High-Contrast Imaging of Cholesterol Crystals in Rabbit Arteries Ex Vivo Using LED-Based Polarization Microscopy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
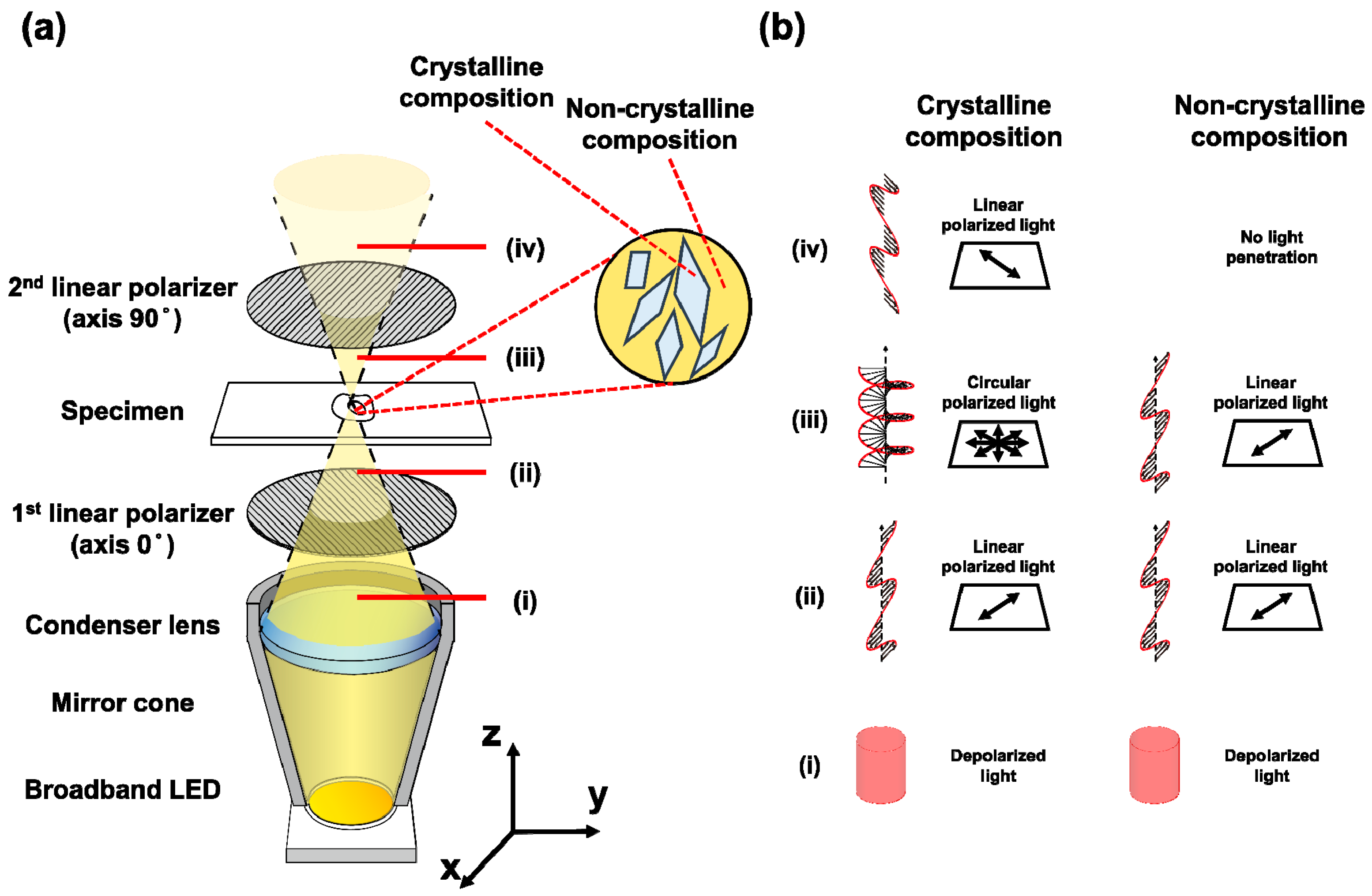
2.1. Polarization Microscopy System
2.2. Ex Vivo Sample Preparation
2.3. Ethical Statement
2.4. Experimental Procedures
3. Results
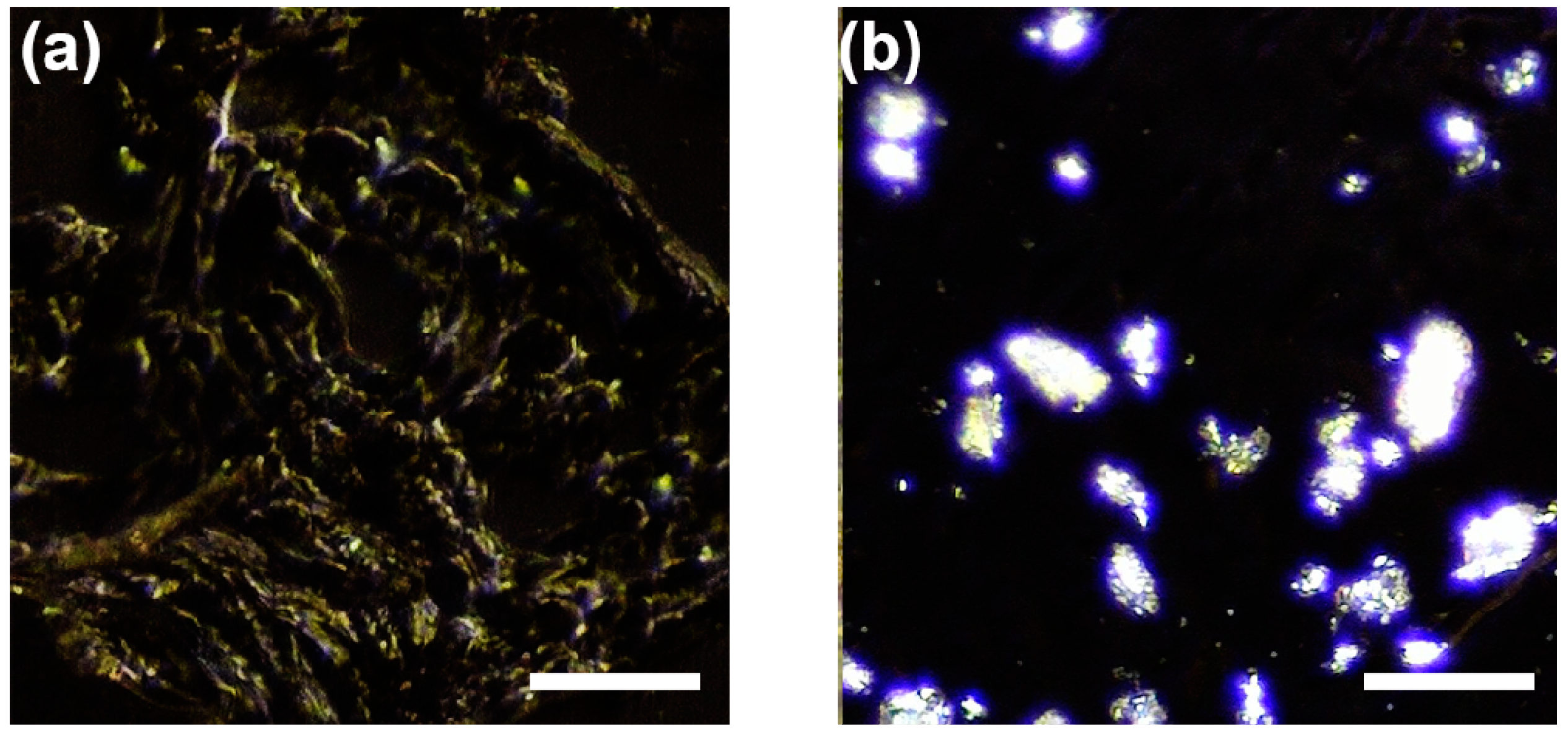
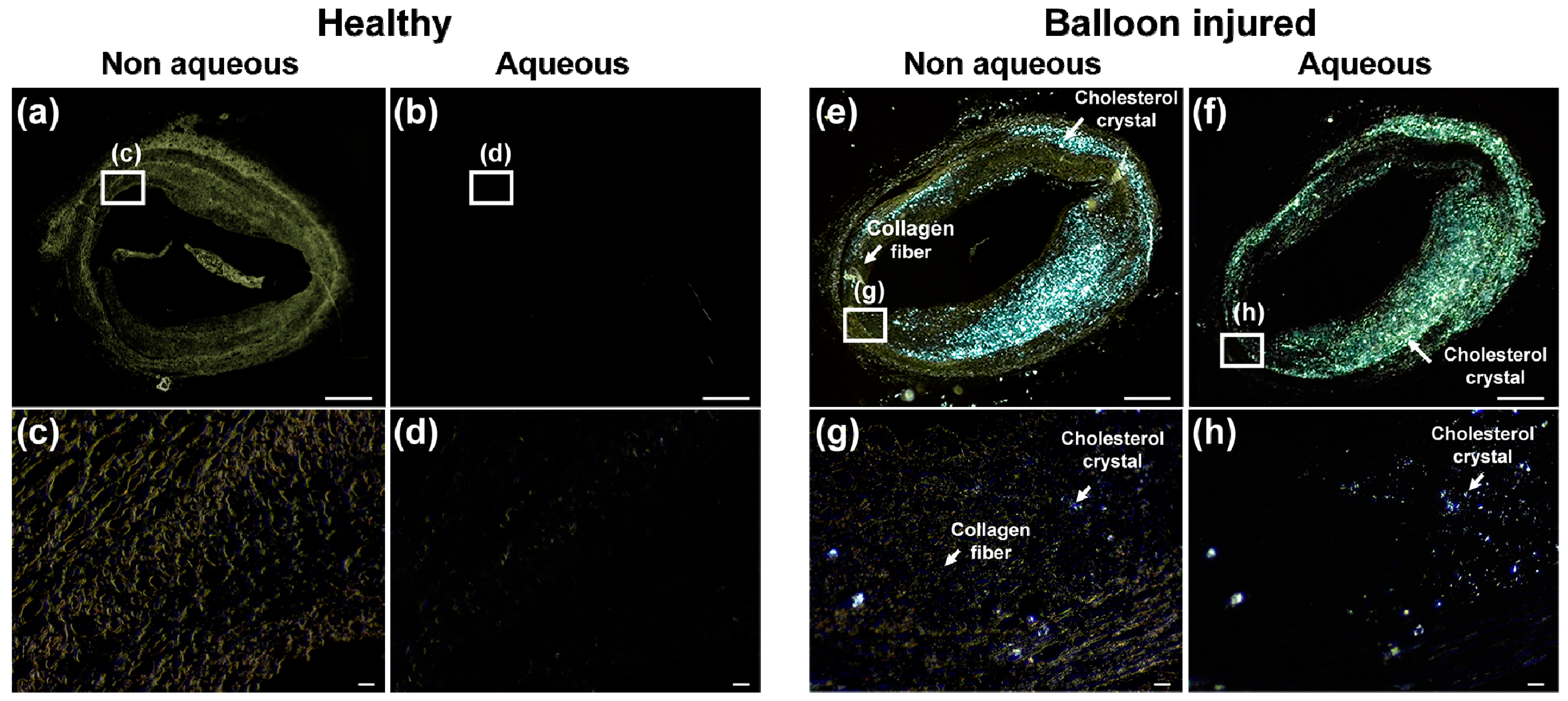
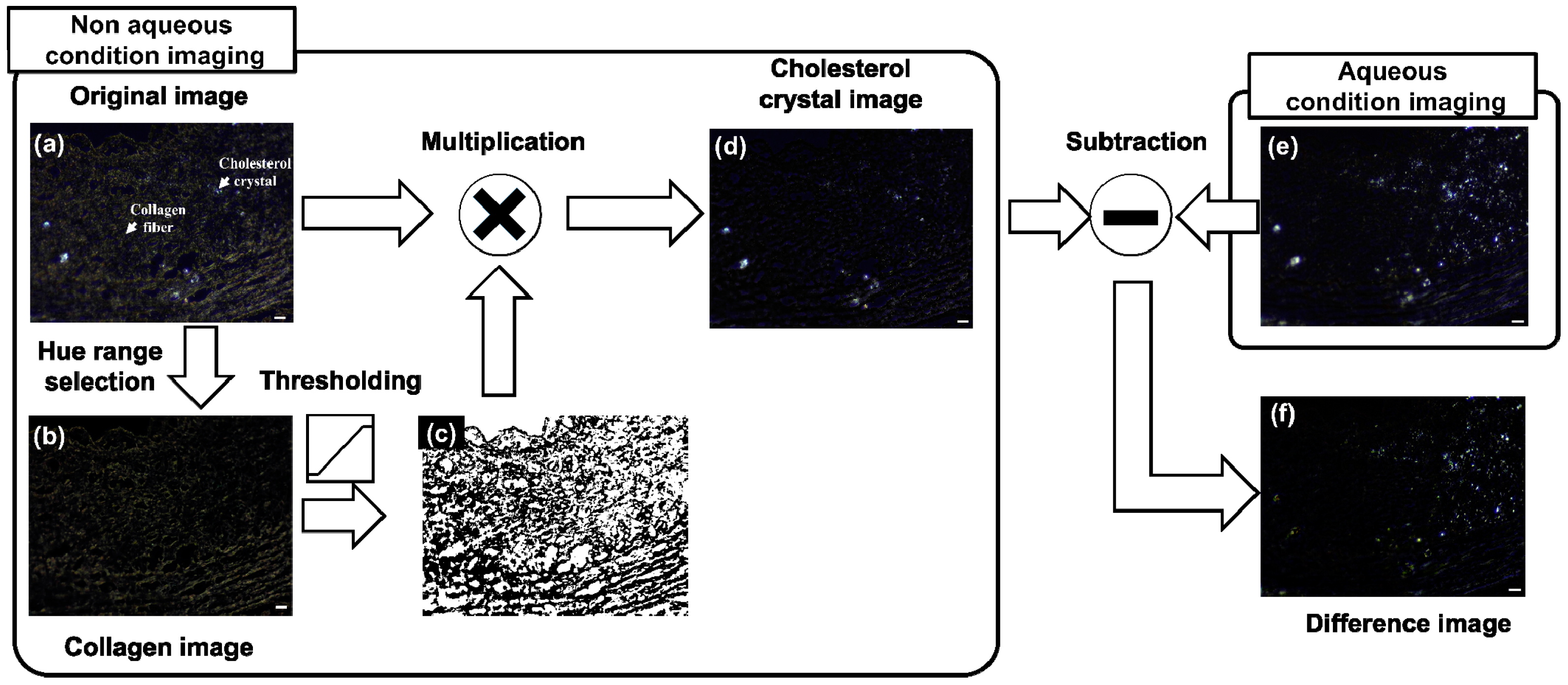
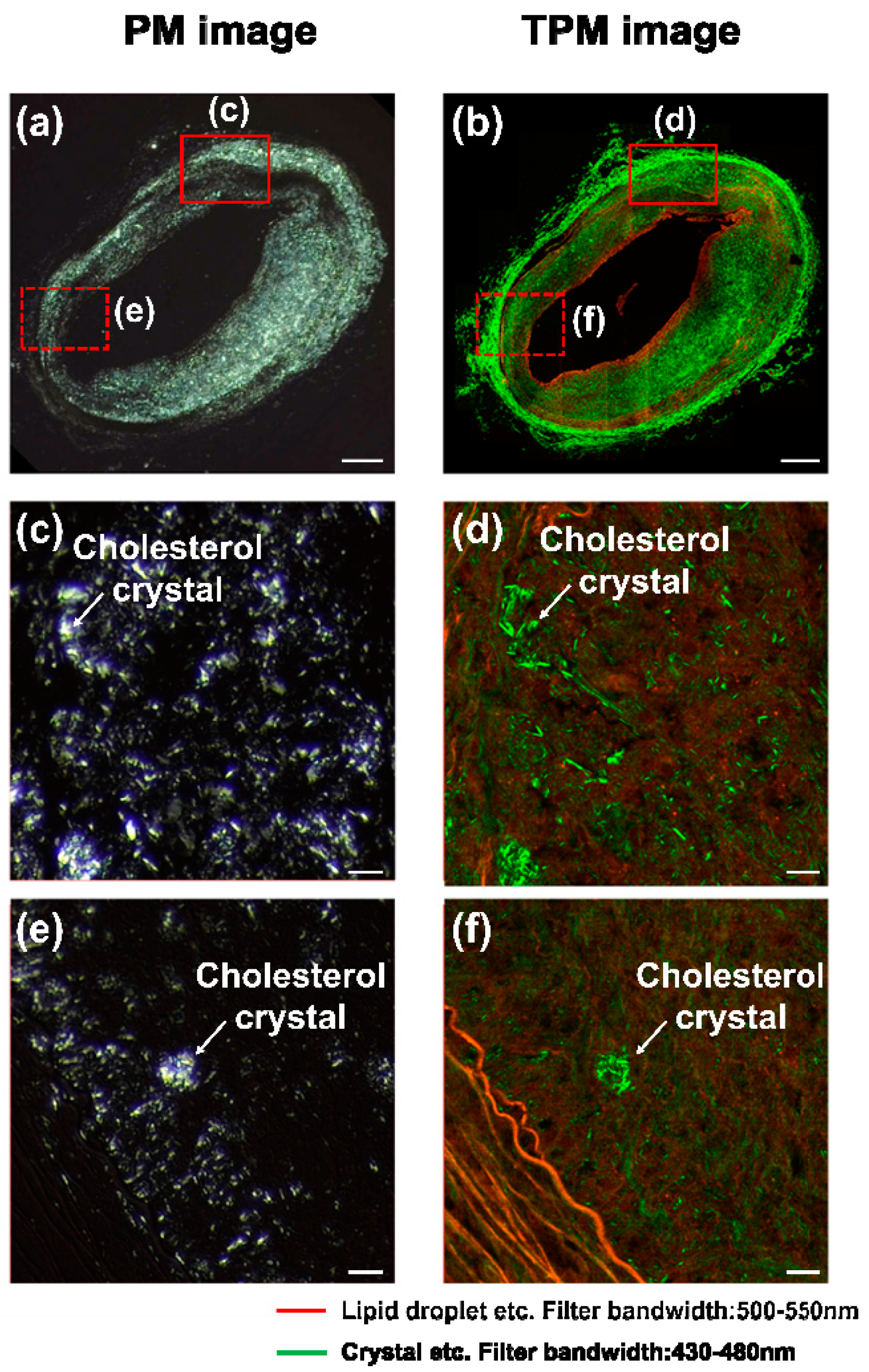
3.1. Cholesterol Crystal Detection
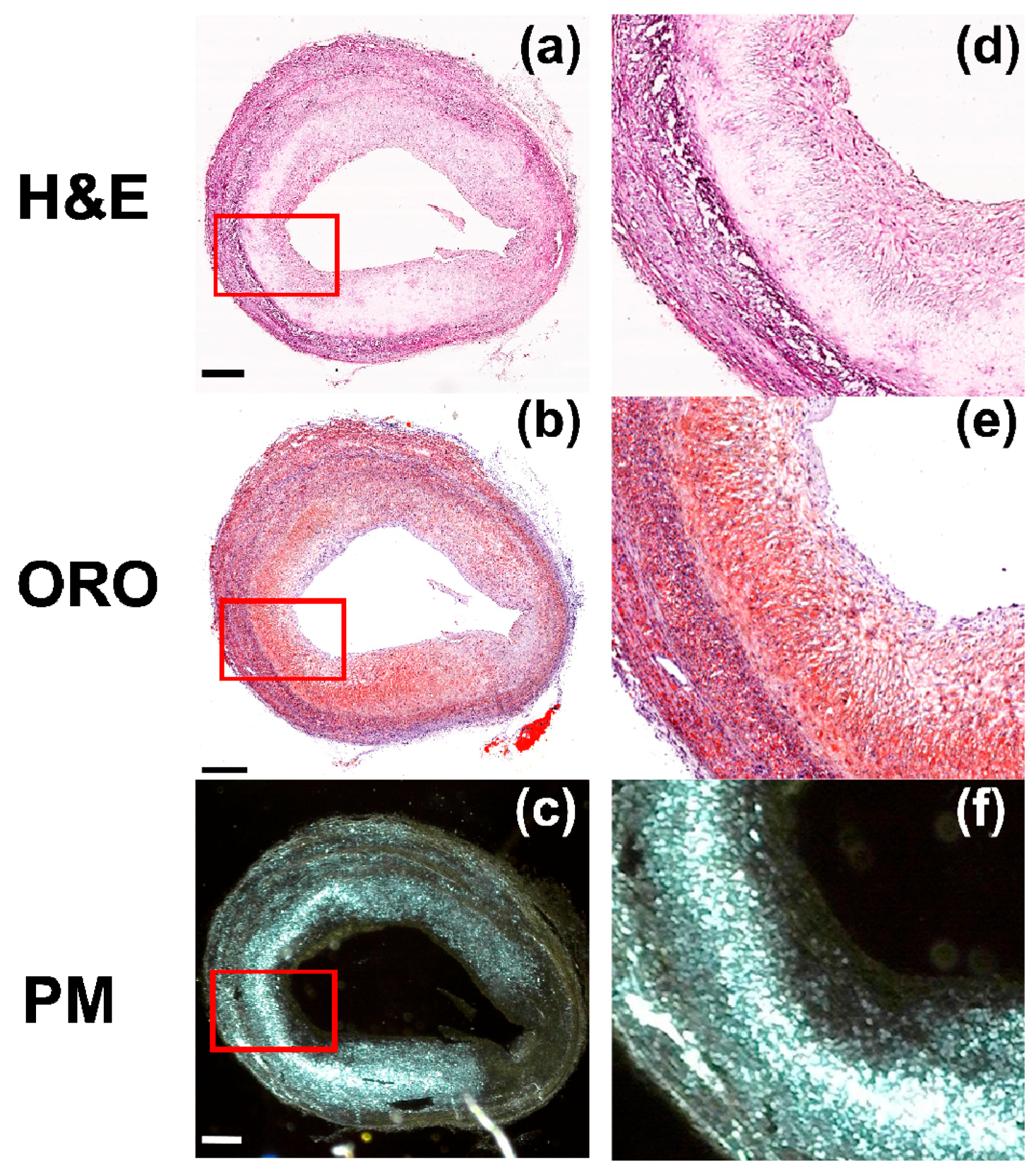
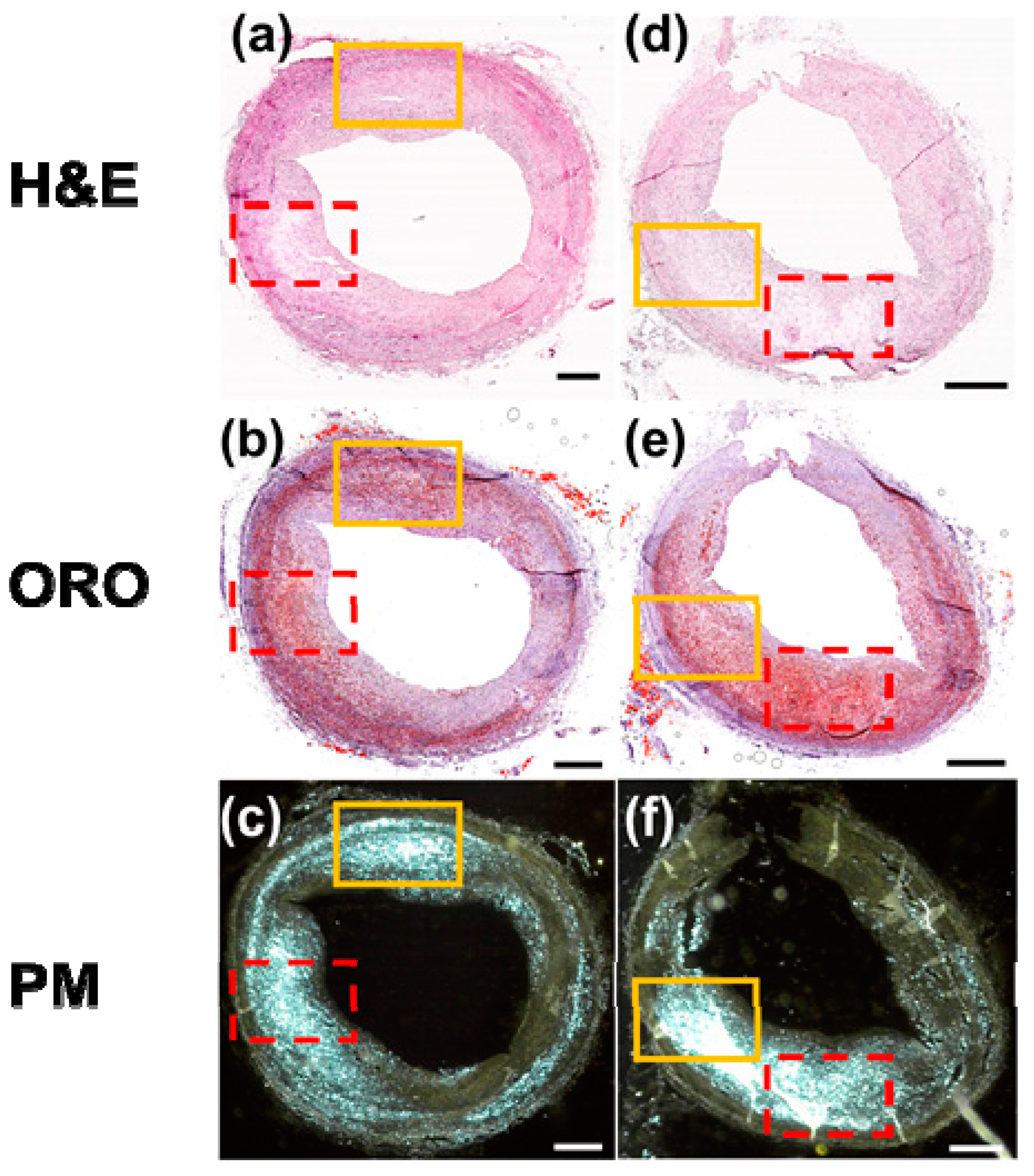
3.2. Comparison with Conventional Histological Methods
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kumar, V.; Abbas, A.K.; Fausto, N.; Aster, J.C. Robbins and Cotran Pathologic Basis of Disease, Professional Edition E-Book; Elsevier Health Sciences: Berlin, Germany, 2014. [Google Scholar]
- Finn, A.V.; Nakano, M.; Narula, J.; Kolodgie, F.D.; Virmani, R. Concept of vulnerable/unstable plaque. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from sudden coronary death. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- Duewell, P.; Kono, H.; Rayner, K.J.; Sirois, C.M.; Vladimer, G.; Bauernfeind, F.G.; Abela, G.S.; Franchi, L.; Nunez, G.; Schnurr, M. NLRP3 inflamasomes are required for atherogenesis and activated by cholesterol crystals that form early in disease. Nature 2010, 464, 1357–1361. [Google Scholar] [CrossRef] [PubMed]
- Grebe, A.; Latz, E. Cholesterol crystals and inflammation. Curr. Rheumatol. Rep. 2013, 15, 313. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Zhou, B.; Hsiai, T.K.; Shung, K.K. A Review of Intravascular Ultrasound-Based Multimodal Intravascular Imaging: The Synergistic Approach to Characterizing Vulnerable Plaques. Ultrason. Imaging 2016, 38, 314–331. [Google Scholar] [CrossRef] [PubMed]
- Arbab-Zadeh, A.; Fuster, V. The Myth of “The Vulnerable Plaque”: Transitioning from a Focus on Individual Lesions to Atherosclerotic Disease Burden for Coronary Artery Disease Risk Assessment. J. Am. Coll. Cardiol. 2015, 65, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Frink, R.J. Parallel cholesterol crystals: A sign of impending plaque rupture? J. Invasive Cardiol. 2010, 22, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Bentzon, J.F.; Otsuka, F.; Virmani, R.; Falk, E. Mechanisms of plaque formation and rupture. Circ. Res. 2014, 114, 1852–1866. [Google Scholar] [CrossRef] [PubMed]
- Janoudi, A.; Shamoun, F.E.; Kalavakunta, J.K.; Abela, G.S. Cholesterol crystal induced arterial inflammation and destabilization of atherosclerotic plaque. Eur. Heart J. 2015, 37, 1959–1967. [Google Scholar] [CrossRef] [PubMed]
- Lilledahl, M.B.; Gustafsson, H.; Ellingsen, P.G.; Zachrisson, H.; Hallbeck, M.; Hagen, V.S.; Kildemo, M.; Lindgren, M. Combined imaging of oxidative stress and microscopic structure reveals new features in human atherosclerotic plaques. J. Biomed. Opt. 2015, 20. [Google Scholar] [CrossRef] [PubMed]
- Wolman, M. Polarized light microscopy as a tool of diagnostic pathology. J. Histochem. Cytochem. 1975, 23, 21–50. [Google Scholar] [CrossRef] [PubMed]
- McCrone, W.C.; McCrone, L.B.; Delly, J.G. Polarized Light Microscopy; Ann Arbor Science Publishers Inc. and McCrone Research Institute: Chicago, IL, USA, 1978. [Google Scholar]
- Freigang, S.; Ampenberger, F.; Spohn, G.; Heer, S.; Shamshiev, A.T.; Kisielow, J.; Hersberger, M.; Yamamoto, M.; Bachmann, M.F.; Kopf, M. NRF2 is essential for cholesterol crystal-induced inflammasome activation and exacerbation of atherosclerosis. Eur. J. Immunol. 2011, 41, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Suhalim, J.L.; Chung, C.-Y.; Lilledahl, M.B.; Lim, R.S.; Levi, M.; Tromberg, B.J.; Potma, E.O. Characterization of cholesterol crystals in atherosclerotic plaques using stimulated Raman scattering and second-harmonic generation microscopy. Biophys. J. 2012, 102, 1988–1995. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Li, J.; Wang, P.; Hu, C.R.; Zhang, D.; Sturek, M.; Cheng, J.X. Label-Free Quantitative Imaging of Cholesterol in Intact Tissues by Hyperspectral Stimulated Raman Scattering Microscopy. Angew. Chem. 2013, 125, 13280–13284. [Google Scholar] [CrossRef]
- Gadeela, N.; Rubinstein, J.; Tamhane, U.; Huang, R.; Pathak, D.R.; Hosein, H.-A.; Rich, M.; Dhar, G.; Abela, G.S. The impact of circulating cholesterol crystals on vasomotor function: Implications for no-reflow phenomenon. JACC Cardiovasc. Interv. 2011, 4, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Keijzer, M.; Richards-Kortum, R.R.; Jacques, S.L.; Feld, M.S. Fluorescence spectroscopy of turbid media: Autofluorescence of the human aorta. Appl. Opt. 1989, 28, 4286–4292. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Johnson, L.A.; Liu, S.; Moons, D.S.; Ma, T.; Zhou, Q.; Rice, M.D.; Ni, J.; Wang, X.; Higgins, P.D. Characterizing intestinal inflammation and fibrosis in Crohn’s disease by photoacoustic imaging: Feasibility study. Biomed. Opt. Express 2016, 7, 2837–2848. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Meek, K. Refractive indices of the collagen fibrils and extrafibrillar material of the corneal stroma. Biophys. J. 1997, 72, 1382–1387. [Google Scholar] [CrossRef]
- Masic, A.; Bertinetti, L.; Schuetz, R.; Chang, S.-W.; Metzger, T.H.; Buehler, M.J.; Fratzl, P. Osmotic pressure induced tensile forces in tendon collagen. Nat. Commun. 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Schear, M.J.; Beatty, B.L. A histological investigation into the correlation of central retinal artery atherosclerosis with the systemic circulation. Anat. Rec. 2014, 297, 1430–1434. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhu, C.; Peng, W.; Degnan, A.J.; Chen, L.; Wang, X.; Liu, Q.; Wang, Y.; Xiang, Z.; Teng, Z.; et al. Ex-vivo imaging and plaque type classification of intracranial atherosclerotic plaque using high resolution MRI. Atherosclerosis 2016, 249, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Gardecki, J.A.; Nadkarni, S.K.; Toussaint, J.D.; Yagi, Y.; Bouma, B.E.; Tearney, G.J. Imaging the subcellular structure of human coronary atherosclerosis using micro-optical coherence tomography. Nat. Med. 2011, 17, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Majidi, S.; Sein, J.; Watanabe, M.; Hassan, A.E.; Van de Moortele, P.-F.; Suri, M.F.K.; Clark, H.B.; Qureshi, A.I. Intracranial-Derived Atherosclerosis Assessment: An In Vitro Comparison between Virtual Histology by Intravascular Ultrasonography, 7T MRI, and Histopathologic Findings. Am. J. Neuroradiol. 2013, 34, 2259–2264. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Choi, C.; Ahn, J.; Kim, T.; Park, S.; Park, H.; Kim, J.; Lee, S.; Kang, Y.; Chang, K.; et al. SNR enhancement for catheter based intravascular photoacoustic/ultrasound imaging. In Proceedings of the Photons Plus Ultrasound: Imaging and Sensing 2017, SPIE BiOS, San Francisco, CA, USA, 28 January–2 February 2017; p. 6. [Google Scholar]
- Li, X.; Bayliss, G.; Zhuang, S. Cholesterol Crystal Embolism and Chronic Kidney Disease. Int. J. Mol. Sci. 2017, 18, 1120. [Google Scholar] [CrossRef] [PubMed]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, S.; Kim, K.; Kim, T.; Park, H.; Kim, J.-M.; Lee, S.; Kang, Y.; Chang, K.; Kim, C. High-Contrast Imaging of Cholesterol Crystals in Rabbit Arteries Ex Vivo Using LED-Based Polarization Microscopy. Sensors 2018, 18, 1258. https://doi.org/10.3390/s18041258
Cho S, Kim K, Kim T, Park H, Kim J-M, Lee S, Kang Y, Chang K, Kim C. High-Contrast Imaging of Cholesterol Crystals in Rabbit Arteries Ex Vivo Using LED-Based Polarization Microscopy. Sensors. 2018; 18(4):1258. https://doi.org/10.3390/s18041258
Chicago/Turabian StyleCho, Seonghee, Kyungmin Kim, Taehoon Kim, Hyoeun Park, Jin-Moo Kim, SeungHoon Lee, YeonSu Kang, Kiyuk Chang, and Chulhong Kim. 2018. "High-Contrast Imaging of Cholesterol Crystals in Rabbit Arteries Ex Vivo Using LED-Based Polarization Microscopy" Sensors 18, no. 4: 1258. https://doi.org/10.3390/s18041258