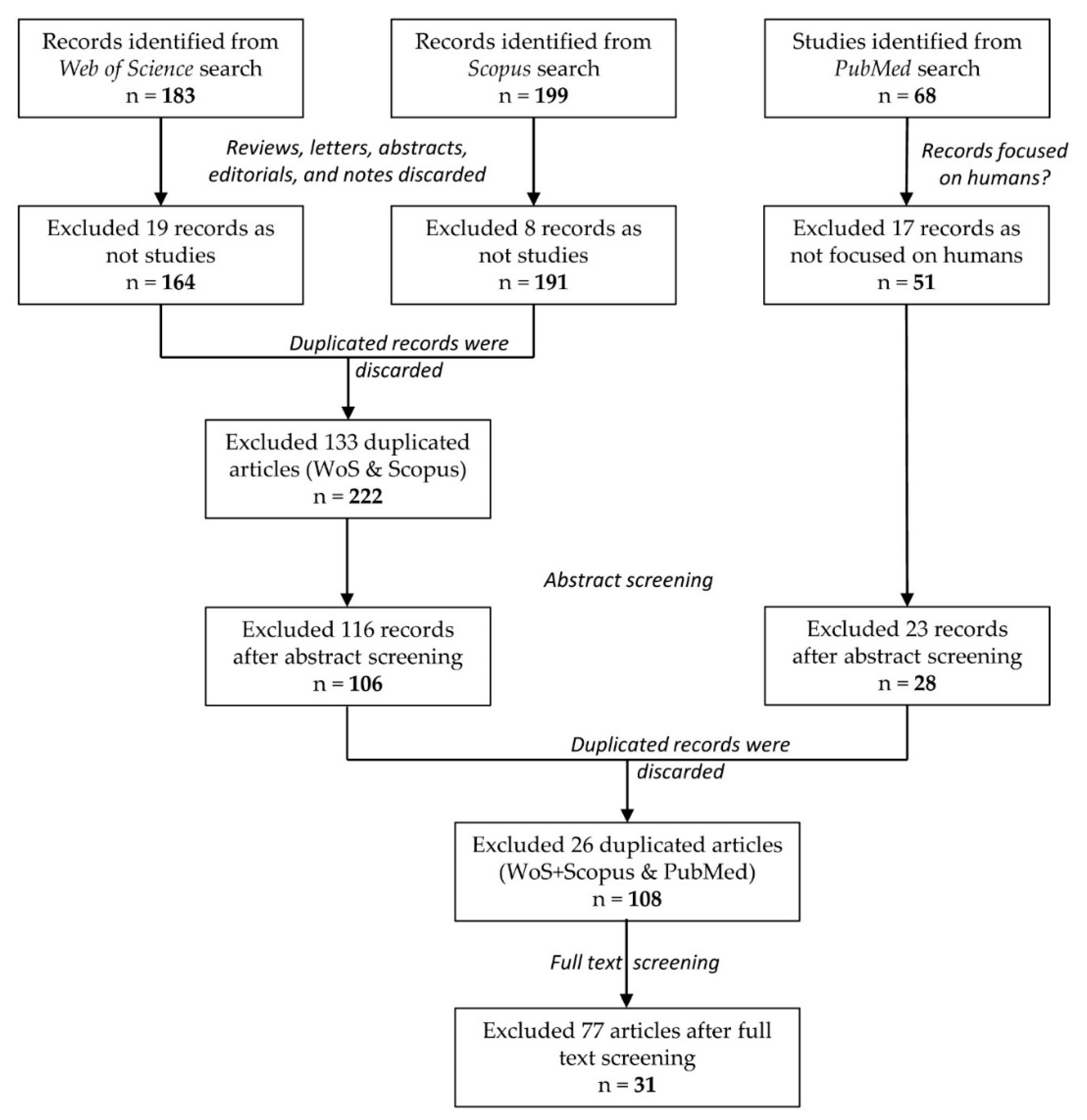
3.1. Study Selection
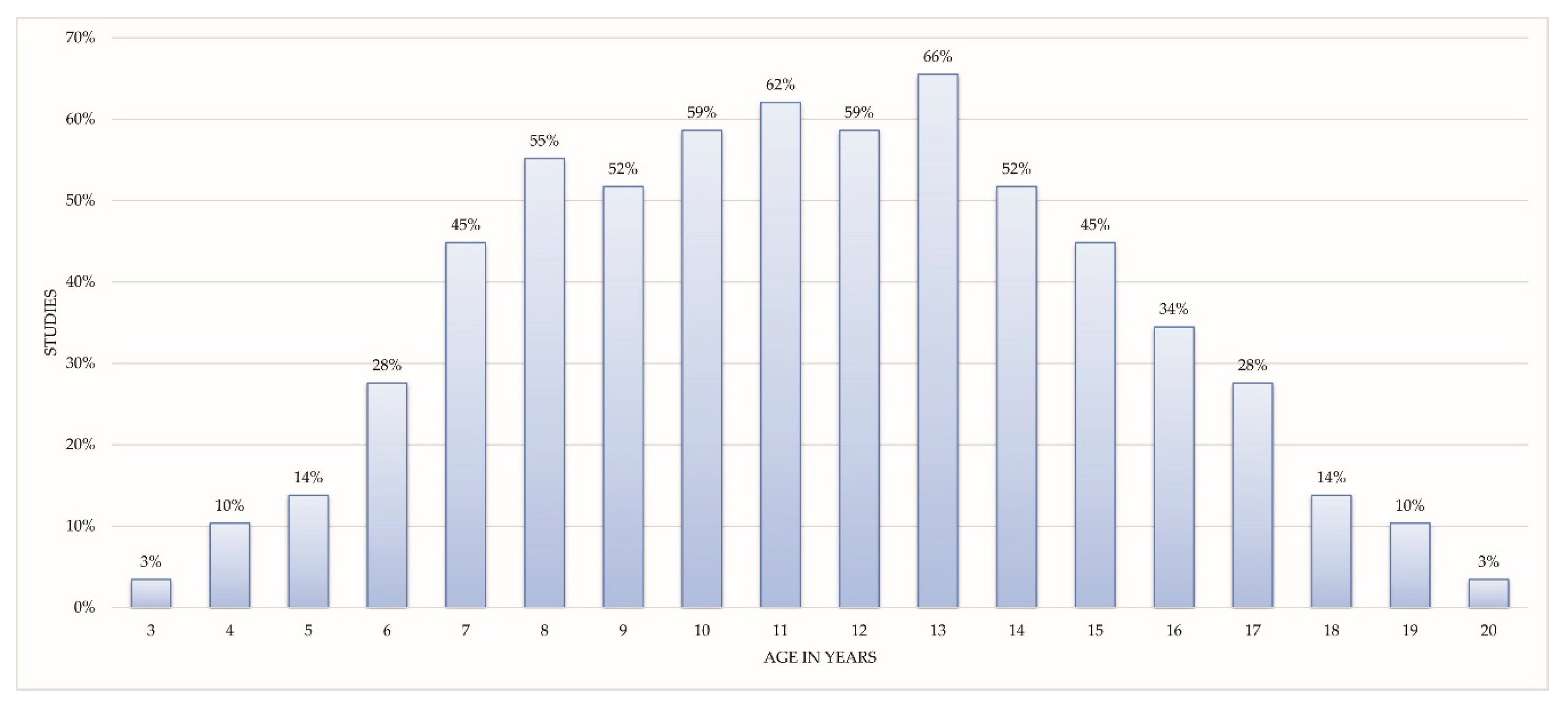
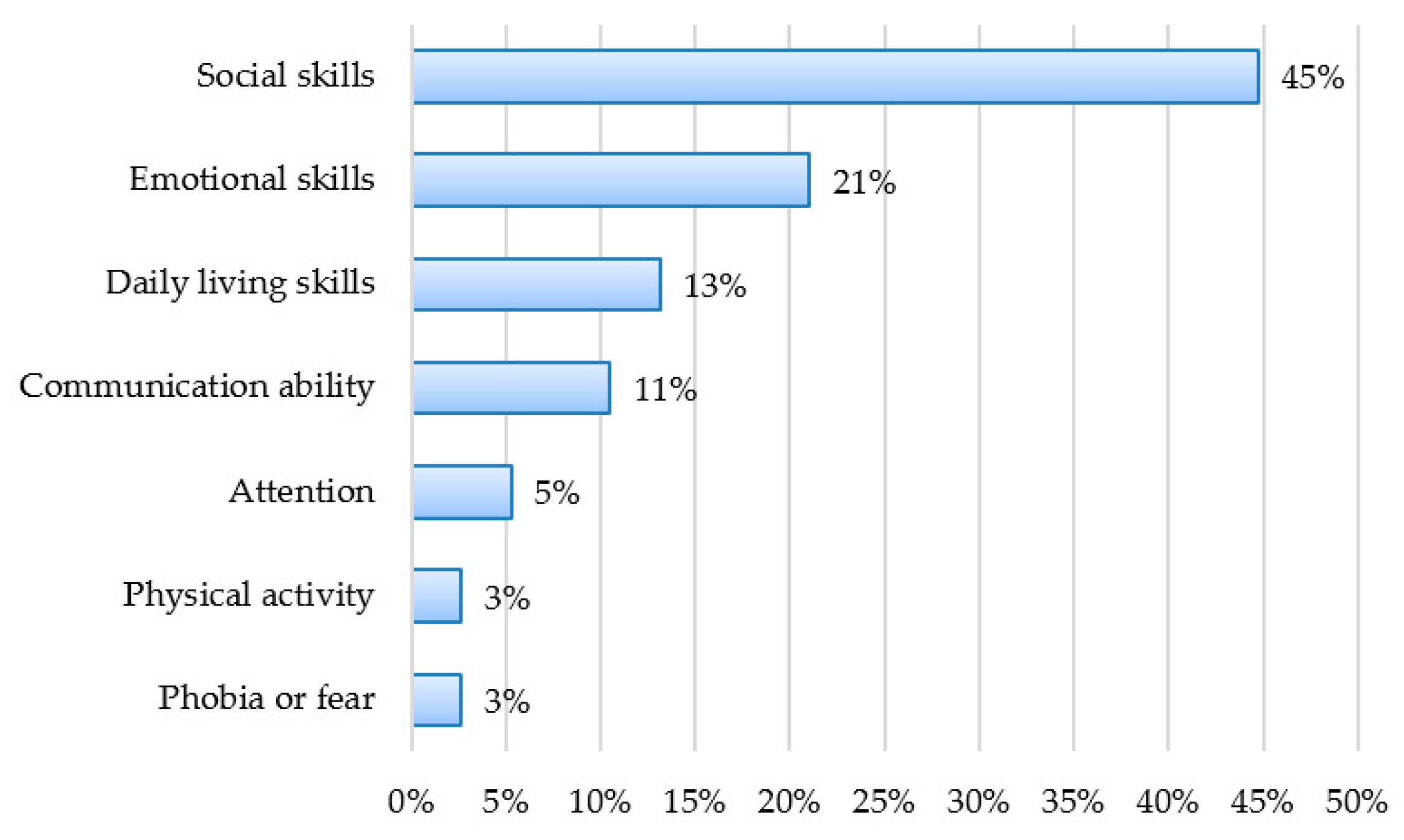
3.2. Study Characteristics
3.2.1. Social Skills
3.2.2. Emotional Skills
3.2.3. Daily Living Skills
3.2.4. Communication Ability
3.2.5. Attention
3.2.6. Physical Activity
3.2.7. Phobia or Fear
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. Available online: http://www.who.int/en/news-room/fact-sheets/detail/autism-spectrum-disorders (accessed on 12 May 2018).
- Colombi, C.; Ghaziuddin, M. Neuropsychological Characteristics of Children with Mixed Autism and ADHD. Autism Res. Treat. 2017, 2017, 5781781. [Google Scholar] [CrossRef] [PubMed]
- Merriam-Webster. Available online: https://www.merriam-webster.com/dictionary/virtual%20reality (accessed on 20 February 2018).
- Bird, M.L.; Cannell, J.; Jovic, E.; Rathjen, A.; Lane, K.; Tyson, A.; Callisaya, M.; Smith, S. A Randomized Controlled Trial Investigating the Efficacy of Virtual Reality in Inpatient Stroke Rehabilitation. Arch. Phys. Med. Rehabil. 2017, 98, e27. [Google Scholar] [CrossRef]
- Albiol-Perez, S.; Gil-Gomez, J.A.; Munoz-Tomas, M.T.; Gil-Gomez, H.; Vial-Escolano, R.; Lozano-Quilis, J.A. The effect of balance training on postural control in patients with Parkinson’s disease using a virtual rehabilitation system. Methods Inf. Med. 2017, 56, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Palacios, A.; Herrero, R.; Vizcaíno, Y.; Belmonte, M.A.; Castilla, D.; Molinari, G.; Baños, R.M.; Botella, C. Integrating Virtual Reality With Activity Management for the Treatment of Fibromyalgia: Acceptability and Preliminary Efficacy. Clin. J. Pain 2015, 31, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes: A Randomized Controlled Trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Orlosky, J.; Itoh, Y.; Ranchet, M.; Kiyokawa, K.; Morgan, J.; Devos, H. Emulation of Physician Tasks in Eye-Tracked Virtual Reality for Remote Diagnosis of Neurodegenerative Disease. IEEE Trans. Vis. Comput. Graph. 2017, 23, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Areces, D.; Rodríguez, C.; García, T.; Cueli, M.; González-Castro, P. Efficacy of a Continuous Performance Test Based on Virtual Reality in the Diagnosis of ADHD and Its Clinical Presentations. J. Atten. Disord. 2016, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Phé, V.; Cattarino, S.; Parra, J.; Bitker, M.O.; Ambrogi, V.; Vaessen, C.; Rouprêt, M. Outcomes of a virtual-reality simulator-training programme on basic surgical skills in robot-assisted laparoscopic surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2016, 13, e1740. [Google Scholar] [CrossRef] [PubMed]
- Pulijala, Y.; Ma, M.; Pears, M.; Peebles, D.; Ayoub, A. Effectiveness of Immersive Virtual Reality in Surgical Training—A Randomized Control Trial. J. Oral Maxillofac. Surg. 2017. [Google Scholar] [CrossRef] [PubMed]
- Jarrold, W.; Mundy, P.; Gwaltney, M.; Bailenson, J.; Hatt, N.; McIntyre, N.; Kim, K.; Solomon, M.; Novotny, S.; Swain, L. Social attention in a virtual public speaking task in higher functioning children with autism. Autism Res. 2013, 6, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Mishkind, M.C.; Norr, A.M.; Katz, A.C.; Reger, G.M. Review of Virtual Reality Treatment in Psychiatry: Evidence Versus Current Diffusion and Use. Curr. Psychiatry Rep. 2017, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.Y.; Wu, Q.; Zhao, W.B.; Luo, X. Technology-Facilitated Diagnosis and Treatment of Individuals with Autism Spectrum Disorder: An Engineering Perspective. Appl. Sci. 2017, 7, 1051. [Google Scholar] [CrossRef]
- Van Bennekom, M.J.; de Koning, P.P.; Denys, D. Virtual Reality Objectifies the Diagnosis of Psychiatric Disorders: A Literature Review. Front. Psychiatry 2017, 8, 163. [Google Scholar] [CrossRef] [PubMed]
- Provoost, S.; Lau, H.M.; Ruwaard, J.; Riper, H. Embodied Conversational Agents in Clinical Psychology: A Scoping Review. J. Med. Internet Res. 2017, 19, e151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, H.M.; Smit, J.H.; Fleming, T.M.; Riper, H. Serious Games for Mental Health: Are They Accessible, Feasible, and effective? A Systematic Review and Meta-analysis. Front. Psychiatry 2017, 7, 209. [Google Scholar] [CrossRef] [PubMed]
- Parsons, S. Authenticity in Virtual Reality for assessment and intervention in autism: A conceptual review. Educ. Res. Rev. 2016, 19, 138–157. [Google Scholar] [CrossRef] [Green Version]
- Den Brok, W.L.J.E.; Sterkenburg, P.S. Self-controlled technologies to support skill attainment in persons with an autism spectrum disorder and/or an intellectual disability: A systematic literature review. Disabil. Rehabil. Assist. Technol. 2015, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ip, H.H.S.; Wong, S.W.L.; Chan, D.F.Y.; Byrne, J.; Li, C.; Yuan, V.S.N.; Lau, K.S.Y.; Wong, J.Y.W. Enhance emotional and social adaptation skills for children with autism spectrum disorder: A virtual reality enabled approach. Comput. Educ. 2018, 117, 1–15. [Google Scholar] [CrossRef]
- Manju, T.; Padmavathi, S.; Tamilselvi, D. A Rehabilitation Therapy for Autism Spectrum Disorder Using Virtual Reality. In Smart Secure Systems—IoT and Analytics Perspective, 1st ed.; Venkataramani, G., Sankaranarayanan, K., Mukherjee, S., Arputharaj, K., Sankara Narayanan, S., Eds.; Springer: Singapore, 2018; Volume 808, pp. 328–336. ISBN 978-981-10-7634-3. [Google Scholar]
- Taryadi, B.R.; Kurniawan, I. The improvement of autism spectrum disorders on children communication ability with PECS method Multimedia Augmented Reality-Based. In Journal of Physics: Conference Series, 1st ed.; Rahayu, Y.S., Ekawati, R., Nandiyanto, A.B.D., Lukito, A., Wibawa, S.C., Eds.; IOP Publishing: Bristol, UK, 2018; Volume 947, pp. 1–7. ISSN 1742-6588. [Google Scholar]
- Adjorlu, A.; Høeg, E.; Mangano, L.; Serafin, S. Daily Living Skills Training in Virtual Reality to Help Children with Autism Spectrum Disorder in a Real Shopping Scenario. In Proceedings of the 16th IEEE International Symposium on Mixed and Augmented Reality, Nantes, France, 9–13 October 2017; IEEE Computer Society Conference Publishing Services: Washington, DC, USA, 2017; pp. 294–302. [Google Scholar]
- Lamash, L.; Klinger, E.; Josman, N. Using a virtual supermarket to promote independent functioning among adolescents with Autism Spectrum Disorder. In Proceedings of the 2017 International Conference on Virtual Rehabilitation, Montreal, QC, Canada, 19–22 June 2017; IEEE Computer Society Conference Publishing Services: Washington, DC, USA, 2017; pp. 1–7. [Google Scholar]
- Bekele, E.; Wade, J.; Bian, D.; Fan, J.; Swanson, A.; Warren, Z.; Sarkar, N. Multimodal adaptive social interaction in virtual environment (MASI-VR) for children with Autism spectrum disorders (ASD). In Virtual Reality (VR); IEEE: Piscataway, NJ, USA, 2016; pp. 121–130. [Google Scholar]
- Chen, C.H.; Lee, I.J.; Lin, L.Y. Augmented reality-based video-modeling storybook of nonverbal facial cues for children with autism spectrum disorder to improve their perceptions and judgments of facial expressions and emotions. Comput. Hum. Behav. 2016, 55, 477–485. [Google Scholar] [CrossRef]
- Didehbani, N.; Allen, T.; Kandalaft, M.; Krawczyk, D.; Chapman, S. Virtual Reality Social Cognition Training for children with high functioning autism. Comput. Hum. Behav. 2016, 62, 703–711. [Google Scholar] [CrossRef]
- Ip, H.H.; Wong, S.W.; Chan, D.F.; Byrne, J.; Li, C.; Yuan, V.S.; Lau, K.S.; Wong, J.Y. Virtual reality enabled training for social adaptation in inclusive education settings for school-aged children with autism spectrum disorder (ASD). In Proceedings of the International Conference on Blending Learning, Beijing, China, 19–21 July 2016; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Lorenzo, G.; Lledó, A.; Pomares, J.; Roig, R. Design and application of an immersive virtual reality system to enhance emotional skills for children with autism spectrum disorders. Comput. Educ. 2016, 98, 192–205. [Google Scholar] [CrossRef]
- Wade, J.; Zhang, L.; Bian, D.; Fan, J.; Swanson, A.; Weitlauf, A.; Sarkar, M.; Warren, Z.; Sarkar, N. A Gaze-Contingent Adaptive Virtual Reality Driving Environment for Intervention in Individuals with Autism Spectrum Disorders. ACM Trans. Interact. Intell. Syst. 2016, 6, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Ke, F.; Lee, S. Virtual reality based collaborative design by children with high-functioning autism: Design-based flexibility, identity, and norm construction. Interact. Learn. Environ. 2016, 24, 1511–1533. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, I.J.; Lin, L.Y. Augmented reality-based self-facial modeling to promote the emotional expression and social skills of adolescents with autism spectrum disorders. Res. Dev. Disabil. 2015, 36, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Huang, C.L.; Yang, C.S. Using a 3D Immersive Virtual Environment System to Enhance Social Understanding and Social Skills for Children with Autism Spectrum Disorders. Focus Autism Other Dev. Disabl. 2015, 30, 222–236. [Google Scholar] [CrossRef]
- Kim, K.; Rosenthal, M.Z.; Gwaltney, M.; Jarrold, W.; Hatt, N.; McIntyre, N.; Swain, L.; Solomon, M.; Mundy, P. A Virtual Joy-Stick Study of Emotional Responses and Social Motivation in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 3891–3899. [Google Scholar] [CrossRef] [PubMed]
- Parsons, S. Learning to work together: Designing a multi-user virtual reality game for social collaboration and perspective-taking for children with autism. Int. J. Child-Comput. Interact. 2015, 6, 28–38. [Google Scholar] [CrossRef] [Green Version]
- Zhen, B.; Blackwell, A.F.; Coulouris, G. Using augmented reality to elicit pretend play for children with autism. IEEE Trans. Vis. Comput. Graph. 2015, 21, 598–610. [Google Scholar] [CrossRef]
- Bekele, E.; Crittendon, J.; Zheng, Z.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. Assessing the utility of a virtual environment for enhancing facial affect recognition in adolescents with autism. J. Autism Dev. Disord. 2014, 44, 1641–1650. [Google Scholar] [CrossRef] [PubMed]
- Escobedo, L.; Tentori, M.; Quintana, E.; Favela, J.; Garcia-Rosas, D. Using augmented reality to help children with autism stay focused. IEEE Pervasive Comput. 2014, 13, 38–46. [Google Scholar] [CrossRef]
- Finkelstein, S.; Barnes, T.; Wartell, Z.; Suma, E.A. Evaluation of the exertion and motivation factors of a virtual reality exercise game for children with autism. IEEE Virtual Real. 2014, 11–16, 11–16. [Google Scholar] [CrossRef]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing specific phobia/fear in young people with autism spectrum disorders (ASDs) through a virtual reality environment intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef] [PubMed]
- Stichter, J.P.; Laffey, J.; Galyen, K.; Herzog, M. iSocial: Delivering the Social Competence Intervention for Adolescents (SCI-A) in a 3D virtual learning environment for youth with high functioning autism. J. Autism Dev. Disord. 2014, 44, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Bekele, E.; Zheng, Z.; Swanson, A.; Crittendon, J.; Warren, Z.; Sarkar, N. Understanding how adolescents with autism respond to facial expressions in virtual reality environments. IEEE Trans. Vis. Comput. Graph. 2013, 19, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Bernardini, S.; Porayska-Pomsta, K.; Sampath, H. Designing an intelligent virtual agent for social communication in autism. In Proceedings of the Ninth AAAI Conference on Artificial Intelligence and Interactive Digital Entertainment (AIIDE′13), Boston, MA, USA, 14–18 October 2013; pp. 9–15. [Google Scholar]
- Cai, Y.; Chia, N.K.; Thalmann, D.; Kee, N.K.; Zheng, J.; Thalmann, N.M. Design and development of a Virtual Dolphinarium for children with autism. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Fengfeng, K.; Tami, I. Virtual-Reality-based social interaction training for children with high-functioning autism. J. Educ. Res. 2013, 106, 441–461. [Google Scholar] [CrossRef]
- Lorenzo, G.; Pomares, J.; Lledó, A. Inclusion of immersive virtual learning environments and visual control systems to support the learning of students with Asperger syndrome. Comput. Educ. 2013, 62, 88–101. [Google Scholar] [CrossRef]
- Modugumudi, Y.R.; Santhosh, J.; Anand, S. Efficacy of collaborative virtual environment intervention programs in emotion expression of children with autism. J. Med. Imaging Health Inf. 2013, 3, 321–325. [Google Scholar] [CrossRef]
- Wang, M.; Reid, D. Using the virtual reality-cognitive rehabilitation approach to improve contextual processing in children with autism. Sci. World J. 2013, 13, 716890. [Google Scholar] [CrossRef] [PubMed]
- Alcorn, A.; Pain, H.; Rajendran, G.; Smith, T.; Lemon, O.; Porayska-Pomsta, K.; Foster, M.E.; Avramides, K.; Frauenberger, C.; Bernardini, S. Social Communication between Virtual Characters and Children with Autism. In Artificial Intelligence in Education; Lecture Notes in Computer Science; Biswas, G., Bull, S., Kay, J., Mitrovic, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6738. [Google Scholar]
- Milne, M.; Luerssen, M.H.; Lewis, T.W.; Leibbrandt, L.E.; Powers, D.M.W. Development of a virtual agent based social tutor for children with autism spectrum disorders. In Proceedings of the 2010 International Joint Conference on Neural Networks (IJCNN), Barcelona, Spain, 18–23 July 2010; pp. 1–9. [Google Scholar] [CrossRef]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesa-Gresa, P.; Lozano, J.A.; Llórens, R.; Alcañiz, M.; Navarro, M.D.; Noé, E. Clinical Validation of a Virtual Environment Test for Safe Street Crossing in the Assessment of Acquired Brain Injury Patients with and without Neglect. Lect. Notes Comput. Sci. 2011, 6947. [Google Scholar] [CrossRef]
- Brooks, B.M.; Rose, F.D. The use of virtual reality in memory rehabilitation: Current findings and future directions. NeuroRehabilitation 2003, 18, 147–157. [Google Scholar] [PubMed]
- Spreij, L.A.; Visser-Meily, J.M.; van Heugten, C.M.; Nijboer, T.C. Novel insights into the rehabilitation of memory post acquired brain injury: A systematic review. Front. Hum. Neurosci. 2014, 8, 993. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, E.; Pullman, S.; McGuire, A. Using Virtual Reality and Videogames for Traumatic Brain Injury Rehabilitation: A Structured Literature Review. Games Health J. 2014, 3, 202–214. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Contribution | Diagnosis | Groups (Sex)/Age | Aim | Evaluation | Main Results |
|---|---|---|---|---|---|
| Ip et al. [21] 2018 | ASD | EG: 36 (31 M, 5 F) CG: 36 (33 M, 3 F) Age: 7–10 y/o | Enhance emotional and social adaptation skills. | FT, ET, PEP-3, ABAS-II. | Improvements in children’s emotion expression and regulation and social-emotional reciprocity. |
| Manju et al. [22] 2018 | ASD | EG: 5 CG: - Age: 4–6 y/o | Enhance social skills, emotions and attention. | Specific scoring criteria based on a Likert scale method. | Improvements in all the participants, but statistical significance is not analyzed. |
| Taryadi and Kurniawan [23] 2018 | ASD | EG: 12 CG: - Age not specified | Improve communication ability. | Subjective qualitative analysis. | Improvement of communication ability, but statistical significance is not analyzed. |
| Adjorlu et al. [24] 2017 | ASD | EG: 4 CG: 5 Age: 12–15 y/o | Development of daily living skills (shopping skills) | Task completion time and effectiveness, questionnaires, observations. | Some of the indicators show significant improvement. |
| Lamash et al. [25] 2017 | ASD | EG: 33 (29 M, 4 F) CG: 23 (17 M, 6 F) Age: 11–19 y/o | Improve the implementation of a shopping task. | WebNeuro, BRIEFSR, and the TOGSS. | Significant improvement of the EG compared to the CG in several indices. |
| Bekele et al. [26] 2016 | HFASD | EG: 6 (6 M) CG: 6 (6 M) Age: 13–17 y/o | Emotion recognition in a social context. | Isolated emotion recognition test, NEPSY test. | System useful in training core deficit areas for eventual better social functioning. |
| Chen et al. [27] 2016 | ASD | EG: 6 (5 M, 1 F) CG: - Age: 11–13 y/o | Identify the 6 core emotions. | Specific questions. | All scores rose significantly during the intervention and remained significantly high. |
| Didehbani et al. [28] 2016 | ASD (17) ASD+ADHD (13) | EG: 30 (26 M, 4 F) CG: - Age: 7–16 y/o | Enhance social skills. | NEPSY-II, Triangles (Social Attribution Task). | Improvements in emotion recognition, social attribution, and executive function. |
| Ip et al. [29] 2016 | ASD or suspected ASD | EG: 52 CG: - Age: 6–11 y/o | Enhance emotional and social adaptation skills. | FT, ET, PEP-3. | Emotion recognition: SD in ET. Affective expression: SD. Social reciprocity: SD. Overall SD for PEP-3. |
| Lorenzo et al. [30] 2016 | ASD | EG: 20 (14 M, 6 F) CG: 20 (15 M, 5 F) Age: 7–12 y/o | Improve emotional skills. | Specific emotional script. Computer vision system to obtain child’s expressions. | Significant improvement in emotional competences. |
| Wade et al. [31] 2016 | ASD | EG: 20 (19 M, 1 F) CG: - Age: 13–18 y/o | Develop daily living skills (driving). | Physiological and EEG data. Gaze data. Subjective observations. | The system may be beneficial in teaching driving skills. SD in most of the measures. |
| Ke and Lee [32] 2015 | HFASD | EG: 3 CG: - Age: 8–11 y/o | Social skills development. | Qualitative time-series and micro-behavior analyses. | Practice and develop flexibility, identity, and norm construction. |
| Chen et al. [33] 2015 | ASD | EG: 3 (2 M, 1 F) CG: - Age: 10–13 y/o | Identify the 6 core emotions. | Correct assessment rates. | SD for all participants. |
| Cheng et al [34] 2015 | ASD | EG: 3 (3 M) CG: - Age: 10–12 y/o | Improve social understanding and skills. | 2 specific scales: Social events card and social behaviors scale | Improvement in the utilization of reciprocal interactions. |
| Kim et al. [35] 2015 | HFASD | EG: 19 (13 M, 6 F) CG: 23 (16 M, 7 F) Age: 8–16 y/o | Examining approach and tendencies in the recognition of emotions. | The final joystick position. Test for symptomatology, cognition and emotion. | EG displayed significantly less approach behavior to positive expressions to happiness than CG. |
| Parsons [36] 2015 | ASD | EG: 6 CG: 8 Age: 7–13 y/o | Collaboration and reciprocity in behavior and communication. | Analysis of collaborative and non-collaborative interactions. | ASD children showed efforts in collaboration and reciprocity of communication. |
| Bai et al. [37] 2015 | ASD or Asperger Syndrome | EG: 12 (10 M, 2 F) CG: - Age: 4–7 y/o | Representation of pretense and promote pretend play. | Video analysis of play behavior. Parent and participant questionnaire. | Positive effects of elicited pretend play in children with ASD. |
| Bekele et al. [38] 2014 | ASD | EG: 10 (ASD) CG: 10 (TD) Age: 13–17 y/o | Performance in facial affect recognition.Gaze patterns. | Accuracy, response latency, and ratings of response confidence.Time spent looking at locations. | Similar accuracy at facial recognition. ASD children endorsed lower confidence, and substantial variation in gaze patterns. |
| Escobedo et al. [39] 2014 | LFASD | EG: 12 CG: - Age: 3–8 y/o | Train selective attention.Elicitation of positive emotions. | System registration of selective and sustained attention, ability to attend the therapy, emotions. | Application seems to increase attention and improve elicitation of positive emotions. |
| Finkelstein et al. [40] 2014 | ASD | EG: 10 CG: - Age: 8–20 y/o | Improve physical activity and motivation. | Post-experimental questionnaire. Physiological measures. | Children showed vigorous play activity and motivation to repeat the game. |
| Maskey et al. [41] 2014 | ASD with phobia/fear | EG: 9 (9 M)CG: - Age: 7–13 y/o | Reduction of specific phobia or fear. | SCAS-P and SCAS-C, confident ratings, report of the family, anxiety report and test. | CBT techniques combined with VRE were effective in the treatment of phobia/fear in children with ASD. |
| Stitcher et al. [42] 2014 | ASD | EG: 11 (11 M) CG: - Age: 11–14 y/o | Enhance social competence in ASD. | SRS, BRIEF, RMET, Faux Pas Stories, Strange Stories, DANVA-2-CF; D-KEFS; CPT-II. | Improvement in social responsiveness and executive functioning skills. |
| Bekele et al. [43] 2013 | HFASD | EG: 10 (8 M, 2 F) CG: 10 (8 M, 2 F) Age: 13–17 y/o | Evaluate usability.Behavioral and physiological difference. | Performance data, eye tracking indices and physiological features. | Differences in the way adolescents with ASD process and recognize emotional faces compared to their TD peers. |
| Bernardini et al. [44] 2013 | ASD | EG: 19 CG: - Age not specified | Acquire social communication skills in ASD. | Assessment based on a structured table-top turn-taking activity (social skills). | Game seems to improve few aspects of social skills. |
| Cai et al. [45] 2013 | ASD | EG: 15 (13 M, 2 F) CG: - Age: 6–17 y/o | Intervention in nonverbal gesturing communication. | TONI-3 and GARS tests. Observation of final task (dolphin training). | Inconclusive data, no statistical analysis. |
| Fengfeng Ke & Tami Im [46] 2013 | HFASD or Asperger Syndrome | EG: 4 (2 M, 2 F) CG: - Age: 9–10 y/o | Improve social interaction. | Physical and virtual communication behaviors, SSQ, Perception of Emotion. | Improvement in performance of social tasks after VR intervention. |
| Lorenzo et al. [47] 2013 | Asperger Syndrome | EG: 20 (16 M, 4 F) CG: - Age: 8–15 y/o | Improve social skills and executive functions. | Interviews (teachers) and assessment of behavior during tasks. | Improvement of executive functions and social skills. Some skills were transferred to school context. |
| Modugumudi et al. [48] 2013 | ASD | EG: 10 (9 M, 1 F) CG: 10 (M) Age: 7–19 y/o | Recognition and expression of emotions. | Neurophysiological measures pre- & post-treatment: EEG, EOG. | Significant improvement in children with CVE intervention program. |
| Wang & Reid [49] 2013 | ASD | EG: 4 (3 M, 1 F) CG: - Age: 6–8 y/o | Train contextual processing of objects. | FIST-m, ASS, VR test of contextual processing of objects, final feedback questionnaire. | Improvement in contextual processing of objects and cognitive flexibility. |
| Alcorn et al. [50] 2011 | ASD | EG: 32 (29 M, 3 F) CG: - Age: 5–14 y/o | Teach children to follow a virtual character’s gaze and gesture cues. | Observational and video data. Reaction time. | Children were able to successfully complete the tasks. Perception of the VR character as an intentional being. |
| Milne et al. [51] 2010 | HFASD or Asperger Syndrome | EG: 14 Age: 6–15 y/o | Social skills. | Pre-test and post-test questions in each round. | Children gained information about conversation and bullying skills. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. https://doi.org/10.3390/s18082486
Mesa-Gresa P, Gil-Gómez H, Lozano-Quilis J-A, Gil-Gómez J-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors. 2018; 18(8):2486. https://doi.org/10.3390/s18082486
Chicago/Turabian StyleMesa-Gresa, Patricia, Hermenegildo Gil-Gómez, José-Antonio Lozano-Quilis, and José-Antonio Gil-Gómez. 2018. "Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review" Sensors 18, no. 8: 2486. https://doi.org/10.3390/s18082486