The Current Research Landscape of the Application of Artificial Intelligence in Managing Cerebrovascular and Heart Diseases: A Bibliometric and Content Analysis

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
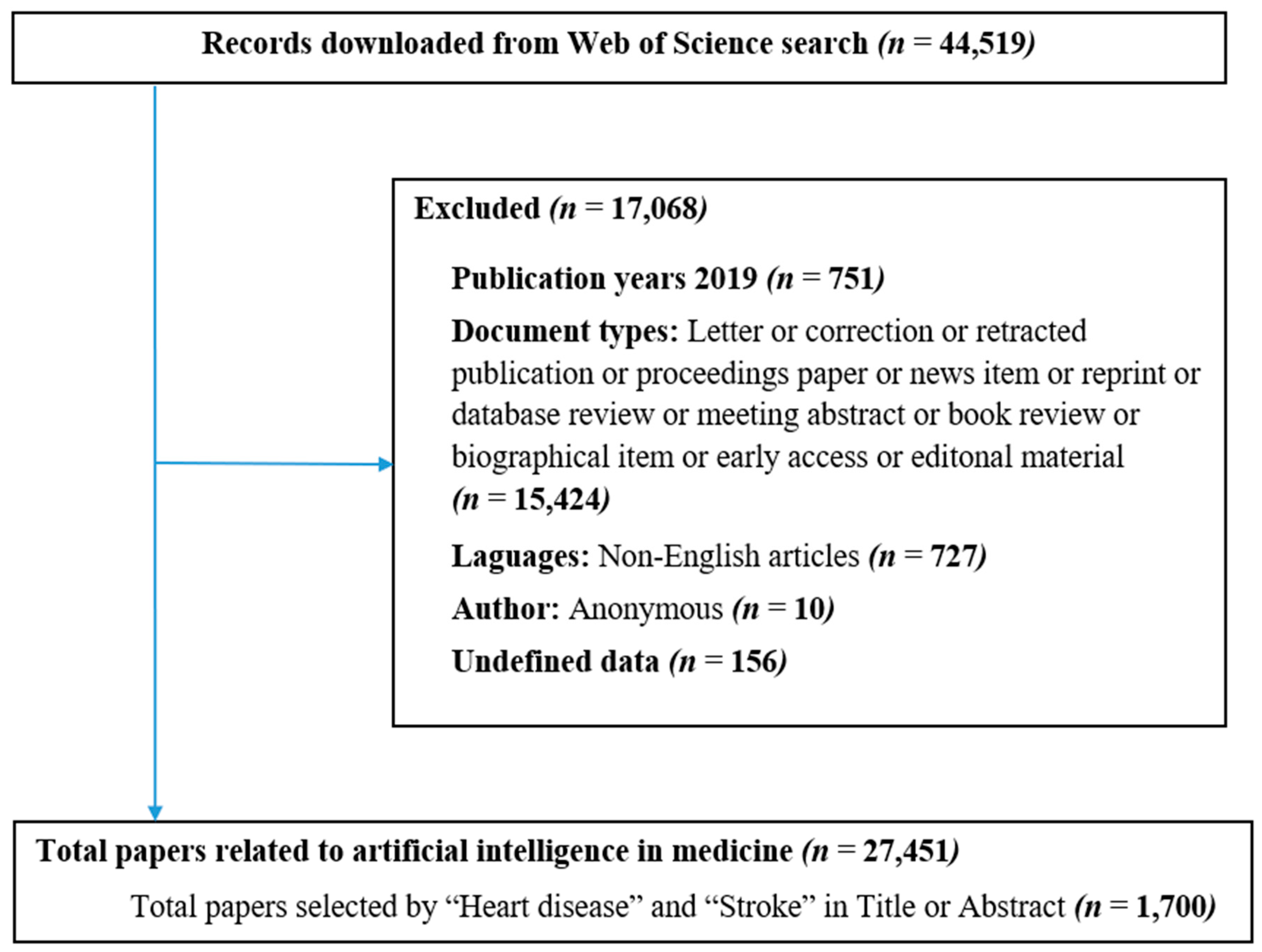
2.1. Search Strategy
2.2. Data Extraction
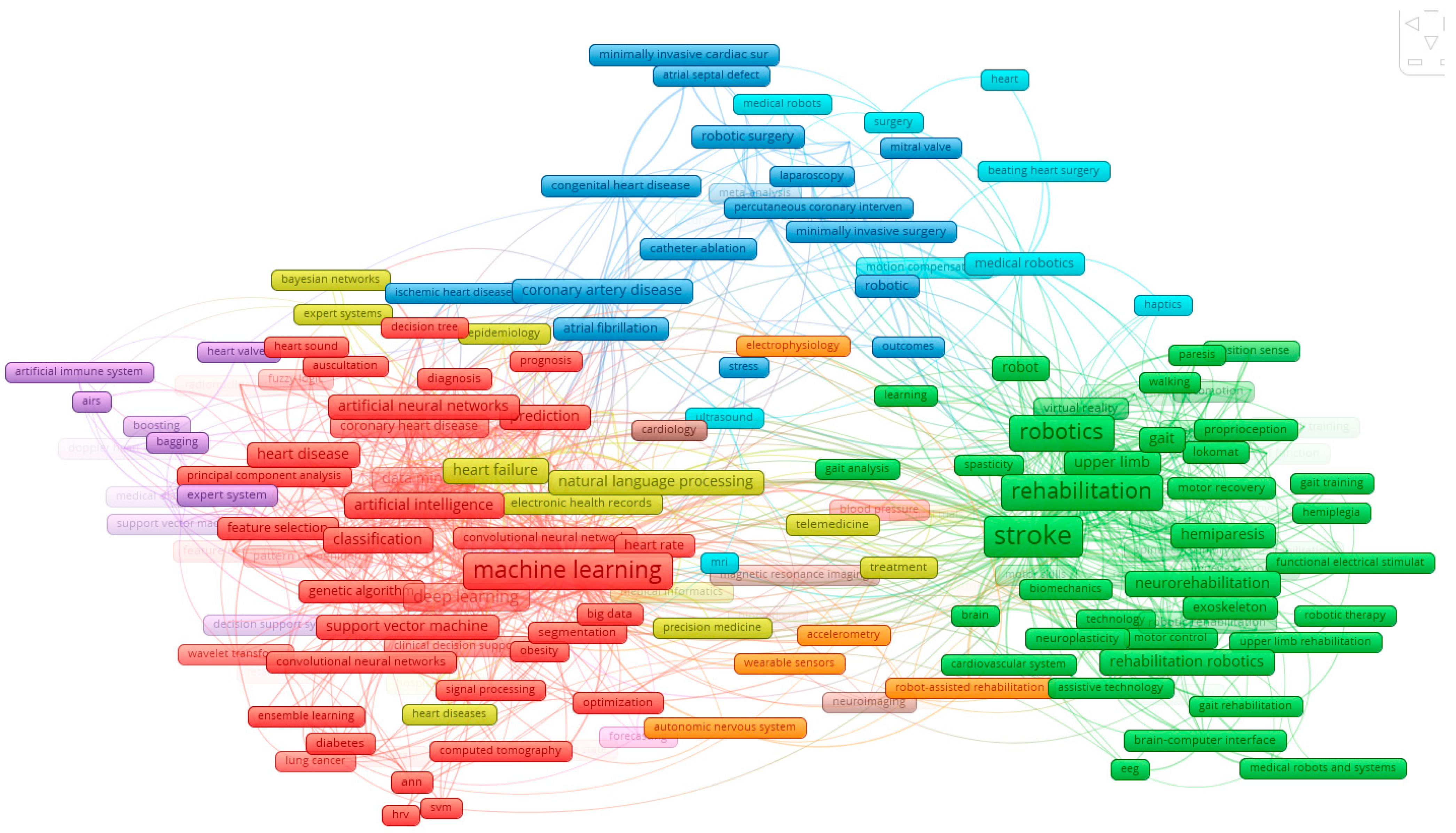
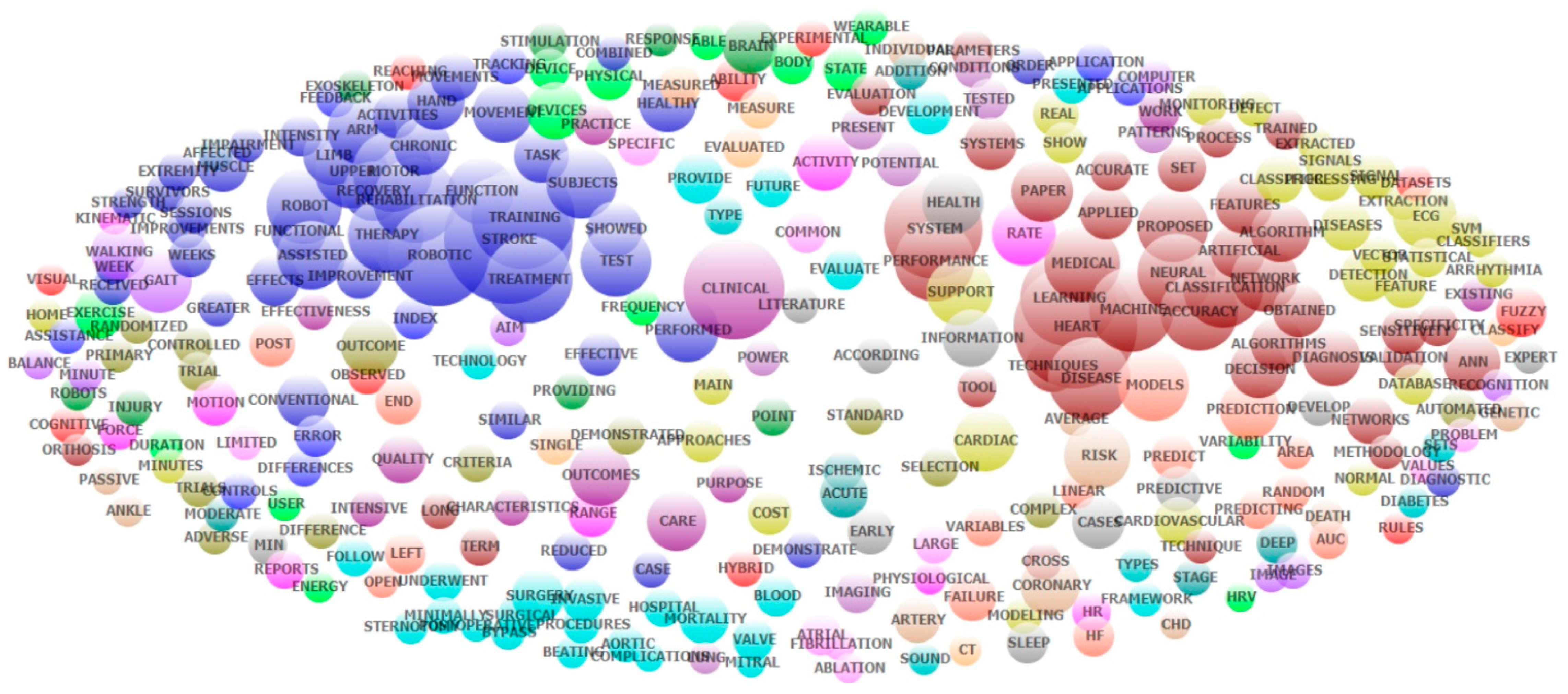
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). Available online: www.who.int/cardiovascular_diseases/en/ (accessed on 26 July 2019).
- GBD 2017 DALYs; HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Tran, B.X.; Vu, G.T.; Ha, G.H.; Vuong, Q.H.; Ho, M.T.; Vuong, T.T.; La, V.P.; Ho, M.T.; Nghiem, K.P.; Nguyen, H.L.T.; et al. Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study. J. Clin. Med. 2019, 8, 360. [Google Scholar] [CrossRef]
- Bom, M.J.; Levin, E.; Driessen, R.S.; Danad, I.; Van Kuijk, C.C.; van Rossum, A.C.; Narula, J.; Min, J.K.; Leipsic, J.A.; Belo Pereira, J.P.; et al. Predictive value of targeted proteomics for coronary plaque morphology in patients with suspected coronary artery disease. EBioMedicine 2019, 39, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Alawieh, A.; Zaraket, F.; Alawieh, M.B.; Chatterjee, A.R.; Spiotta, A. Using machine learning to optimize selection of elderly patients for endovascular thrombectomy. J. NeuroInterv. Surg. 2019, 11, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Wan, T.; Feng, H.; Tong, C.; Li, D.; Qin, Z. Automated identification and grading of coronary artery stenoses with X-ray angiography. Comput. Methods Programs Biomed. 2018, 167, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Huang, L.; Lin, Z.; Huang, S.; Chi, Y.; Zhou, J.; Zhang, J.; Tan, R.-S.; Zhong, L. Coronary Artery Segmentation by Deep Learning Neural Networks on Computed Tomographic Coronary Angiographic Images. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 608–611. [Google Scholar]
- Van Hamersvelt, R.W.; Zreik, M.; Voskuil, M.; Viergever, M.A.; Isgum, I.; Leiner, T. Deep learning analysis of left ventricular myocardium in CT angiographic intermediate-degree coronary stenosis improves the diagnostic accuracy for identification of functionally significant stenosis. Eur. Radiol. 2019, 29, 2350–2359. [Google Scholar] [CrossRef]
- Von Knebel Doeberitz, P.L.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; van Assen, M.; Bauer, M.J.; Savage, R.H.; Pannell, J.T.; De Santis, D.; et al. Coronary CT angiography-derived plaque quantification with artificial intelligence CT fractional flow reserve for the identification of lesion-specific ischemia. Eur. Radiol. 2019, 29, 2378–2387. [Google Scholar] [CrossRef] [PubMed]
- Hae, H.; Kang, S.J.; Kim, W.J.; Choi, S.Y.; Lee, J.G.; Bae, Y.; Cho, H.; Yang, D.H.; Kang, J.W.; Lim, T.H.; et al. Machine learning assessment of myocardial ischemia using angiography: Development and retrospective validation. PLoS Med. 2018, 15, e1002693. [Google Scholar] [CrossRef]
- Heo, J.; Yoon, J.G.; Park, H.; Kim, Y.D.; Nam, H.S.; Heo, J.H. Machine Learning–Based Model for Prediction of Outcomes in Acute Stroke. Stroke 2019, 50, 1263–1265. [Google Scholar] [CrossRef]
- Pinto, A.; McKinley, R.; Alves, V.; Wiest, R.; Silva, C.A.; Reyes, M. Stroke Lesion Outcome Prediction Based on MRI Imaging Combined with Clinical Information. Front. Neurol. 2018, 9, 1060. [Google Scholar] [CrossRef]
- Winzeck, S.; Hakim, A.; McKinley, R.; Pinto, J.; Alves, V.; Silva, C.; Pisov, M.; Krivov, E.; Belyaev, M.; Monteiro, M.; et al. ISLES 2016 and 2017-Benchmarking Ischemic Stroke Lesion Outcome Prediction Based on Multispectral MRI. Front. Neurol. 2018, 9, 679. [Google Scholar] [CrossRef] [PubMed]
- Maier, O.; Wilms, M.; Von Der Gablentz, J.; Krämer, U.M.; Münte, T.F.; Handels, H. Extra Tree forests for sub-acute ischemic stroke lesion segmentation in MR sequences. J. Neurosci. Methods 2015, 240, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Scalzo, F.; Hao, Q.; Alger, J.R.; Hu, X.; Liebeskind, D.S. Regional Prediction of Tissue Fate in Acute Ischemic Stroke. Ann. Biomed. Eng. 2012, 40, 2177–2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemmling, A.; Flottmann, F.; Forkert, N.D.; Minnerup, J.; Heindel, W.; Thomalla, G.; Eckert, B.; Knauth, M.; Psychogios, M.; Langner, S.; et al. Multivariate dynamic prediction of ischemic infarction and tissue salvage as a function of time and degree of recanalization. Br. J. Pharmacol. 2015, 35, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- McKinley, R.; Hani, L.; Gralla, J.; El-Koussy, M.; Bauer, S.; Arnold, M.; Fischer, U.; Jung, S.; Mattmann, K.; Reyes, M.; et al. Fully automated stroke tissue estimation using random forest classifiers (FASTER). J. Cereb. Blood Flow Metab. 2017, 37, 2728–2741. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.; Kemmling, A.; Bouteldja, N.; Aulmann, L.F.; Mamlouk, A.M.; Heinrich, M.P. Learning to Predict Ischemic Stroke Growth on Acute CT Perfusion Data by Interpolating Low-Dimensional Shape Representations. Front. Neurol. 2018, 9, 989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuang, H.; Najm, M.; Chakraborty, D.; Maraj, N.; Sohn, S.I.; Goyal, M.; Hill, M.D.; Demchuk, A.M.; Menon, B.K.; Qiu, W. Automated ASPECTS on Noncontrast CT Scans in Patients with Acute Ischemic Stroke Using Machine Learning. AJNR Am. J. Neuroradiol. 2019, 40, 33–38. [Google Scholar] [CrossRef]
- Herweh, C.A.; Ringleb, P.; Rauch, G.; Gerry, S.; Behrens, L.; Möhlenbruch, M.; Gottorf, R.; Richter, D.; Schieber, S.; Nagel, S. Performance of e-ASPECTS software in comparison to that of stroke physicians on assessing CT scans of acute ischemic stroke patients. Int. J. Stroke 2016, 11, 438–445. [Google Scholar] [CrossRef]
- Kwon, J.M.; Kim, K.H.; Jeon, K.H.; Park, J. Deep learning for predicting in-hospital mortality among heart disease patients based on echocardiography. Echocardiography 2019, 36, 213–218. [Google Scholar] [CrossRef]
- Li, Y.; Rapkin, B.; Atkinson, T.M.; Schofield, E.; Bochner, B.H. Leveraging Latent Dirichlet Allocation in processing free-text personal goals among patients undergoing bladder cancer surgery. Qual. Life Res. 2019, 28, 1441–1455. [Google Scholar] [CrossRef]
- Valle, D.; Albuquerque, P.; Zhao, Q.; Barberan, A.; Fletcher, R.J. Extending the Latent Dirichlet Allocation model to presence/absence data: A case study on North American breeding birds and biogeographic shifts expected from climate change. Glob. Chang. Biol. 2018, 24, 5560–5572. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zare, A.; Trinh, H.N.; Omotara, G.O.; Cobb, J.T.; Lagaunne, T.A. Partial Membership Latent Dirichlet Allocation for Soft Image Segmentation. IEEE Trans. Image Process. 2017, 26, 5590–5602. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.M.; Wei, C.P.; Hsiao, F.Y. Modeling healthcare data using multiple-channel latent Dirichlet allocation. J. Biomed. Inform. 2016, 60, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Murthy, D. Modeling virtual organizations with Latent Dirichlet Allocation: A case for natural language processing. Neural Netw. 2014, 58, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Bastanlar, Y.; Ozuysal, M. Introduction to machine learning. Methods Mol. Biol. 2014, 1107, 105–128. [Google Scholar] [CrossRef] [PubMed]
- Pakhomov, S.S.; Hemingway, H.; Weston, S.A.; Jacobsen, S.J.; Rodeheffer, R.; Roger, V.L. Epidemiology of angina pectoris: Role of natural language processing of the medical record. Am. Heart J. 2007, 153, 666–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, S.Y.; Chuang, Y.C.; Kang, T.W.; Tseng, K.H.; Peng, S.Y.; Chuang, Y.C.; Kang, T.W.; Tseng, K.H. Random forest can predict 30-day mortality of spontaneous intracerebral hemorrhage with remarkable discrimination. Eur. J. Neurol. 2010, 17, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.R.; Robbins, J.M.; Kurgansky, K.E.; Imran, T.; Orkaby, A.R.; McLean, R.R.; Ho, Y.L.; Cho, K.; Michael Gaziano, J.; Djousse, L.; et al. Development and validation of a heart failure with preserved ejection fraction cohort using electronic medical records. BMC Cardiovasc. Disord. 2018, 18, 128. [Google Scholar] [CrossRef] [PubMed]
- Bonato, P. Advances in wearable technology and its medical applications. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; Volume 2010, pp. 2021–2024. [Google Scholar]
- Loh, E. Medicine and the rise of the robots: A qualitative review of recent advances of artificial intelligence in health. BMJ Lead. 2018, 2, 59–63. [Google Scholar] [CrossRef]
- Char, D.S.; Shah, N.H.; Magnus, D. Implementing Machine Learning in Health Care—Addressing Ethical Challenges. N. Engl. J. Med. 2018, 378, 981–983. [Google Scholar] [CrossRef]
- Panch, T.; Szolovits, P.; Atun, R. Artificial intelligence, machine learning and health systems. J. Glob. Health 2018, 8, 020303. [Google Scholar] [CrossRef] [PubMed]
- Deo, R.C. Machine Learning in Medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.J.; Katz, D.H.; Selvaraj, S.; Burke, M.A.; Yancy, C.W.; Gheorghiade, M.; Bonow, R.O.; Huang, C.C.; Deo, R.C. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation 2015, 131, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.H.; Sangoi, A.R.; Leung, S.; Marinelli, R.J.; Nielsen, T.O.; Van De Vijver, M.J.; West, R.B.; Van De Rijn, M.; Koller, D. Systematic Analysis of Breast Cancer Morphology Uncovers Stromal Features Associated with Survival. Sci. Transl. Med. 2011, 3, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Golden, J.A. Deep Learning Algorithms for Detection of Lymph Node Metastases from Breast Cancer: Helping Artificial Intelligence Be Seen. JAMA 2017, 318, 2184–2186. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Data | Unit of Analysis | Analytical Methods | Presentations of Results |
|---|---|---|---|
| Keywords, Countries | Words | Frequency of co-occurrence | Map of keywords clusters |
| Abstracts | Words | Exploratory factors analyses | Top 50 constructed research domains Clustering map of the landscapes constructed by these domains. |
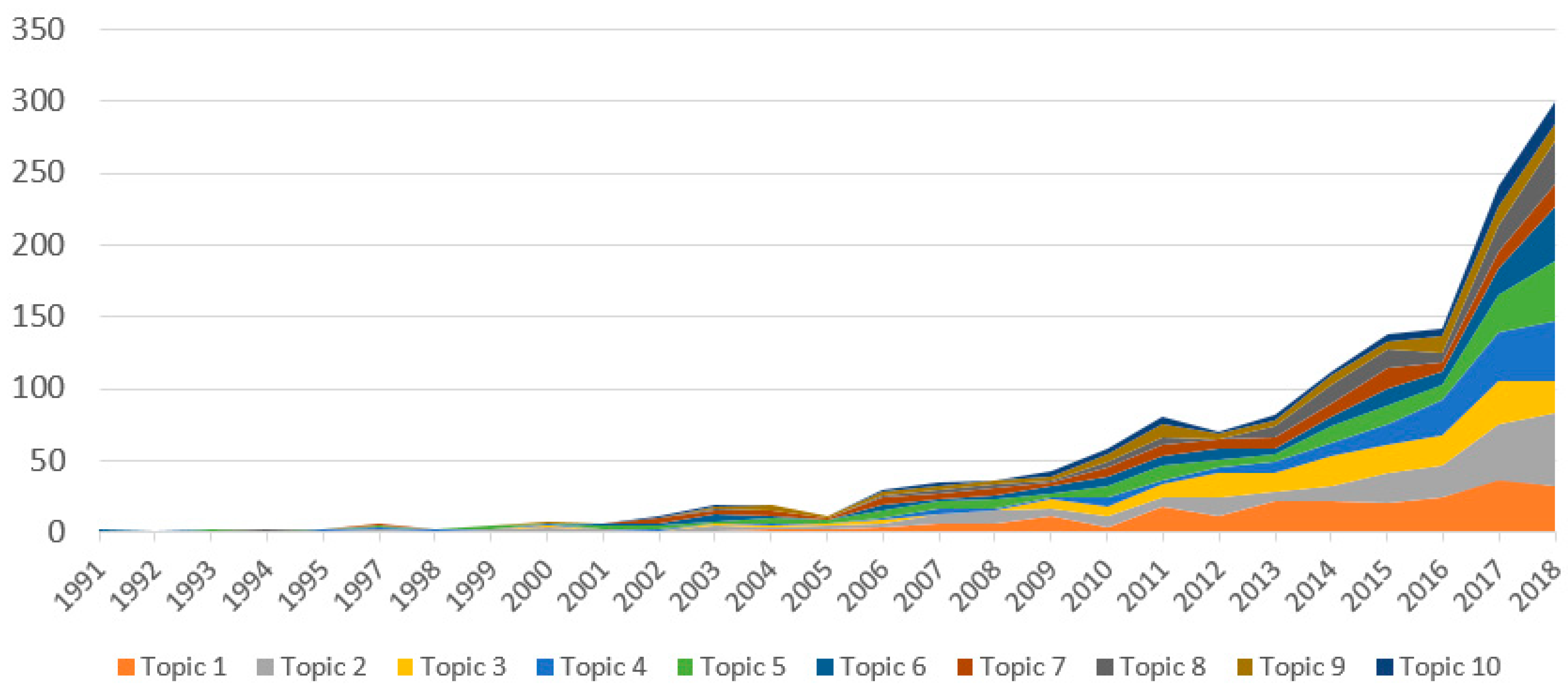
| Abstracts | Papers | Latent Dirichlet allocation | 10 classifications of research topics |
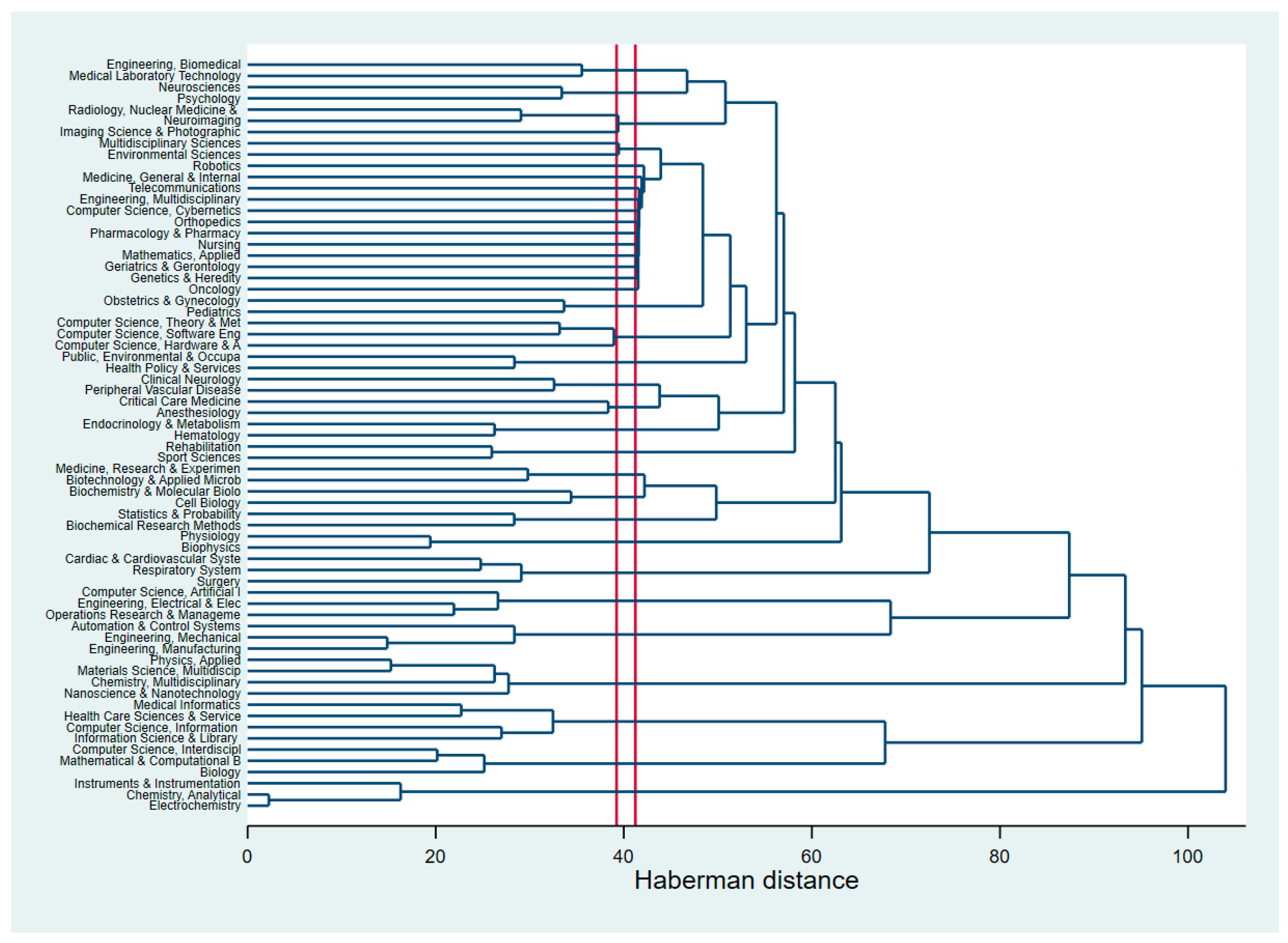
| WoS classification of research areas | WoS research areas | Haberman distance | Dendrogram of research disciplines |
| Year Published | Total Number of Papers | Total Citations | Mean Cite Rate per Year | Total Usage in the Last 6 Months | Total Usage in the Last 5 Years | Mean Use Rate in the Last 6 Months | Mean Use Rate in the Last 5 Years |
|---|---|---|---|---|---|---|---|
| 2018 | 358 | 345 | 0.96 | 1968 | 3289 | 5.50 | 1.84 |
| 2017 | 273 | 1571 | 2.88 | 903 | 4139 | 3.31 | 3.03 |
| 2016 | 157 | 1149 | 2.44 | 287 | 2542 | 1.83 | 3.24 |
| 2015 | 152 | 1720 | 2.83 | 196 | 2424 | 1.29 | 3.19 |
| 2014 | 131 | 1884 | 2.88 | 136 | 2193 | 1.04 | 3.35 |
| 2013 | 100 | 1725 | 2.88 | 75 | 1819 | 0.75 | 3.64 |
| 2012 | 80 | 1903 | 3.40 | 85 | 1480 | 1.06 | 3.70 |
| 2011 | 91 | 3086 | 4.24 | 128 | 1724 | 1.41 | 3.79 |
| 2010 | 64 | 1827 | 3.17 | 42 | 708 | 0.66 | 2.21 |
| 2009 | 54 | 2481 | 4.59 | 58 | 859 | 1.07 | 3.18 |
| 2008 | 44 | 1751 | 3.62 | 32 | 483 | 0.73 | 2.20 |
| 2007 | 39 | 2032 | 4.34 | 25 | 438 | 0.64 | 2.25 |
| 2006 | 39 | 1956 | 3.86 | 33 | 503 | 0.85 | 2.58 |
| 2005 | 15 | 694 | 3.30 | 10 | 136 | 0.67 | 1.81 |
| 2004 | 23 | 650 | 1.88 | 6 | 75 | 0.26 | 0.65 |
| 2003 | 21 | 1373 | 4.09 | 20 | 222 | 0.95 | 2.11 |
| 2002 | 13 | 243 | 1.10 | 5 | 27 | 0.38 | 0.42 |
| 2001 | 8 | 304 | 2.11 | 3 | 39 | 0.38 | 0.98 |
| 2000 | 8 | 672 | 4.42 | 9 | 89 | 1.13 | 2.23 |
| 1999 | 8 | 494 | 3.09 | 4 | 65 | 0.50 | 1.63 |
| 1998 | 3 | 26 | 0.41 | 1 | 1 | 0.33 | 0.07 |
| 1997 | 8 | 926 | 5.26 | 13 | 122 | 1.63 | 3.05 |
| 1995 | 3 | 25 | 0.35 | 0 | 3 | 0.00 | 0.20 |
| 1994 | 2 | 51 | 1.02 | 0 | 2 | 0.00 | 0.20 |
| 1993 | 3 | 51 | 0.65 | 0 | 2 | 0.00 | 0.13 |
| 1992 | 1 | 10 | 0.37 | 0 | 1 | 0.00 | 0.20 |
| 1991 | 2 | 4 | 0.07 | 0 | 2 | 0.00 | 0.20 |
| No. | Country Settings | Frequency | % | No. | Country | Frequency | % |
|---|---|---|---|---|---|---|---|
| 1 | United States | 108 | 44.1% | 19 | Czech | 2 | 0.8% |
| 2 | Ireland | 25 | 10.2% | 20 | France | 2 | 0.8% |
| 3 | Italy | 15 | 6.1% | 21 | Netherlands | 2 | 0.8% |
| 4 | India | 14 | 5.7% | 22 | Singapore | 2 | 0.8% |
| 5 | Australia | 9 | 3.7% | 23 | United Arab Emirates | 2 | 0.8% |
| 6 | Japan | 8 | 3.3% | 24 | Antarctica | 1 | 0.4% |
| 7 | Taiwan | 6 | 2.4% | 25 | Brazil | 1 | 0.4% |
| 8 | Spain | 5 | 2.0% | 26 | Bulgaria | 1 | 0.4% |
| 9 | United Kingdom | 5 | 2.0% | 27 | Egypt | 1 | 0.4% |
| 10 | Germany | 4 | 1.6% | 28 | Greece | 1 | 0.4% |
| 11 | Israel | 4 | 1.6% | 29 | Jordan | 1 | 0.4% |
| 12 | Switzerland | 4 | 1.6% | 30 | Malaysia | 1 | 0.4% |
| 13 | Iran | 3 | 1.2% | 31 | Mexico | 1 | 0.4% |
| 14 | Poland | 3 | 1.2% | 32 | New Zealand | 1 | 0.4% |
| 15 | Saudi Arabia | 3 | 1.2% | 33 | Pakistan | 1 | 0.4% |
| 16 | Austria | 2 | 0.8% | 34 | Sweden | 1 | 0.4% |
| 17 | Canada | 2 | 0.8% | 35 | Tunisia | 1 | 0.4% |
| 18 | China | 2 | 0.8% | 36 | Turkey | 1 | 0.4% |
| No. | Name | Keywords | Eigen-Value | Freq. | % of Cases |
|---|---|---|---|---|---|
| 1 | Fugl-Meyer; upper | Fugl; meyer; upper; motor; rehabilitation; Fugl-Meyer (FMA); limb; extremity; impairment; arm; reaching; improvements; weeks; therapy; stroke | 19.3 | 758 | 53.8% |
| 2 | Support vector; machine (SVM) | Vector; svm; support; feature; classification; machine; heart rate variability (HRV) | 6.8 | 385 | 48.8% |
| 3 | Coronary artery bypass; surgery | Bypass; surgery; postoperative; endoscopic; surgical; invasive; procedures; left; underwent; coronary; times | 4.8 | 273 | 33.3% |
| 4 | Blood pressure (BP) | Pressure; blood; bp; tilt | 3.8 | 63 | 10.8% |
| 5 | Flexion; joint | Flexion; joint; elbow; passive; motion; movements; healthy; range | 3.4 | 244 | 34.1% |
| 6 | Neural network | Neural; artificial; network; artificial neural network (ANN); networks | 3.3 | 256 | 27.8% |
| 7 | Predict | Area under the curve (AUC); Rheumatoid factor (RF); random; predicting; predictive; predict | 3.2 | 134 | 22.6% |
| 8 | Gait; walking | Gait; walking; lokomat; practice; phase; training | 3.0 | 192 | 33.1% |
| 9 | Machine learning; heart disease | Machine; learning; disease; accuracy; classification; prediction; risk; heart | 2.9 | 811 | 72.7% |
| 10 | Fuzzy; systems | Fuzzy; systems; expert; decision; problem; medical | 2.8 | 224 | 39.1% |
| 11 | Sensitivity | Sensitivity; specificity; detection; predictive | 2.6 | 137 | 21.3% |
| 12 | Mitral valve; repair | Valve; mitral; repair; underwent | 2.5 | 62 | 10.0% |
| 13 | Brain; hand | Brain; hand; stimulation; plasticity; movements; functional; brain-computer interfaces (BCI) | 2.5 | 197 | 29.4% |
| 14 | Randomized controlled; assisted | Controlled; randomized; assisted; conventional; improvement; functional; efficacy; treatment | 2.4 | 386 | 49.9% |
| 15 | Assistance; finger | Assistance; finger; virtual; demonstrated; activities | 2.4 | 106 | 19.7% |
| 16 | Image | Images; image; computed tomography (CT); deep | 2.4 | 58 | 10.2% |
| 17 | Observed; effects | Observed; effects; week; post | 2.3 | 129 | 23.4% |
| 18 | Sensor; healthcare | Sensor; healthcare; monitoring; framework | 2.1 | 73 | 15.5% |
| 19 | Complications; respiratory | Complications; respiratory; cardiac | 2.1 | 88 | 17.6% |
| 20 | Exercise; subjects | Exercise; subjects; peak; tilt | 2.1 | 106 | 22.3% |
| 21 | State; applied | State; applied; field | 2.1 | 104 | 21.5% |
| 22 | Atrial | Atrial; atrial fibrillation (AF); catheter; procedure | 2.0 | 61 | 11.3% |
| 23 | Paper | Paper; presents; proposed; experimental | 2.0 | 243 | 39.4% |
| 24 | Space; terms | Space; terms; values | 2.0 | 62 | 13.4% |
| 25 | Coronary artery; carotid | Artery; coronary; carotid; myocardial; disease; risk | 2.0 | 261 | 39.9% |
| 26 | Clinical | Clinical; recent | 2.0 | 160 | 37.5% |
| 27 | Conditions; future | Conditions; future; tested; healthy | 1.9 | 155 | 29.1% |
| 28 | Variables; models | Variables; models; selected; develop; predict | 1.9 | 167 | 30.5% |
| 29 | Physical activity; wearable | Physical; wearable; devices; activity; technology | 1.9 | 185 | 32.0% |
| 30 | Chronic | Chronic; combined; weeks; week | 1.9 | 133 | 23.4% |
| 31 | Able; user | Able; user; process; tested; wearable | 1.8 | 135 | 25.2% |
| 32 | Diabetes; classifier | Diabetes; classifier; ensemble; dataset; classifiers; cancer; problems | 1.8 | 147 | 23.1% |
| 33 | Muscle; guidance | Muscle; guidance | 1.8 | 29 | 6.8% |
| 34 | Parameters | Parameters; error | 1.8 | 72 | 16.8% |
| 35 | Validation | Validation; cancer; lung | 1.8 | 63 | 13.1% |
| 36 | Severe; visual | Severe; visual; feedback | 1.8 | 66 | 13.7% |
| 37 | Mortality; failure | Mortality; failure; outcomes; myocardial; hospital | 1.7 | 179 | 29.9% |
| 38 | Trained; set | Trained; set; sets; validation | 1.7 | 125 | 23.1% |
| 39 | Propose; terms | Propose; terms; show | 1.7 | 101 | 21.5% |
| 40 | End; task | End; task; position; measured | 1.7 | 124 | 24.2% |
| 41 | Robot | Robots; robot; therapy; field; intensity | 1.7 | 213 | 34.1% |
| 42 | Multiple; index | Multiple; index; sleep; events | 1.7 | 92 | 19.4% |
| 43 | Patterns | Patterns; pattern; potential; duration | 1.6 | 119 | 25.5% |
| 44 | Technique; diagnosis | Technique; diagnosis; techniques | 1.6 | 128 | 26.8% |
| 45 | Stroke | Stroke | 1.6 | 168 | 44.1% |
| 46 | Pre; post | Pre; post; effective | 1.6 | 117 | 22.6% |
| 47 | Quality | Quality; life | 1.6 | 70 | 15.0% |
| 48 | Provided; differences | Provided; differences; acute | 1.6 | 86 | 18.6% |
| 49 | Development; role | Development; role; plasticity | 1.6 | 76 | 16.3% |
| 50 | Electrocardiogram (ECG); signals; arrhythmia | Electrocardiogram (ECG); arrhythmia; database; frequency; signals; normal; classifiers; cardiac | 1.6 | 225 | 34.9% |
| Year | Research Areas | Frequency | Percent |
|---|---|---|---|
| Topic 1 | Reviews of AI and robotics in healthcare | 234 | 15.9% |
| Topic 2 | AI for big data analysis (genetics, metabolic studies) | 217 | 14.8% |
| Topic 3 | Robotically-assisted cardiac surgery | 170 | 11.6% |
| Topic 4 | Robotic prosthesis | 167 | 11.4% |
| Topic 5 | Robotics-assisted stroke rehabilitation | 167 | 11.4% |
| Topic 6 | Minimally invasive surgery | 130 | 8.8% |
| Topic 7 | AI for medical diagnostics | 118 | 8.0% |
| Topic 8 | AI for population identification | 110 | 7.5% |
| Topic 9 | AI-assisted biometric assessment | 90 | 6.1% |
| Topic 10 | AI interpretation of medical investigations | 66 | 4.5% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, B.X.; Latkin, C.A.; Vu, G.T.; Nguyen, H.L.T.; Nghiem, S.; Tan, M.-X.; Lim, Z.-K.; Ho, C.S.H.; Ho, R.C.M. The Current Research Landscape of the Application of Artificial Intelligence in Managing Cerebrovascular and Heart Diseases: A Bibliometric and Content Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2699. https://doi.org/10.3390/ijerph16152699
Tran BX, Latkin CA, Vu GT, Nguyen HLT, Nghiem S, Tan M-X, Lim Z-K, Ho CSH, Ho RCM. The Current Research Landscape of the Application of Artificial Intelligence in Managing Cerebrovascular and Heart Diseases: A Bibliometric and Content Analysis. International Journal of Environmental Research and Public Health. 2019; 16(15):2699. https://doi.org/10.3390/ijerph16152699
Chicago/Turabian StyleTran, Bach Xuan, Carl A. Latkin, Giang Thu Vu, Huong Lan Thi Nguyen, Son Nghiem, Ming-Xuan Tan, Zhi-Kai Lim, Cyrus S.H. Ho, and Roger C.M. Ho. 2019. "The Current Research Landscape of the Application of Artificial Intelligence in Managing Cerebrovascular and Heart Diseases: A Bibliometric and Content Analysis" International Journal of Environmental Research and Public Health 16, no. 15: 2699. https://doi.org/10.3390/ijerph16152699