Hand Hygiene Teaching Strategies among Nursing Staff: A Systematic Review

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Methods
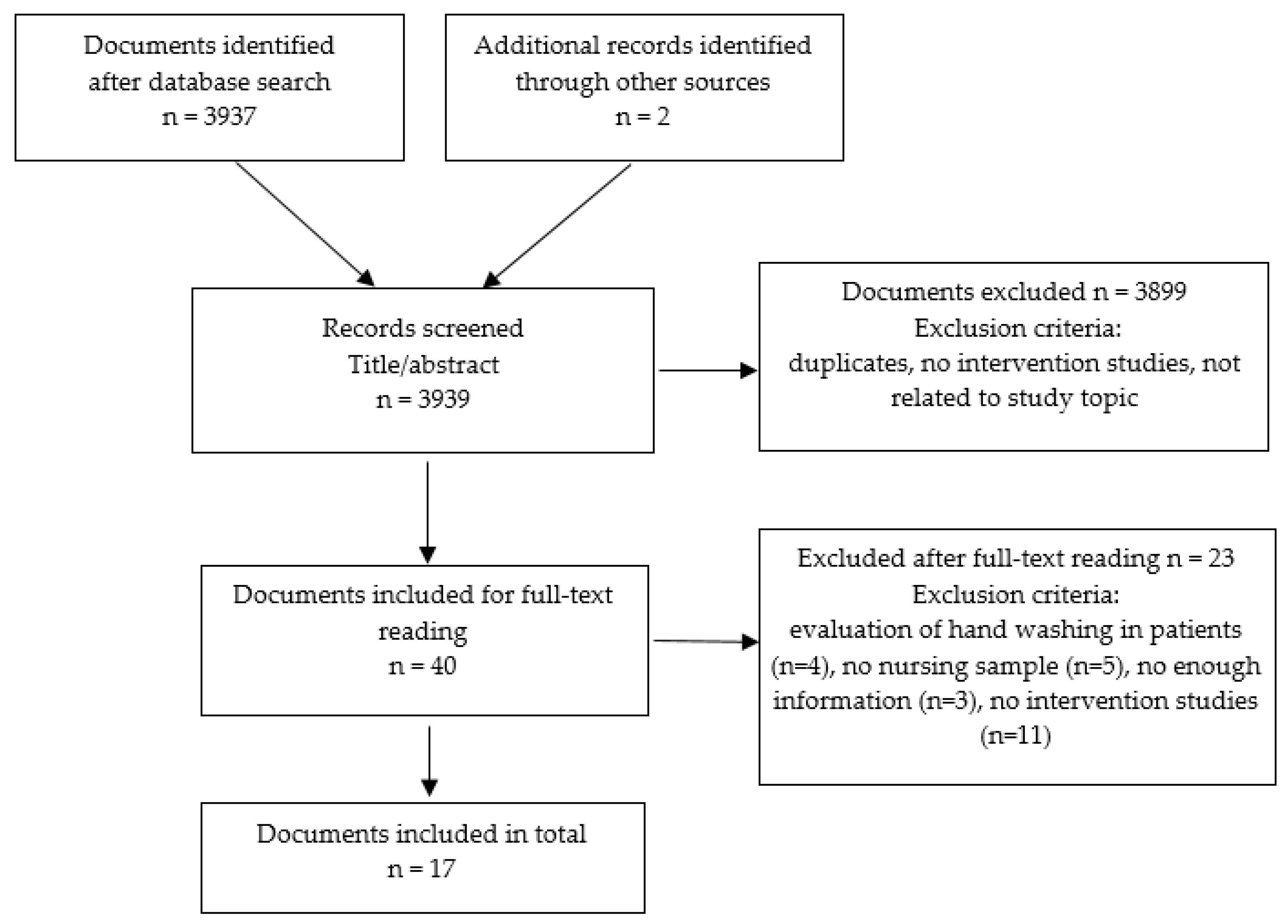
2.1. Search Strategy
2.2. Study Selection, Data Collection, Critical Review, and Level of Evidence
3. Results
3.1. Characteristics of the Clinical Trials
3.2. Educational Strategies of Healthcare Staff in Hand Hygiene
3.3. Effectiveness of Different Methods
3.4. Educational Materials and Feedback Concerning Hand Hygiene
3.5. Prevention-Focused Training
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chraïti, M.N.; Allegranzi, B.; Bagheri Nejad, S.; Kilpatrick, C.; Mathai, E.; Pittet, D. Clean care is safer care: From a global challenge to a WHO patient safety program. BMC Proc. 2011, 5, 260. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. Available online: https://www.who.int/gpsc/5may/tools/9789241597906/en/ (accessed on 1 March 2019).
- Okada, J.; Yamamizu, Y.; Fukai, K. Effectiveness of hand hygiene depends on the patient’s health condition and care environment. Jpn. J. Nurs. Sci. 2016, 13, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Kingston, L.M.; Slevin, B.L.; O’Connell, N.H.; Dunne, C.P. Hand hygiene: Attitudes and practices of nurses, a comparison between 2007 and 2015. Am. J. Infect. Control 2017, 45, 1300–1307. [Google Scholar] [CrossRef]
- Al Kuwaiti, A. Impact of a multicomponent hand hygiene intervention strategy in reducing infection rates at a university hospital in Saudi Arabia. Int. Med. Appl. Sci. 2017, 9, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Smiddy, M.P.; O’Connell, R.; Creedon, S.A. Systematic qualitative literature review of health care workers’ compliance with hand hygiene guidelines. Am. J. Infect. Control 2015, 43, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Taneja, J.; Mishra, B. Promotion of successful hand hygiene practices in the intensive care units of a tertiary care hospital. J. Patient Saf. Infect. Control 2015, 3, 130–133. [Google Scholar] [CrossRef]
- Piras, S.E.; Minnick, A.; Lauderdale, J.; Dietrich, M.S.; Vogus, T.J. The effects of social influence on nurses’ hand hygiene behaviors. J. Nurs. Adm. 2018, 48, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 11, MR000030. [Google Scholar] [CrossRef] [PubMed]
- OCEBM Levels of Evidence Working Group. The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. Available online: http://www.cebm.net/wp-content/uploads/2014/06/CEBMLevels-of-Evidence-2.1.pdf (accessed on 7 June 2019).
- Fisher, D.A.; Seetoh, T.; Oh May-Lin, H.; Viswanathan, S.; Toh, Y.; Yin, W.C.; Siw Eng, L.; Yang, T.S.; Schiefen, S.; Je, M.; et al. Automated measures of hand hygiene compliance among healthcare workers using ultrasound: Validation and a randomized controlled trial. Infect. Control Hosp. Epidemiol. 2013, 34, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.L.; Seto, W.; Wong, L.C.; Wong, T.Y. Effectiveness of multifaceted hand hygiene interventions in long-term care facilities in Hong Kong: A cluster-randomized controlled trial. Infect. Control Hosp. Epidemiol. 2012, 33, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Huis, A.; Holleman, G.; Achterberg, T.; Grol, R.; Schoonhoven, L.; Hulscher, M. Explaining the effects of two different strategies for promoting hand hygiene in hospital nurses: A process evaluation alongside a cluster randomised controlled trial. Implement. Sci. 2013, 8, 41. [Google Scholar] [CrossRef]
- Huis, A.; Schoonhoven, L.; Grol, R.; Donders, R.; Hulscher, M.; Achterberg, T. Impact of a team and leaders-directed strategy to improve nurses’ adherence to hand hygiene guidelines: A cluster randomized trial. Int. J. Nurs. Stud. 2013, 50, 464–474. [Google Scholar] [CrossRef]
- Kukanich, K.S.; Kaur, R.; Freeman, L.C.; Powell, D.A. Evaluation of a hand hygiene campaign in outpatient health care clinics. Am. J. Nurs. 2013, 113, 36–42. [Google Scholar] [CrossRef]
- Martín-Madrazo, C.; Soto-Díaz, S.; Cañada-Dorado, A.; Salinero-Fort, M.A.; Medina-Fernández, M.; Carrillo de Santa Pau, E.; Gómez-Campelo, P.; Abánades-Herranz, J.C. Cluster randomized trial to evaluate the effect of a multimodal hand hygiene improvement strategy in primary care. Infect. Control Hosp. Epidemiol. 2012, 33, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, V.; Giuffre, C.; Villa, S.; Almada, G.; Prasopa-Plizier, N.; Gogna, M.; Gibbons, L.; García Elorrio, E. A multimodal intervention to improve hand hygiene in ICUs in Buenos Aires, Argentina: A stepped wedge trial. Int. J. Qual. Health Care 2015, 27, 405–411. [Google Scholar] [CrossRef]
- Rupp, M.E.; Fitzgerald, T.; Puumala, S.; Anderson, J.R.; Craig, R.; Iwen, P.C.; Jourdan, D.; Keuchel, J.; Marion, N.; Peterson, D.; et al. Prospective, controlled, cords-over trial of alcohol hand gel in critical care units. Infect. Control Hosp. Epidemiol. 2008, 29, 8–15. [Google Scholar] [CrossRef]
- Stewardson, A.; Sax, H.; Gayet-Ageron, A.; Touveneau, S.; Longtin, Y.; Zinng, W.; Pittet, D. Enhanced performance feedback and patient participation improve hand hygiene compliance of healthcare workers in the setting of established multimodal promotion: A single-centre, cluster randomised controlled trial. Lancet Infect. Dis. 2016, 16, 1345–1355. [Google Scholar] [CrossRef]
- von Lengerke, T.V.; Lutze, B.; Krauth, C.; Lange, K.; Stahmeyer, J.T.; Chaberny, I.F. Promoting hand hygiene compliance. Dtsch. Ärztebl. Int. 2017, 114, 29–36. [Google Scholar] [CrossRef]
- Chow, A.; Arah, O.A.; Chan, S.P.; Poh, B.F.; Krishnan, P.; Ng, W.K.; Choudhury, S.; Chan, J.; Ang, B. Alcohol handrubbing and chlorhexidine handwashing protocols for routine hospital practice: A randomized clinical trial of protocol efficacy and time effectiveness. Am. J. Infect. Control 2012, 40, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Xiong, P.; Zhang, J.; Wang, X.; Leong, T.; Hall, B.J. Effects of a mixed media education intervention program on increasing knowledge, attitude, and compliance with standard precautions among nursing students: A randomized controlled trial. Am. J. Infect. Control 2017, 45, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.S.; Dutta, S.; Taneja, N.; Narang, A. Comparing hand hygiene measures in a neonatal ICU: A randomized crossover trial. Indian Pediatr. 2013, 50, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Dulon, M.; Pohrt, U.; Skudlik, C.; Nienhaus, A. Prevention of occupational skin disease: A workplace intervention study in geriatric nurses. Br. J. Dermatol. 2009, 161, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, E.; Boot, C.R.; Van der Gulden, J.W.; Knol, D.L.; Jungbauer, F.H.; Coenraads, P.J.; Anema, J.R. Hands4U: The effects of a multifaceted implementation strategy on hand eczema prevalence in a healthcare setting. Results of a randomized controlled trial. Contact Dermat. 2014, 72, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, J.; Roberts, J.; While, A. The effect of computer-assisted learning versus conventional teaching methods on the acquisition and retention of handwashing theory and skills in pre-qualification nursing students: A randomised controlled trial. Int. J. Nurs. Stud. 2010, 47, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.M.; Syrjälä, H.P.; Ohtonen, P.P.; Meriläinen, M.H.; Kyngäs, H.A.; Ala-Kokko, T.I. Simulation education as a single intervention does not improve hand hygiene practices: A randomized controlled follow-up study. Am. J. Infect. Control 2016, 44, 625–630. [Google Scholar] [CrossRef]
- De Wandel, D.; Maes, L.; Labeau, S.; Vereecken, C.; Blot, S. Behavioral determinants of hand hygiene compliance in intensive care units. Am. J. Crit. Care 2010, 19, 230–239. [Google Scholar] [CrossRef]
- Tromp, M.; Huis, A.; de Guchteneire, I.; van der Meer, J.; van Achterberg, T.; Hulscher, M.; Bleeker-Rovers, C. The short-term and long-term effectiveness of a multidisciplinary hand hygiene improvement program. Am. J. Infect. Control 2012, 40, 732–736. [Google Scholar] [CrossRef]
- Fulbrook, P.; Albarran, J.W.; Baktoft, B.; Sidebottom, B. A survey of European intensive care nurses’ knowledge levels. Int. J. Nurs. Stud. 2012, 49, 191–200. [Google Scholar] [CrossRef]
- Katherason, S.G.; Naing, L.; Jaalam, K.; Nik Mohamad, N.A.; Bhojwani, K.; Harussani, N.D.; Ismail, A. Hand decontamination practices and the appropriate use of gloves in two adult intensive care units in Malaysia. J. Infect. Dev. Ctries. 2010, 4, 118–123. [Google Scholar] [CrossRef]
- Kritsotakis, E.I.; Astrinaki, E.; Messaritaki, A.; Gikas, A. Implementation of multimodal infection control and hand hygiene strategies in acute-care hospitals in Greece: A cross-sectional benchmarking survey. Am. J. Infect. Control 2018, 46, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Coyne, E.; Rands, H.; Frommolt, V.; Kain, V.; Plugge, M.; Mitchell, M. Investigation of blended learning video resources to teach health students clinical skills: An integrative review. Nurse Educ. Today 2018, 63, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Therattil, P.J.; Yueh, J.H.; Kordahi, A.M.; Cherla, D.V.; Lee, E.S.; Granick, M.S. Randomized controlled trial of antiseptic hand hygiene methods in an outpatient surgery clinic. Wounds 2015, 27, 347–353. [Google Scholar] [PubMed]
- Weber, U.; Constantinescu, M.; Woermann, U.; Schmitz, F.; Schnabel, K. Video-based instruction for surgical hand disinfection as a replacement for conventional tuition? A randomized, blind comparative study. GMS J. Med. Educ. 2016, 33, Doc57. [Google Scholar] [CrossRef] [PubMed]
- Price, L.; Melone, L.; McLarnon, N.; Bunyan, D.; Kilpatrick, C.; Flowers, P.; Reilly, J. A systematic review to evaluate the evidence base for the World Health Organization’s adopted hand hygiene technique for reducing the microbial load on the hands of healthcare workers. Am. J. Infect. Control 2018, 46, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Schiffers, H.; Zaatreh, S.; Mittelmeier, W.; Bader, R. Examination of cross contamination risks between hospitals by external medical staff via cross-sectional intercept survey of hand hygiene. GMS Hyg. Infect. Control 2014, 9, Doc11. [Google Scholar] [CrossRef] [PubMed]
- Álvarez Lerma, F.; Sánchez García, M.; Lorente, L.; Gordo, F.; Añón, J.M.; Álvarez, J.; Palomar, M.; García, R.; Arias, S.; Vázquez-Calatayud, M.; et al. Guidelines for the prevention of ventilator-associated pneumonia and their implementation. The Spanish “Zero-VAP” bundle. Med. Intensiv. 2014, 38, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, J.; Yeager, M.P.; Beach, M.; Patel, H.M.; Huysman, B.C.; Loftus, R.W. Video observations to map hand contact and bacterial transmission in operating rooms. Am. J. Infect. Control 2014, 42, 698–701. [Google Scholar] [CrossRef]
- Sendall, M.C.; McCosker, L.K.; Halton, K. Cleaning Staff’s Attitudes about Hand Hygiene in a Metropolitan Hospital in Australia: A Qualitative Study. Int. J. Environ. Res. Public Health 2019, 16, 1067. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe-Petitte, D.M.; Van de Mortel, T.; Nasirudeen, A.M.A. A systematic review on hand hygiene knowledge and compliance in student nurses. Int. Nurs. Rev. 2018, 65, 336–348. [Google Scholar] [CrossRef]
- Le, C.D.; Lehman, E.B.; Nguyen, T.H.; Craig, T.J. Hand Hygiene Compliance Study at a Large Central Hospital in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 607. [Google Scholar] [CrossRef]
- Lien, L.T.Q.; Johansson, E.; Lan, P.T.; Chuc, N.T.K.; Thoa, N.T.M.; Hoa, N.Q.; Phuc, H.D.; Tamhankar, A.J.; Lundborg, C.S. A Potential Way to Decrease the Know-Do Gap in Hospital Infection Control in Vietnam: “Providing Specific Figures on Healthcare-Associated Infections to the Hospital Staff Can ‘Wake Them Up’ to Change Their Behaviour”. Int. J. Environ. Res. Public Health 2018, 15, 1549. [Google Scholar] [CrossRef]
- Bauer, A.; Rönsch, H.; Elsner, P.; Dittmar, D.; Bennett, C.; Schuttelaar, M.A.; Lukács, J.; John, S.; Williams, H.C. Interventions for preventing occupational irritant hand dermatitis. Cochrane Database Syst. Rev. 2018, 4, CD004414. [Google Scholar] [CrossRef]
- Rosiński, J.; Różańska, A.; Jarynowski, A.; Wójkowska-Mach, J. Factors Shaping Attitudes of Medical Staff towards Acceptance of the Standard Precautions. Int. J. Environ. Res. Public Health 2019, 16, 1050. [Google Scholar] [CrossRef]
- Jeffries, P.R. Computer versus lecture: A comparison of two methods of teaching oral medication administration in a nursing skills laboratory. J. Nurs. Educ. 2001, 40, 323–329. [Google Scholar] [PubMed]
- Al-Khawaldeh, O.A.; Al-Hussami, M.; Darawad, M. Influence of nursing students handwashing knowledge, beliefs, and attitudes on their handwashing compliance. Health 2015, 7, 572–579. [Google Scholar] [CrossRef]
- Kingston, L.M.; O’Connell, N.H.; Dunne, C.P. Survey of attitudes and practices of Irish nursing students towards hand hygiene, including handrubbing with alcohol-based hand rub. Nurse Educ. Today 2017, 52, 57–62. [Google Scholar] [CrossRef]
- Lewis, M.J.; Davies, R.; Jenkins, D.; Tait, M.I. A review of evaluative studies of computer-based learning in nursing education. Nurse Educ. Today 2001, 21, 26–37. [Google Scholar] [CrossRef]
- Jeffries, P.R.; Rew, S.; Cramer, J.M. A comparison of student-centred versus traditional methods for teaching basic nursing skills in a learning laboratory. Nurs. Educ. Perspect. 2002, 23, 14–19. [Google Scholar]
- Konicki, T.; Miller, E. Use of a simulation intervention to examine differences in nursing students’ hand hygiene knowledge, beliefs, and behaviors. Nurse Educ. Today 2016, 45, 96–101. [Google Scholar] [CrossRef]
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N.; Wensing, M.; Fiander, M.; Eccles, M.P.; et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. 2015, 4, CD005470. [Google Scholar] [CrossRef] [PubMed]
- von Lengerke, T.; Ebadi, E.; Schock, B.; Krauth, C.; Lange, K.; Stahmeyer, J.T.; Chaberny, I.F. Impact of psychologically tailored hand hygiene interventions on nosocomial infections with multidrug-resistant organisms: Results of the cluster-randomized controlled trial PSYGIENE. Antimicrob. Resistance Infect. Control 2019, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Mauger, B.; Marbella, A.; Pines, E.; Chopra, R.; Black, E.R.; Aronson, N. Implementing quality improvement strategies to reduce healthcare-associated infections: A systematic review. Am. J. Infect. Control 2014, 42, S274–S283. [Google Scholar] [CrossRef] [PubMed]
- Caris, M.G.; Kamphuis, P.G.A.; Dekker, M.; De Bruijne, M.C.; Van Agtmael, M.A.; Vandenbroucke-Grauls, C.M.J.E. Patient safety culture and the ability to improve: A proof of concept study on hand hygiene. Infect. Control Hosp. Epidemiol. 2017, 38, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Wikström, E.; Dellenborg, L.; Wallin, L.; Gillespie, B.M.; Erichsen Andersson, A. The Safe Hands Study: Implementing aseptic techniques in the operating room: Facilitating mechanisms for contextual negotiation and collective action. Am. J. Infect. Control 2018, 47, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Vargas, C.; Cañadas-De la Fuente, G.A.; Aguayo, R.; Fernández-Castillo, R.; De la Fuente, E.I. Which occupational risk factors are associated with burnout in nursing? A meta-analytic study. Int. J. Clin. Health Psychol. 2014, 14, 28–38. [Google Scholar] [CrossRef]


{kind=link}
| Author, Country, (Year) | Design | Interventions | Sample | Hand Hygiene Compliance | Main Results | LE/GR |
|---|---|---|---|---|---|---|
| Educational strategies | ||||||
| Fisher et al., Singapore, (2013) [12] | Randomized controlled trial | HH compliance using ultrasound + audio reminders | n = 72 ICU nurses | - | Higher HH compliance after intervention of 6.8% (95% CI, 2.5–9.5) | 1a/A |
| Ho et al., China, (2012) [13] | Randomized controlled trial by groups | CG: reception of intervention package (posters, talks, hydroalcoholic solution)IG 1: same + glove pack slightlypowderedIG 2: same + powderless gloves | n = 612 geriatric nurses CG n = 189 IG1 n = 180 IG2 n = 243 | CG = 19.5% IG1 = 27% IG2 = 22% | Increase in HH compliance 1 month/4 months after interventionCG = 19.8%/21.6% IG1 = 59.2%/60.6% IG2 = 59.9%/48.6% | 1a/A |
| Huis et al., Netherlands, (2013a) [14] | Randomized controlled trial | Adherence to two improvement strategies of HH Group led by leaders (GLD) (classic education) State-of-the-art strategy group (SASG): education, reminders, feedback, facilities and products, establishment of norms and objectives, social influence, and leadership | n = 67 nurses GLD: n = 20 SASG: n = 47 | GLD: 19.1% SASG: 21.8% | Increase of HH adherence through social influence and enhanced leadership in HH improvement strategies Postintervention/follow-up (at 6 months): GLD: 34%/33% SASG: 18.6%/24.1% | 1a/A |
| Huis et al., Netherlands, (2013b) [15] | Randomized controlled trial by groups | Strategy of HH compliance that was leader-directed CG: education, reminders, feedback, and orientation (led by leaders) IG: same as the last group + social influence and leadership (state-of-the-art wards) | n = 914 nurses, 67 wards CG: n = 402 IG: n = 512 | CG: 20% IG: 22% | HH compliance rates improved from 22% (just before implementing strategies) to 47% (after the intervention) and to 48% (six months after). The vanguard group improved from 23% to 42% in the short term and 46% in the long term. Compliance in CG increased from 20% to 53% (short term) and remained at 53% in the long term | 1a/A |
| Kukanich et al., United States, (2013) [16] | Randomized controlled trial | Improved HH in two outpatient healthcare clinics Outpatient clinic oncology (G1) Gastrointestinal specialist outpatient clinic (G2)Disinfectant gel and informational signs were introduced together as an intervention | n = 56 nurses G1: n = 41 G2: n = 15 | G1: 11% G2: 21% | The frequency of HH improved significantly after intervention G1: 36% G2: 54% | 1a/A |
| Martín-Madrazo et al., Spain, (2012) [17] | Cluster randomized controlled trial | 5MHH to evaluate HH CG: - IG: training of HWs through teaching sessions, the implementation of hydroalcoholic preparations, and the installation of reminder posters | n = 198 nurses CG n = 99 IG n = 99 | Overall baseline compliance level: 8.1% Increased adherence to HH: 21.6% At 6 months: CG: 3.6%IG: 16.1% | 1a/A | |
| Rodríguez et al., Argentina, (2015) [18] | Conglomerate randomized controlled trial | Improving HWs compliance with HH Shipping one time per month of an intervention: (i) leadership commitment, (ii) surveillance of materials necessary to comply with hand hygiene and alcohol consumption, (iii) use of reminders, (iv) a screenplay of the project, and (v) feedback | n = 468 ICU nurses | 50% | A multimodal strategy was effective for HH compliance Handwashing after interventions was 70% | 1a/A |
| Rupp et al., United States, (2008) [19] | Randomized clinical trial | Adherence in the use of alcohol-based hand gel Unit A: educational program, reminders of handwashing, and leaflets with questionnaires. After 12 months, introduction of hydroalcoholic gel Unit B: installation of hydroalcoholic solution containers inside and outside of each patient care room | n = 174 ICU nurses | Unit A: 47% Unit B: 38% | Increase in the use of alcohol-based hand gel at 31% in both units Unit A: ● After the educational program: 62% ● With hand gel available: 66% Unit B: ● Hand gel available: 74% | 1a/A |
| Stewardson et al., Switzerland, (2016) [20] | Conglomerate randomized controlled trial | Control group (G1): observation of participants Improved performance feedback group (G2): observation + feedback (verbal comments, reminder of 5MHH) Improved performance feedback and participation group (G3): observation + feedback + reports and posters every 3 months | n = 67 nurses G1 = 21 G2 = 24 G3 = 22 | G1: 66% G2: 65% G3: 66% | HH compliance increase from 65% to 77% G1: 73% G2: 75% G3: 77% Effect of the intervention: G1 = OR, 1.41 CI (1.21–1.63) G2 = OR, 1.61 CI (1.41–1.84) G3 = OR, 1.73 CI (1.51–1.98) | 1a/A |
| von Lengerke et al., Germany, (2017) [21] | Randomized controlled trial | CG: training measures on “clean hands action” (adaptation of World Health Organization’s (WHO’s) “Cleaner Care Is Safer Care” program) IG: application of 29 patterns of behavior change | n = 572 ICU nurses CG: n = 367 IG: n = 205 | CG: 55% IG: 54% (compliance with HH in 2013) | Increased adherence to HH through behavioral interventions in 2013 vs 2015 CG: +9% (95% CI, 5.1–11.8) IG: +16% (95% CI, 11.9–18.9) | 1a/A |
| Xiong et al., China, (2017) [22] | Randomized controlled trial | CG: self-directed readings IG: education sessions, with lectures, videos, role play + 15–20 min of individual online supervision and feedback sessions after each class | n = 84 nursing students (n = 42 in each group) | The level of knowledge about HH increased by 15% in the intervention group | 1a/A | |
| Effectiveness of Different Methods | ||||||
| Chow et al., Singapore, (2012) [23] | Randomized controlled trial | Compared the effectiveness of 3 HH protocols Protocol 1 (P1): hand rubbing with alcohol covering all hand surfaces in no particular order Protocol 2 (P2): manual scraping with alcohol using the standard seven-step technique Protocol 3 (P3): washing hands with chlorhexidine using the standard seven-step technique | n = 60 nurses | In terms of daily care, alcohol hand rubbing covering all hand surfaces was the most effective intervention The effectiveness of the three interventions was shown to be equally effective Time spent on chlorhexidine HH was 79.7 s vs alcohol HH at 26 s | 1a/A | |
| Sharma et al., India, (2013) [24] | Randomized controlled trial | Comparison of 3 HH methods ● Group hand washing soap (G1) ● Alcohol solution group (G2) ● Povidone iodine group (G3) | n = 105 NICU nurses | Povidone–iodine scrub and alcohol hand rubbing were superior to plain soap hand washing In the groups using alcoholic solution and povidone, the measurement of colony-forming units was lower than in the group using soap. Mean reduction was 38.6%. | 1a/A | |
| Prevention-Focused Training | ||||||
| Dulon et al., Germany, (2009) [25] | Randomized controlled trial | Increase protective behavior through a skincare program reducing skin disease CG: training seminar IG: training seminar + advice on interventions and protection of the skin by instructors | n = 388 geriatric nurses CG: n = 242IG: n = 146 | CG: 19% IG: 26% | No differences between groups in work behavior (prevalence post-intervention= 17% in both groups). In IG, increase in the use of moisturizers and hand disinfection instead of hand washing. | 1a/A |
| Van der Meer et al., Netherlands, (2014) [26] | Randomized controlled trial | Effects of a multifaceted implementation strategy on behavior, behavioral determinants, knowledge, and awareness of HWs regarding the use of recommendations to prevent hand eczema CG: only brochure IG: education, participatory work groups, and role models | n = 1649 nurses CG: n = 773 IG: n = 876 | CG: 10.3% IG: 7.3% | IG group was significantly more likely to report hand eczema CG: 9.7% IG: 11.3% The intervention had a positive effect on the frequency of HH, the use of a moisturizer, and wearing cotton gloves | 1a/A |
| Training with Audiovisual Media | ||||||
| Bloomfield et al., UK, (2010) [27] | Randomized controlled trial | Effects of a computer-assisted learning module (IG) vs conventional face-to-face classroom teaching (CG) | n = 231 nursing students CG: n = 113 IG: n = 118 | - | Computer-assisted learning was effective in teaching both the theory and the skill of knowledge of hand washing | 1a/A |
| Jansson et al., Finland, (2016) [28] | Randomized controlled trial follow-up study | Four phases: (1) Simulation; (2) Orientation to mannequin capabilities; (3) Practical scenario; (4) Post-scenario debriefing session. | n = 30 ICU nurses IG: n = 15 CG: n = 15 | IG = 40.8% | HH adherence in IG increased to 59.2% (6 months after the intervention) and decreased to 50.8% (24 months after) | 1a/A |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martos-Cabrera, M.B.; Mota-Romero, E.; Martos-García, R.; Gómez-Urquiza, J.L.; Suleiman-Martos, N.; Albendín-García, L.; Cañadas-De la Fuente, G.A. Hand Hygiene Teaching Strategies among Nursing Staff: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 3039. https://doi.org/10.3390/ijerph16173039
Martos-Cabrera MB, Mota-Romero E, Martos-García R, Gómez-Urquiza JL, Suleiman-Martos N, Albendín-García L, Cañadas-De la Fuente GA. Hand Hygiene Teaching Strategies among Nursing Staff: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(17):3039. https://doi.org/10.3390/ijerph16173039
Chicago/Turabian StyleMartos-Cabrera, María B., Emilio Mota-Romero, Raúl Martos-García, José L. Gómez-Urquiza, Nora Suleiman-Martos, Luis Albendín-García, and Guillermo A. Cañadas-De la Fuente. 2019. "Hand Hygiene Teaching Strategies among Nursing Staff: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 17: 3039. https://doi.org/10.3390/ijerph16173039