Travelers to U.S.: Zika Virus Knowledge, Attitudes, and Determinants of Practices in the Middle East—Insights for Future Awareness Campaigns

Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Study Design and Data Collection
2.3. Statistical Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Knowledge about Zika infection
3.3. Multivariate Linear Regression Model for the Factors Associated with High Knowledge Score
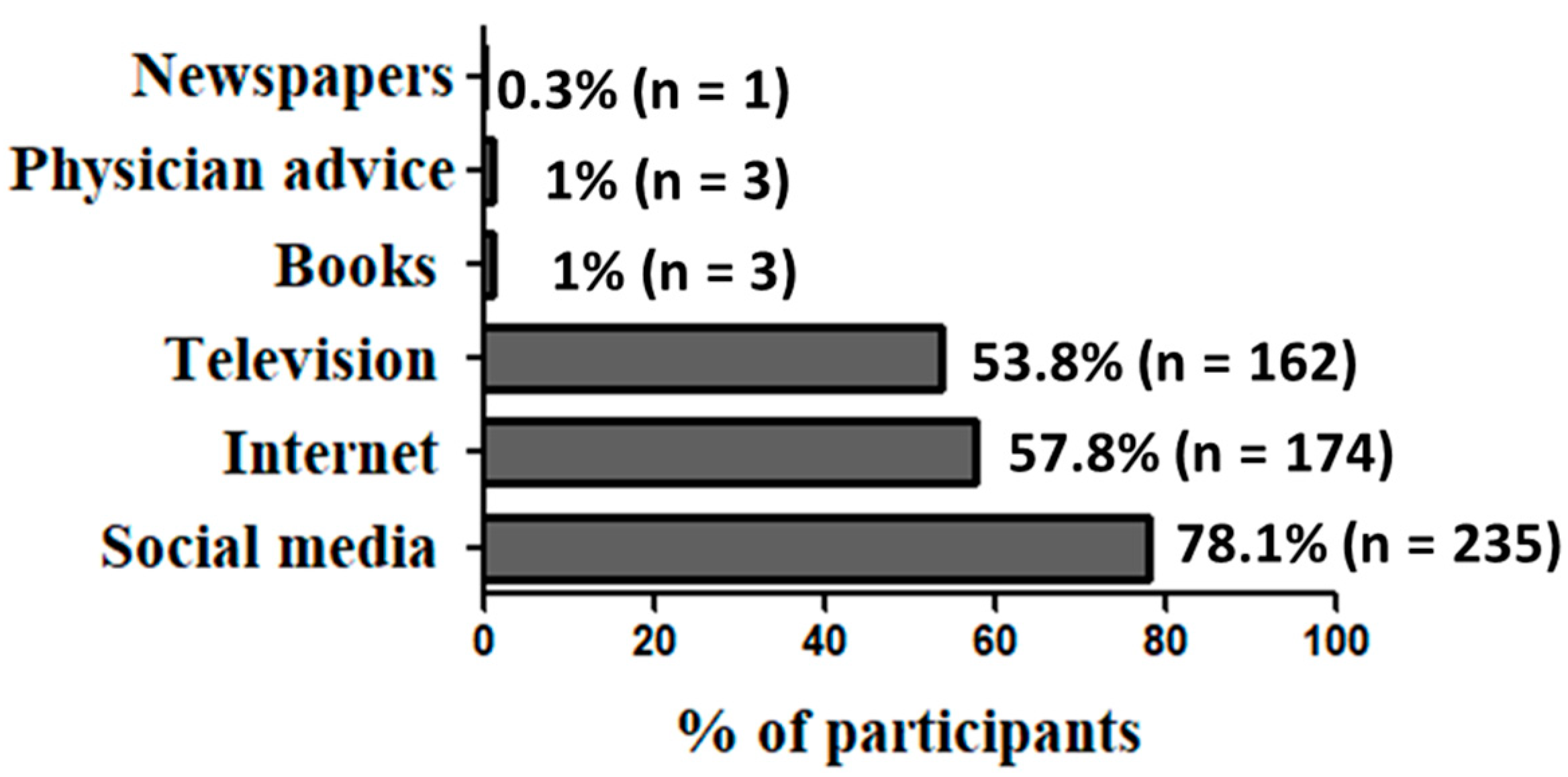
3.4. Sources of Information about Zika Infection
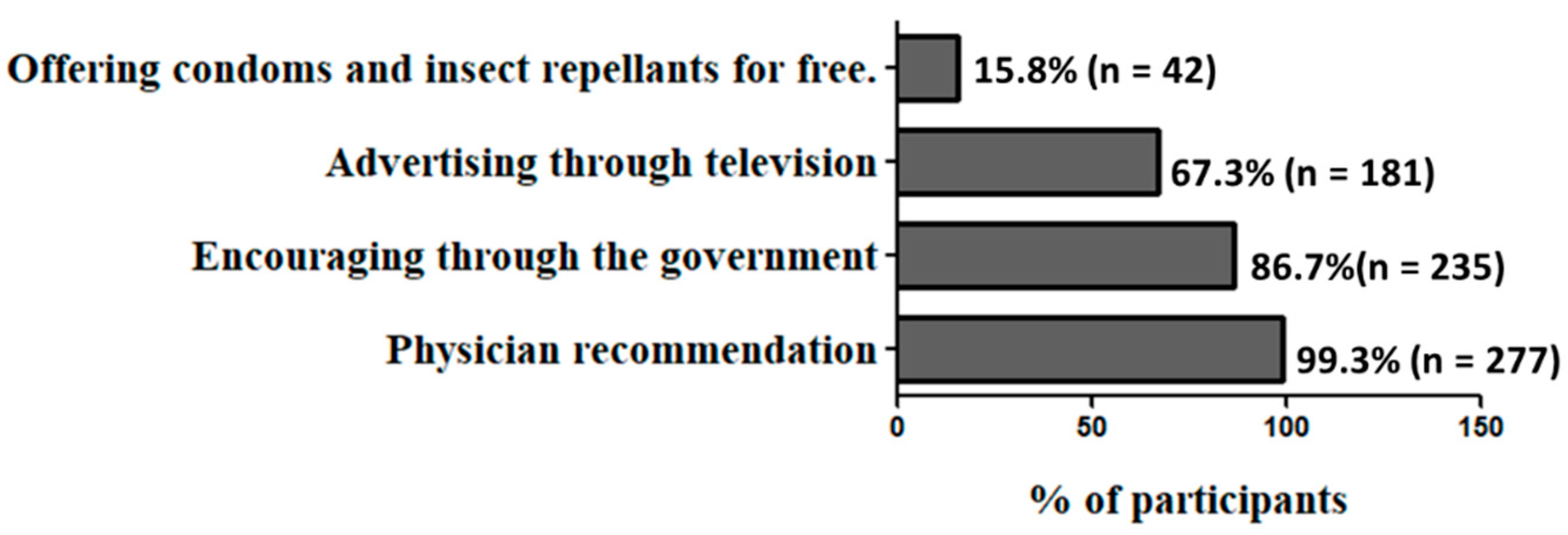
3.5. Attitude of Participants towards Zika and Its Prevention Measures
3.6. Factors Associated with Population Adherence to Zika Prevention Measures
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Benelli, G.; Romano, D. Mosquito vectors of Zika virus. Entomol. Gen. 2017, 36, 309–318. [Google Scholar] [CrossRef]
- Al-Qahtani, A.A.; Nazir, N.; Al-Anazi, M.R.; Rubino, S.; Al-Ahdal, M.N. Zika virus: A new pandemic threat. J. Infect. Dev. Ctries. 2016, 10, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Ampudia, Y.; Monsalve, D.M.; Castillo-Medina, L.F.; Rodríguez, Y.; Pacheco, Y.; Halstead, S.; Willison, H.J.; Anaya, J.-M.; Ramírez-Santana, C. Autoimmune neurological conditions associated with Zika virus infection. Front. Mol. Neurosci. 2018, 11, 116. [Google Scholar] [CrossRef] [PubMed]
- Hamer, D.H.; Barbre, K.A.; Chen, L.H.; Grobusch, M.P.; Schlagenhauf, P.; Goorhuis, A.; van Genderen, P.J.; Molina, I.; Asgeirsson, H.; Kozarsky, P.E.; et al. Travel-Associated Zika Virus Disease Acquired in the Americas Through February 2016: A GeoSentinel Analysis. Ann. Intern. Med. 2017, 166, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.; Gubler, D.J.; Weaver, S.C.; Monath, T.P.; Heymann, D.L.; Scott, T.W. Epidemic arboviral diseases: Priorities for research and public health. Lancet Infect. Dis. 2017, 17, e101–e106. [Google Scholar] [CrossRef]
- Pyke, A.T.; Moore, P.R.; Hall-Mendelin, S.; McMahon, J.L.; Harrower, B.J.; Constantino, T.R.; van den Hurk, A.F. Isolation of Zika virus imported from Tonga into Australia. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- Jia, H.; Zhang, M.; Chen, M.; Yang, Z.; Li, J.; Huang, G.; Guan, D.; Cen, X.; Zhang, L.; Feng, Q.; et al. Zika virus infection in travelers returning from countries with local transmission, Guangdong, China, 2016. Travel Med. Infect. Dis. 2018, 21, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Nicastri, E.; Pisapia, R.; Corpolongo, A.; Fusco, F.M.; Cicalini, S.; Scognamiglio, P.; Castilletti, C.; Bordi, L.; Di Caro, A.; Capobianchi, M.R.; et al. Three cases of Zika virus imported in Italy: Need for a clinical awareness and evidence-based knowledge. BMC Infect. Dis. 2016, 16, 669. [Google Scholar] [CrossRef]
- Meltzer, E.; Lustig, Y.; Leshem, E.; Levy, R.; Gottesman, G.; Weissmann, R.; Rabi, D.H.; Hindiyeh, M.; Koren, R.; Mendelson, E.; et al. Zika virus disease in traveler returning from Vietnam to Israel. Emerg. Infect. Dis. 2016, 22, 1521–1522. [Google Scholar] [CrossRef]
- PAHO and WHO. Available online: https://www.paho.org/hq/index.php?option=com_content&view=article&id=12390:zika-cumulative-cases&Itemid=42090&lang=en (accessed on 15 December 2018).
- Centers for Disease Control and Prevention (CDC). Available online: https://wwwnc.cdc.gov/travel/page/zika-travel-information (accessed on 12 June 2019).
- Fédération Internationale de Football Association (FIFA). Available online: https://www.fifa.com/worldcup/qatar2022/ (accessed on 9 July 2019).
- Ducheyne, E.; Tran Minh, N.N.; Haddad, N.; Bryssinckx, W.; Buliva, E.; Simard, F.; Malik, M.R.; Charlier, J.; De Waele, V.; Mahmoud, O.; et al. Current and future distribution of Aedes aegypti and Aedes albopictus (Diptera: Culicidae) in WHO Eastern Mediterranean Region. Int. J. Health Geogr. 2018, 17, 4. [Google Scholar] [CrossRef]
- Kanani, K.; Amr, Z.; Katbeh-Bader, A.; Arbaji, M. First record of Aedes albopictus in Jordan. J. Am. Mosq. Control Assoc. 2017, 33, 134–135. [Google Scholar] [CrossRef] [PubMed]
- Sweileh, W.M. Global research output in the health of international Arab migrants (1988–2017). BMC Public Health 2018, 18, 755. [Google Scholar] [CrossRef] [PubMed]
- Pew Research Center. Available online: http://www.pewglobal.org/2016/10/18/middle-easts-migrant-population-more-than-doubles-since-2005/ (accessed on 15 December 2018).
- Centers for Disease Control and Prevention (CDC). Available online: https://www.cdc.gov/zika/healtheffects/index.html (accessed on 15 April 2017).
- Squiers, L.; Herrington, J.; Kelly, B.; Bann, C.; Becker-Dreps, S.; Stamm, L.; Johnson, M.; McCormack, L. Zika Virus Prevention: U.S. Travelers’ Knowledge, Risk Perceptions, and Behavioral Intentions—A National Survey. Am. J. Trop. Med. Hyg. 2018, 98, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Abu-rish, E.Y.; Elayeh, E.R.; Albsoul-Younes, A.M. The Role of the Middle East in ZIKA Virus Circulation: Implications of a Cross-Sectional Study in Jordan. Am. J. Trop. Med. Hyg. 2019, 100, 974–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atif, M.; Azeem, M.; Sarwar, M.R.; Bashir, A. Zika virus disease: A current review of the literature. Infection 2016, 44, 695–705. [Google Scholar] [CrossRef]
- Abu-Rish, E.Y.; Elayeh, E.R.; Mousa, L.A.; Butanji, Y.K.; Albsoul-Younes, A.M. Knowledge, awareness and practices towards seasonal influenza and its vaccine: Implications for future vaccination campaigns in Jordan. Fam. Pract. 2016, 33, 690–697. [Google Scholar] [CrossRef]
- Mouchtouri, V.A.; Papagiannis, D.; Katsioulis, A.; Rachiotis, G.; Dafopoulos, K.; Hadjichristodoulou, C. Knowledge, attitudes, and practices about the prevention of mosquito bites and Zika virus disease in pregnant women in Greece. Int. J. Environ. Res. Public Health 2017, 14, 367. [Google Scholar] [CrossRef]
- Samuel, G.; DiBartolo-Cordovano, R.; Taj, I.; Merriam, A.; Lopez, J.M.; Torres, C.; Lantigua, R.A.; Morse, S.; Chang, B.P.; Gyamfi-Bannerman, C.; et al. A survey of the knowledge, attitudes and practices on Zika virus in New York City. BMC Public Health 2018, 18, 98. [Google Scholar] [CrossRef]
- Howells, M.E.; Lynn, C.D.; Weaver, L.J.; Langford-Sesepesara, M.; Tufa, J. Zika virus in American Samoa: Challenges to prevention in the context of health disparities and non-communicable disease. Ann. Hum. Biol. 2018, 45, 229–238. [Google Scholar] [CrossRef]
- Cheema, S.; Maisonneuve, P.; Weber, I.; Fernandez-Luque, L.; Abraham, A.; Alrouh, H.; Sheikh, J.; Lowenfels, A.B.; Mamtani, R. Knowledge and perceptions about Zika virus in a Middle East country. BMC Infect. Dis. 2017, 17, 524. [Google Scholar] [CrossRef]
- Smith, D. Health care consumer’s use and trust of health information sources. J. Commun. Healthc. 2011, 4, 200–210. [Google Scholar] [CrossRef]
- Berenson, A.B.; Hirth, J.M.; Guo, F.; Fuchs, E.L.; Weaver, S.C. Prevention practices among United States pregnant women who travel to Zika outbreak areas. Am. J. Trop. Med. Hyg. 2018, 98, 178–180. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | (%)1 n | Knowledge score | p-value |
|---|---|---|---|
| Mean ± SD | |||
| Age 2 | |||
| <35 | 48.1 (143) | 8.6 ± 3.2 | 0.004 * |
| ≥35 | 51.9 (154) | 9.6 ± 2.4 | |
| Gender 2 | |||
| Females | 32.2 (97) | 8.7 ± 2.8 | 0.183 |
| Males | 67.8 (204) | 9.2 ± 3.1 | |
| Marital status 3 | |||
| Married | 89.0 (266) | 9.1 ± 2.9 | 0.425 |
| Single | 7.4 (22) | 8.2 ± 3.4 | |
| Others 4 | 3.6 (11) | 8.9 ± 3.4 | |
| Education 2 | |||
| Less than bachelor degree | 16.7 (50) | 7.5 ± 3.4 | 0.001* |
| Bachelor degree or higher | 83.3 (251) | 9.0 ± 2.7 | |
| Employment 2 | |||
| Not working | 18.9 (57) | 8 ± 3.5 | 0.019* |
| Working full time or part time | 81.1 (244) | 9.2 ± 2.7 | |
| Having children 2 | |||
| Yes | 71.3 (211) | 9.0 ± 2.8 | 0.835 |
| No | 28.7 (85) | 8.9 ± 3.2 | |
| Future plans of the partners for pregnancy 2 | |||
| Yes | 46.5 (140) | 9.6 ± 2.7 | 0.001 * |
| No | 53.5 (161) | 8.5 ± 3.0 | |
| First trip to America 2 | |||
| Yes | 10.0 (30) | 8.3 ± 3.0 | 0.105 |
| No | 90.0 (269) | 9.2 ± 2.8 | |
| Visiting America for different purposes (tourism, medical treatment…etc) 2 | |||
| Yes | 95.6 (274) | 9.0 ± 2.9 | 0.873 |
| No | 4.4 (12) | 9.2 ± 2.6 | |
| Nationality 2 | |||
| Jordanian | 48.7 (134) | 9.0 ± 2.8 8.8 ± 3.0 | 0.57 |
| Non-Jordanian | 51.3 (142) | ||
| Palestinian | 5.8 (16) | ||
| Saudi | 6.2 (17) | ||
| Syrian | 5.1 (14) | ||
| Egyptian | 8.7 (24) | ||
| Lebanese | 3.6 (10) | ||
| Iraqi | 8.0 (22) | ||
| Kuwaiti | 4.0 (11) | ||
| Swedish | 4.0 (11) | ||
| Yemeni | 2.2 (6) | ||
| Omani | 2.2 (6) | ||
| Qatari | 1.1 (3) | ||
| Tunisian | 0.4 (1) | ||
| Question | Correctly answered % (n) |
|---|---|
| Definition, signs and symptoms, risk groups, and complications | |
| Zika is a disease caused by a virus that is primarily spread to people through the bite of an infected mosquito. | 7.7 (23) |
| The most common signs and symptoms are fever, rash, joint pain, and conjunctivitis (red eyes). | 79.6 (238) |
| The highest risk group is pregnant women. | 24.1 (72) |
| Complications of Zika infection | |
| Zika infection during pregnancy can cause severe birth defects, including microcephaly. | 2.7 (8) |
| Severe disease requiring hospitalization due to Zika is common.* | 0.3 (1) |
| Death from Zika infection is common.* | 0.3 (1) |
| Mode of transmission | |
| Zika is transmitted primarily through the bite of infected mosquitoes. | 10.4 (31) |
| Sexual contact. | 55.9 (167) |
| Vertically from a pregnant woman to her fetus. | 81.3 (243) |
| Through blood transfusion. | 96.0 (287) |
| Directly from one person to another through casual contact.* | 66.6 (199) |
| From a mother to fetus through breastfeeding.* | 17.1 (51) |
| Prevention measures | |
| Prevention of mosquito bites | |
| The use of insect repellents is necessary to prevent mosquito’s bite. | 71.9 (215) |
| Wearing long-sleeved shirts and long pants is not necessary. * | 69.2 (207) |
| Stay in places with air conditioning or window and door screens. | 76.3 (228) |
| Removing standing water and rubbish around your home. | 75.3 (225) |
| Asymptomatically infected individuals returning from affected areas to non-affected areas should continue the use of insect repellents for a minimum of extra 14 days. | 25.6 (76) |
| Prevention of transmission through sex | |
| Male partners should use condoms (or other barriers) to reduce the chance of getting Zika from sex. | 59.8 (177) |
| Prevention of transmission during pregnancy | |
| Pregnant women should not travel to areas with Zika. | 68.6 (201) |
| Variables | SE | B 1 | T | p-value |
|---|---|---|---|---|
| Constant | 3.444 | - | 3.702 | <0.005 * |
| Age | 0.345 | 0.114 | 1.936 | 0.054 |
| Level of education | 0.472 | 0.202 | 3.393 | 0.001 * |
| Employment | 0.225 | 0.078 | 1.281 | 0.201 |
| Planning for pregnancy | 0.336 | −0.122 | −0.180 | 0.002 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-rish, E.Y.; Elayeh, E.R.; Browning, M.J. Travelers to U.S.: Zika Virus Knowledge, Attitudes, and Determinants of Practices in the Middle East—Insights for Future Awareness Campaigns. Int. J. Environ. Res. Public Health 2019, 16, 2517. https://doi.org/10.3390/ijerph16142517
Abu-rish EY, Elayeh ER, Browning MJ. Travelers to U.S.: Zika Virus Knowledge, Attitudes, and Determinants of Practices in the Middle East—Insights for Future Awareness Campaigns. International Journal of Environmental Research and Public Health. 2019; 16(14):2517. https://doi.org/10.3390/ijerph16142517
Chicago/Turabian StyleAbu-rish, Eman Y., Eman R. Elayeh, and Michael J. Browning. 2019. "Travelers to U.S.: Zika Virus Knowledge, Attitudes, and Determinants of Practices in the Middle East—Insights for Future Awareness Campaigns" International Journal of Environmental Research and Public Health 16, no. 14: 2517. https://doi.org/10.3390/ijerph16142517