Prediction of Computer Vision Syndrome in Health Personnel by Means of Genetic Algorithms and Binary Regression Trees †

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Genetic Algorithms
2.2. Regression Trees
2.3. Study Population
2.4. Data Collection
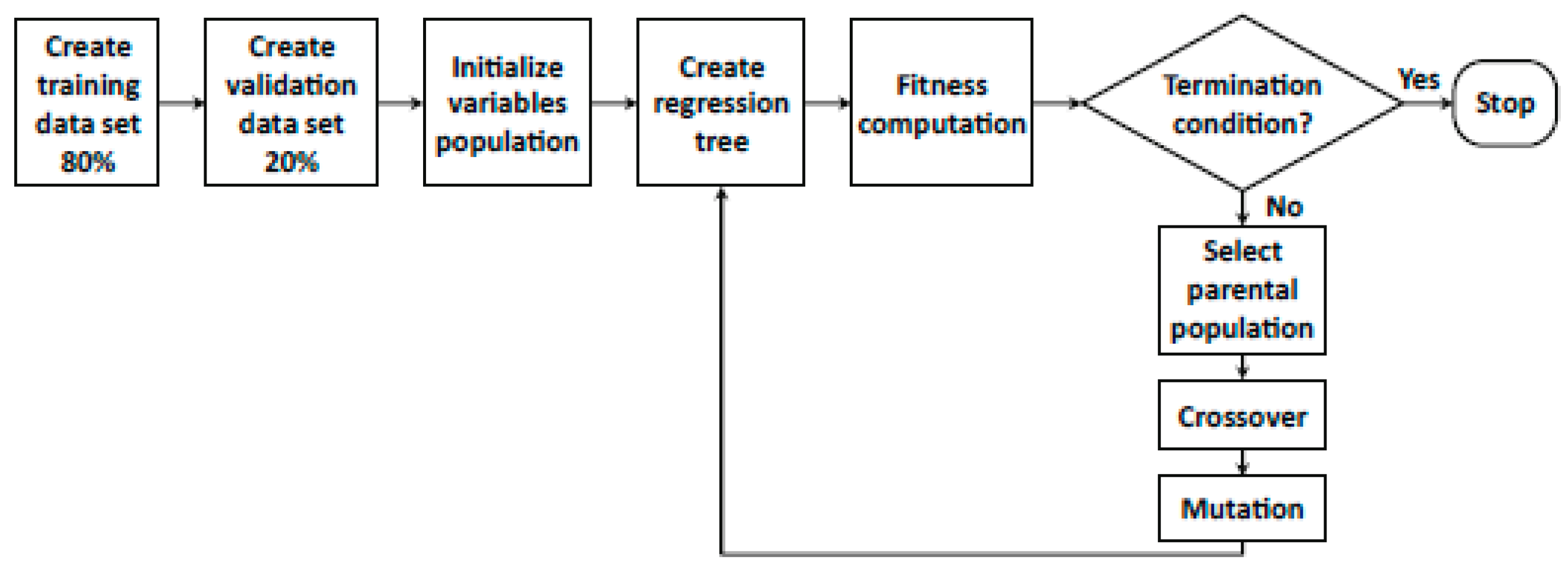
2.5. The Proposed Algorithm
3. Results
3.1. General Characteristics of the Subjects
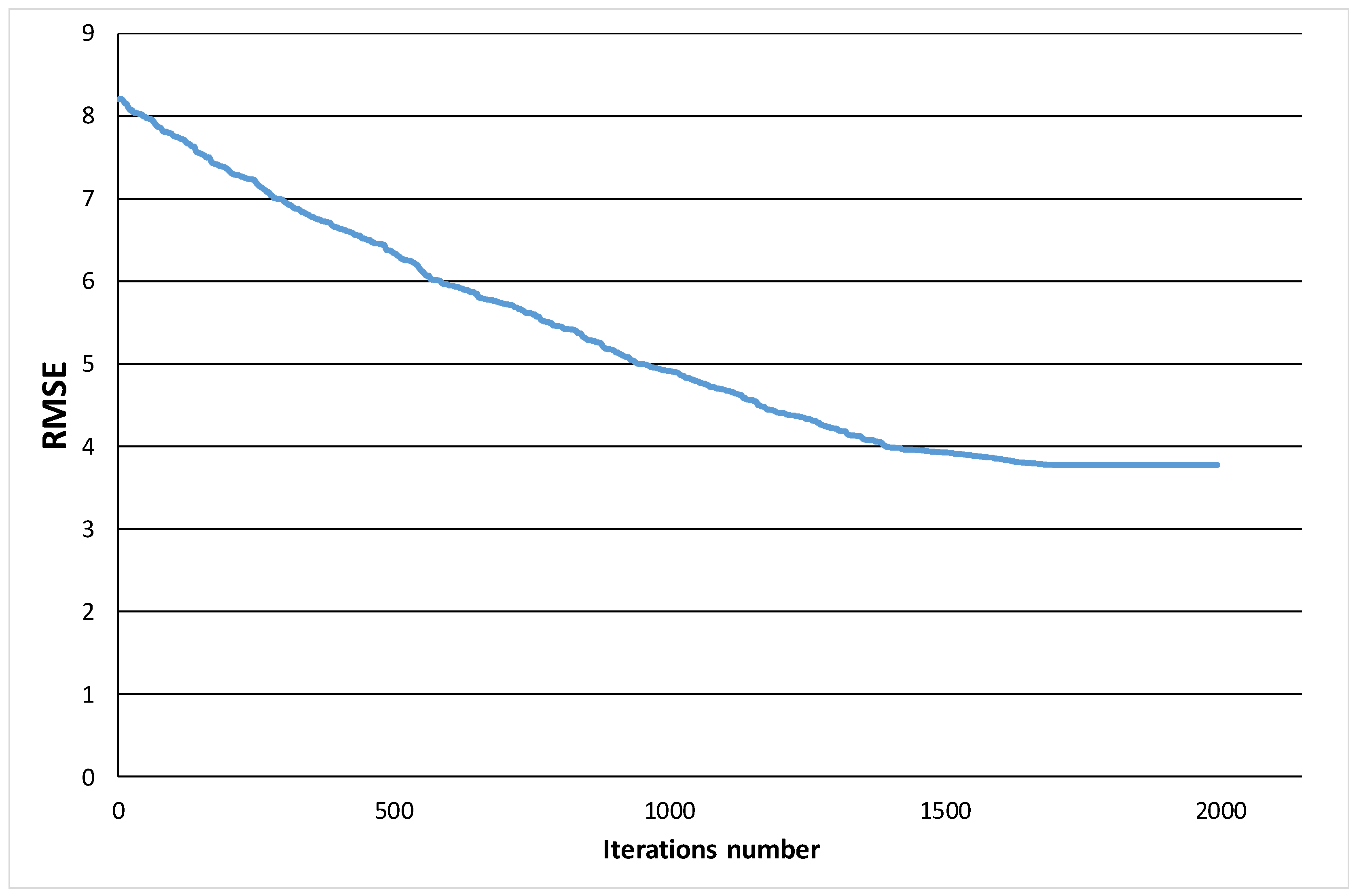
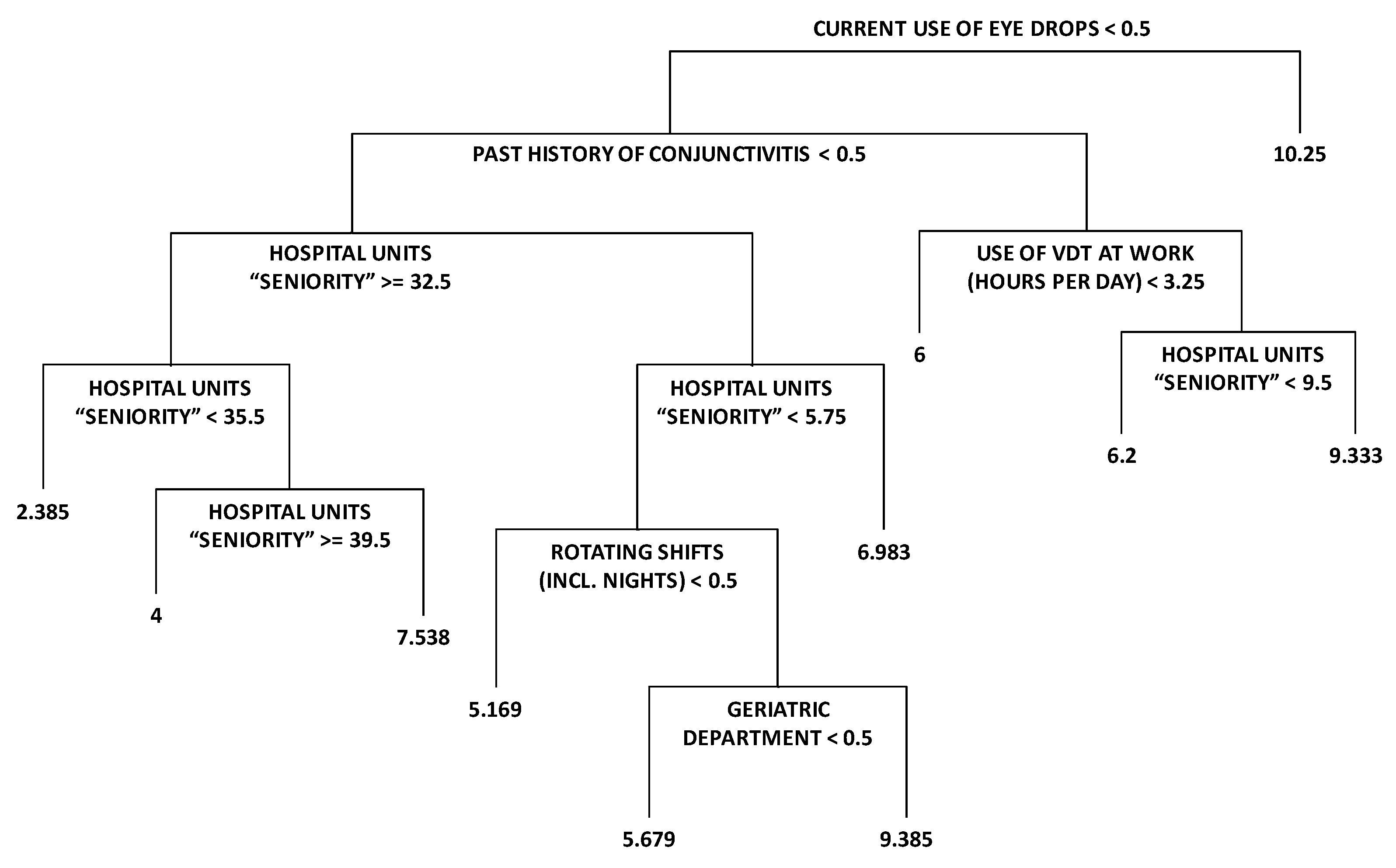
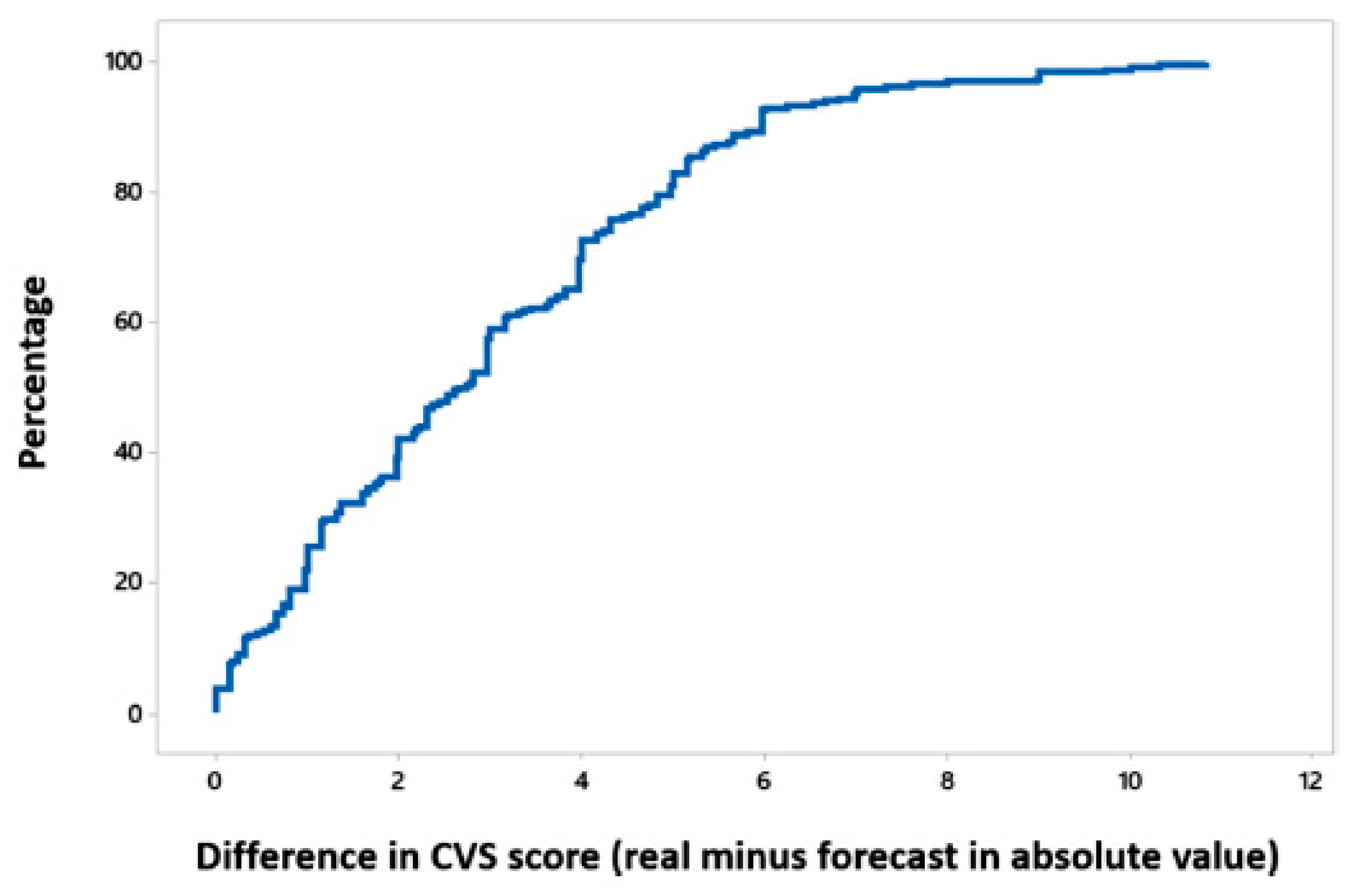
3.2. Implementation of the Algorithm
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parent-Thirion, A.; Biletta, I.; Cabrita, J.; Vargas, O.; Vermeylen, G.; Wilczynska, A.; Wilkens, M. Sixth European Working Conditions Survey–Overview Report (2017 update); Eurofound; Publications Office of the European Union: Luxembourg, 2017; ISBN 978-92-897-1597-3. [Google Scholar]
- Blehm, C.; Vishnu, S.; Khattak, A.; Mitra, S.; Yee, R.W. Computer vision syndrome: A review. Surv. Ophthalmol. 2005, 50, 253–262. [Google Scholar] [CrossRef]
- American Optometric Association. Computer Vision Syndrome. Available online: https://www.aoa.org/patients-and-public/caring-for-your-vision/protecting-your-vision/computer-vision-syndrome (accessed on 16 January 2018).
- Rosenfield, M. Computer vision syndrome: A review of ocular causes and potential treatments. Ophthalmic Physiol. Opt. 2011, 31, 502–515. [Google Scholar] [CrossRef]
- Yan, Z.; Hu, L.; Chen, H.; Lu, F. Computer Vision Syndrome: A widely spreading but largely unknown epidemic among computer users. Comput. Hum. Behav. 2008, 24, 2026–2042. [Google Scholar] [CrossRef]
- Ye, Z.; Abe, Y.; Kusano, Y.; Takamura, N.; Eida, K.; Takemoto, T.; Aoyagi, K. The influence of visual display terminal use on the physical and mental conditions of administrative staff in Japan. J. Physiol. Anthropol. 2007, 26, 69–73. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Wathurapatha, W.S.; Perera, Y.S.; Lamabadusuriya, D.A.; Kulatunga, S.; Jayawardana, N.; Katulanda, P. Computer vision syndrome among computer office workers in a developing country: An evaluation of prevalence and risk factors. BMC Res. Notes 2016, 9, 150. [Google Scholar] [CrossRef]
- Tauste, A.; Ronda, E.; Molina, M.J.; Seguí, M. Effect of contact lens use on computer vision syndrome. Ophthalmic Physiol. Opt. 2016, 36, 112–119. [Google Scholar] [CrossRef]
- Sa, E.C.; Ferreira Junior, M.; Rocha, L.E. Risk factors for computer visual syndrome (CVS) among operators of two call centers in São Paulo, Brazil. Work 2012, 41, 3568–3574. [Google Scholar] [CrossRef]
- Sen, A.; Richardson, S. A study of computer-related upper limb discomfort and computer vision syndrome. J. Hum. Ergol. 2007, 36, 45–50. [Google Scholar] [CrossRef]
- Logaraj, M.; Madhupriya, V.; Hegde, S. Computer vision syndrome and associated factors among medical and engineering students in chennai. Ann. Med. Health Sci. Res. 2014, 4, 179–185. [Google Scholar] [CrossRef]
- Scheiman, M. Accommodative and binocular vision disorders associated with video display terminals: Diagnosis and management issues. J. Am. Optom. Assoc. 1996, 67, 531–539. [Google Scholar]
- Bergqvist, U.O.; Knave, B.G. Eye discomfort and work with visual display terminals. Scand. J. Work Environ. Health 1994, 20, 27–33. [Google Scholar] [CrossRef]
- Fenga, C.; Aragona, P.; Di Nola, C.; Spinella, R. Comparison of ocular surface disease index and tear osmolarity as markers of ocular surface dysfunction in video terminal display workers. Am. J. Ophthalmol. 2014, 158, 41–48. [Google Scholar] [CrossRef]
- Ünlü, C.; Güney, E.; Akçay, B.; Akçali, G.; Erdoğan, G.; Bayramlar, H. Comparison of ocular-surface disease index questionnaire, tearfilm break-up time, and Schirmer tests for the evaluation of the tearfilm in computer users with and without dry-eye symptomatology. Clin. Ophthalmol. 2012, 6, 1303–1306. [Google Scholar] [CrossRef] [Green Version]
- Parihar, J.K.; Jain, V.K.; Chaturvedi, P.; Kaushik, J.; Jain, G.; Parihar, A.K. Computer and visual display terminals (VDT) vision syndrome (CVDTS). Med. J. Armed Forces India 2016, 72, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Seguí, M.M.; Cabrero-García, J.; Crespo, A.; Verdú, J.; Ronda, E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J. Clin. Epidemiol. 2015, 68, 662–673. [Google Scholar] [CrossRef] [Green Version]
- González-Pérez, M.; Susi, R.; Antona, B.; Barrio, A.; González, E. The Computer-Vision Symptom Scale (CVSS17): Development and initial validation. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4504–4511. [Google Scholar] [CrossRef]
- Vertinsky, T.; Forster, B. Prevalence of eye strain among radiologists: Influence of viewing variables on symptoms. AJR Am. J. Roentgenol. 2005, 184, 681–686. [Google Scholar] [CrossRef]
- Aronsson, K.; Teär Fahnehjelm, K.; Nylén, P.; Eklund, J. Visual ergonomics and eye strain in eye careprofessionals. In Proceedings of the 2012 NES Conference on Ergonomics for sustainability and growth, Saltsjöbaden, Sweden, 19–22 August 2012. [Google Scholar]
- Yazici, A.; Sari, E.S.; Sahin, G.; Kilic, A.; Cakmak, H.; Ayar, O.; Ermis, S.S. Change in tear film characteristics in visual display terminal users. Eur. J. Ophthalmol. 2015, 25, 85–89. [Google Scholar] [CrossRef]
- Azmoon, H.; Dehghan, H.; Akbari, J.; Souri, S. The relationship between thermal comfort and light intensity with sleep quality and eye tiredness in shift work nurses. J. Environ. Public Health 2013, 2013, 639184. [Google Scholar] [CrossRef]
- Chawla, A.; Lim, T.C.; Shikhare, S.N.; Munk, P.L.; Peh, W.C.G. Computer vision syndrome: Darkness under the shadow of light. Can. Assoc. Radiol. J. 2019, 70, 5–9. [Google Scholar] [CrossRef]
- Artime Ríos, E.M.; Sánchez Lasheras, F.; Suárez Sánchez, A.; Iglesias-Rodríguez, F.J.; Seguí Crespo, M.M. A Hybrid Algorithm for the Prediction of Computer Vision Syndrome in Health Personnel Based on Trees and Evolutionary Algorithms. In Hybrid Artificial Intelligent Systems, Proceedings of the 13th International Conference (HAIS 2018), Oviedo, Spain, 20–22 June 2018; de Cos Juez, F.J., Villar, J.R., de la Cal, E.A., Herrero, A., Quintián, H., Saéz, J.A., Corchado, E., Eds.; Lecture Notes in Artificial Intelligence; Springer: Cham, Switzerland, 2018; Volume 10870, pp. 597–608. ISBN 978-3-319-92638-4. [Google Scholar]
- García Nieto, P.J.; Álvarez Fernández, J.R.; de Cos Juez, F.J.; Sánchez Lasheras, F.; Díaz Muñiz, C. Hybrid modelling based on support vector regression with genetic algorithms in forecasting the cyanotoxins presence in the Trasona reservoir (Northern Spain). Environ. Res. 2013, 122, 1–10. [Google Scholar] [CrossRef]
- Holland, J.H. Adaptation in Natural and Artificial Systems: An Introductory Analysis with Applications to Biology, Control, and Artificial Intelligence; University of Michigan Press: Ann Arbor, MI, USA, 1975; ISBN 0262082136. [Google Scholar]
- Artime Ríos, E.M.; Seguí Crespo, M.M.; Suarez Sánchez, A.; Suárez Gómez, S.L.; Sánchez Lasheras, F. Genetic algorithm based on support vector machines for computer vision syndrome classification. In Proceedings of the International Joint Conference SOCO’17-CISIS’17-ICEUTE’17, León, Spain, 6–8 September 2017; Pérez García, H., Alfonso-Cendón, J., Sánchez González, L., Quintián, H., Corchado, E., Eds.; Advances in Intelligent Systems and Computing. Springer: Cham, Switzerland, 2018; Volume 649, pp. 381–390, ISBN 978-3-319-67179-6. [Google Scholar]
- Ordóñez Galán, C.; Sánchez Lasheras, F.; de Cos Juez, F.J.; Bernardo Sánchez, A. Missing data imputation of questionnaires by means of genetic algorithms with different fitness functions. J. Comput. Appl. Math. 2017, 311, 704–717. [Google Scholar] [CrossRef]
- Sánchez Lasheras, F.; Suárez Gómez, S.L.; Riesgo García, M.V.; Krzemień, A.; Suárez Sánchez, V. Time series and artificial intelligence with a genetic algorithm hybrid approach for rare earth price prediction. In Proceedings of the International Conference of Time Series (ITISE 2017), Granada, Spain, 18–20 September 2017. [Google Scholar]
- Alonso Fernández, J.R.; Díaz Muñiz, C.; García Nieto, P.J.; de Cos Juez, F.J.; Sánchez Lasheras, F.; Roqueñí, M.N. Forecasting the cyanotoxins presence in fresh waters: A new model based on genetic algorithms combined with the MARS technique. Ecol. Eng. 2013, 53, 68–78. [Google Scholar] [CrossRef]
- Sánchez Lasheras, F.; García Nieto, P.J.; de Cos Juez, F.J.; Mayo Bayón, R.; González Suárez, V.M. A hybrid PCA-CART-MARS-based prognostic approach of the remaining useful life for aircraft engines. Sensors 2015, 15, 7062–7083. [Google Scholar] [CrossRef]
- Tiryaki, B. Estimating rock cuttability using regression trees and artificial neural networks. Rock. Mech. Rock Eng. 2009, 42, 939. [Google Scholar] [CrossRef]
- Cariou, V. Extension of multivariate regression trees to interval data. Application to electriciry load profiling. Comput. Stat. 2006, 21, 325–341. [Google Scholar] [CrossRef]
- Waldmann, P. Genome-wide prediction using Bayesian additive regression trees. Genet. Sel. Evol. 2016, 48, 42. [Google Scholar] [CrossRef] [Green Version]
- Chao, C.M.; Yu, Y.W.; Cheng, B.W.; Kou, Y.L. Construction the model on the breast cancer survival analysis use support vector machine, logistic regression and decision tree. J. Med. Syst. 2014, 38, 106. [Google Scholar] [CrossRef]
- García Nieto, P.J.; García-Gonzalo, E.; Sánchez Lasheras, F.; Alonso Fernández, J.R.; Díaz Muñiz, C.; de Cos Juez, F.J. Cyanotoxin level prediction in a reservoir using gradient boosted regression trees: A case study. Environ. Sci. Pollut. Res. Int. 2018, 25, 22658–22671. [Google Scholar] [CrossRef]
- Varma, S.; Simon, R. Bias in error estimation when using cross-validation for model selection. BMC Bioinf. 2006, 7, 91. [Google Scholar] [CrossRef]
- Artime Ríos, E.M.; Suárez Sánchez, A.; Sánchez Lasheras, F.; Seguí Crespo, M.M. Genetic algorithm based on support vector machines for computer vision syndrome classification in health personnel. Neural Comput. Appl. 2018. [Google Scholar] [CrossRef]
- Robertson, M.M.; Huang, Y.H.; Larson, N. The relationship among computer work, environmental design, and musculoskeletal and visual discomfort: Examining the moderating role of supervisory relations and co-worker support. Int. Arch. Occup. Environ. Health 2016, 89, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Portello, J.K.; Rosenfield, M.; Bababekova, Y.; Estrada, J.M.; Leon, A. Computer-related visual symptoms in office workers. Ophthalmic Physiol. Opt. 2012, 32, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The Osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Ramin, C.; Devore, E.E.; Wang, W.; Pierre-Paul, J.; Wegrzyn, L.R.; Schernhammer, E.S. Night shift work at specific age ranges and chronic disease risk factors. Occup. Environ. Med. 2015, 72, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Gu, F.; Han, J.; Laden, F.; Pan, A.; Caporaso, N.E.; Stampfer, M.J.; Kawachi, I.; Rexrode, K.M.; Willett, W.C.; Hankinson, S.E.; et al. Total and cause-specific mortality of U.S. nurses working rotating night shifts. Am. J. Prev. Med. 2015, 48, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Erren, T.C.; Morfeld, P.; Stork, J.; Knauth, P.; von Mülmann, M.J.; Breitstadt, R.; Müller, U.; Emmerich, M.; Piekarski, C. Shift work, chronodisruption and cancer? The IARC 2007 challenge for research and prevention and 10 theses from the Cologne Colloquium 2008. Scand. J. Work Environ. Health 2009, 35, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Shtein, R.M. Post-LASIK dry eye. Expert Rev. Ophthalmol. 2011, 6, 575–582. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Subjects (n = 343) | No. with CVS (n = 195) | p-Value |
|---|---|---|---|
| Sex | |||
| male | 78 (22.7%) | 37 (47.4%) | 0.056 |
| female | 265 (77.3%) | 158 (59.6%) | |
| Age (years) | |||
| ≤30 | 32 (9.3%) | 16 (50.0%) | 0.062 |
| 31–40 | 73 (21.3%) | 42 (57.5%) | |
| 41–50 | 93 (27.1%) | 62 (66.7%) | |
| 51–60 | 107 (31.2%) | 60 (56.1%) | |
| >60 | 38 (11.1%) | 15 (39.5%) | |
| Hospital | |||
| HMN | 141 (41.1%) | 85 (60.3%) | 0.284 |
| HUCA | 202 (58.9%) | 110 (54.5%) | |
| Ophthalmic lens wearers | |||
| no | 101 (29.4%) | 49 (48.5%) | 0.044 |
| yes | 242 (70.6%) | 146 (60.3%) | |
| Contact lens wearers | |||
| no | 290 (84.5%) | 155 (53.4%) | 0.003 |
| yes | 53 (15.5%) | 40 (75.5%) | |
| Ocular Surgery | |||
| no | 309 (90.1%) | 173 (56.0%) | 0.330 |
| yes | 34 (9.9%) | 22 (64.7%) | |
| Occupational groups | |||
| physicians and surgeons, including residents | 128 (37.3%) | 63 (49.2%) | 0.056 |
| nurses and nurse specialists, including those in training | 164 (47.8%) | 104 (63.4%) | |
| nursing assistants | 51 (14.9%) | 28 (54.9%) | |
| Work schedule | |||
| morning shifts | 133 (38.8%) | 71 (53.4%) | 0.075 |
| evening shifts | 3 (0.9%) | 0 (0.0%) | |
| rotating shifts, without nights | 24 (7.0%) | 14 (58.3%) | |
| rotating shifts, including nights | 100 (29.2%) | 66 (66.0%) | |
| morning shifts plus on-call | 83 (24.2%) | 44 (53.0% | |
| Easy software application | |||
| no | 74 (21.6%) | 39 (52.7%) | 0.416 |
| yes | 269 (78.4%) | 156 (58.0%) | |
| Use of visual display terminals (VDT) at work (hour per day) | |||
| <2 | 27 (7.9%) | 13 (48.1%) | 0.534 |
| 2–4 | 112 (32.7%) | 67 (59.8%) | |
| >4 | 204 (59.5%) | 115 (56.4%) | |
| Use of computer outside work | |||
| no | 55 (16.0%) | 24 (43.6%) | 0.031 |
| yes | 288 (84.0%) | 171 (59.4%) |
| Variables | Percentage of Models |
|---|---|
| Occupational seniority (years) | 97.20% |
| Use of VDT at work (hours per day) | 96.90% |
| Hospital units’ seniority (years) | 96.30% |
| Past history of conjunctivitis | 88.50% |
| Current use of eye drops | 79.80% |
| Rotating Shifts (including nights) | 74.60% |
| Refractive surgery | 74.20% |
| Time as VDT worker (>2 years) | 74.10% |
| Ocular surgery | 69.40% |
| Ophthalmic lens wearers | 64.10% |
| Geriatric department | 60.70% |
| Use of VDT outside work (hours per day) | 60.60% |
| Total VDT use (hours per day) | 60.10% |
| Morning shifts plus on-call | 57.20% |
| Sterilization unit | 53.40% |
| Contact lens wearers | 50.30% |
| Surgery unit | 48.60% |
| Past history of ocular herpes | 46.10% |
| Age | 42.40% |
| Blood bank department | 41.10% |
| Anatomical pathology department | 40.90% |
| Endocrinology unit | 40.70% |
| Morning shifts | 40.50% |
| Sex | 40.20% |
| Traumatology unit | 39.90% |
| Nephrology unit | 39.70% |
| Easy software application | 39.60% |
| Past history of keratitis | 39.30% |
| Anesthesiology department | 34.60% |
| Evening shifts | 34.20% |
| CVS Value | Avg. Difference | n |
|---|---|---|
| 0 | 5.224 | 19 |
| 1 | 4.356 | 24 |
| 2 | 3.855 | 16 |
| 3 | 3.558 | 17 |
| 4 | 2.351 | 38 |
| 5 | 1.587 | 34 |
| 6 | 1.21 | 27 |
| 7 | 0.991 | 27 |
| 8 | 1.671 | 31 |
| 9 | 2.313 | 20 |
| 10 | 2.499 | 24 |
| 11 | 3.27 | 21 |
| 12 | 3.899 | 14 |
| 13 | 5.647 | 8 |
| 14 | 5.204 | 8 |
| 15 | 6.127 | 3 |
| 16 | 9.386 | 7 |
| 17 | 8.816 | 2 |
| 19 | 9.667 | 1 |
| 20 | 9.75 | 1 |
| All | 2.976 | 343 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artime Ríos, E.M.; Sánchez Lasheras, F.; Suárez Sánchez, A.; Iglesias-Rodríguez, F.J.; Seguí Crespo, M.d.M. Prediction of Computer Vision Syndrome in Health Personnel by Means of Genetic Algorithms and Binary Regression Trees. Sensors 2019, 19, 2800. https://doi.org/10.3390/s19122800
Artime Ríos EM, Sánchez Lasheras F, Suárez Sánchez A, Iglesias-Rodríguez FJ, Seguí Crespo MdM. Prediction of Computer Vision Syndrome in Health Personnel by Means of Genetic Algorithms and Binary Regression Trees. Sensors. 2019; 19(12):2800. https://doi.org/10.3390/s19122800
Chicago/Turabian StyleArtime Ríos, Eva María, Fernando Sánchez Lasheras, Ana Suárez Sánchez, Francisco J. Iglesias-Rodríguez, and María del Mar Seguí Crespo. 2019. "Prediction of Computer Vision Syndrome in Health Personnel by Means of Genetic Algorithms and Binary Regression Trees" Sensors 19, no. 12: 2800. https://doi.org/10.3390/s19122800