Validity of Wearable Sensors at the Shoulder Joint: Combining Wireless Electromyography Sensors and Inertial Measurement Units to Perform Physical Workplace Assessments

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
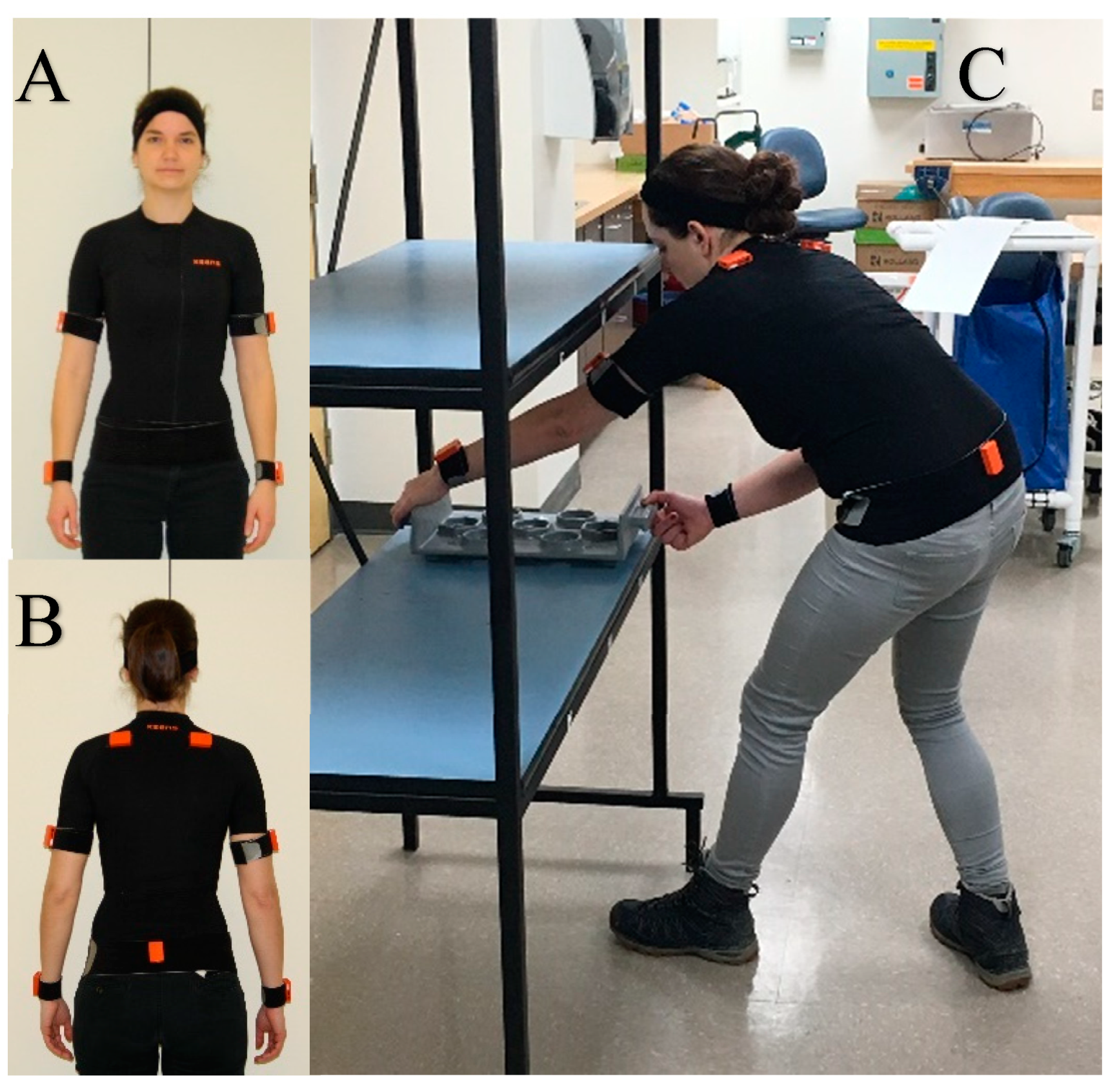
2.2. Instrumentation and Data Collection
2.3. Study Design and Experimental Procedure
2.4. Data Processing
2.5. Statistical Analysis
3. Results
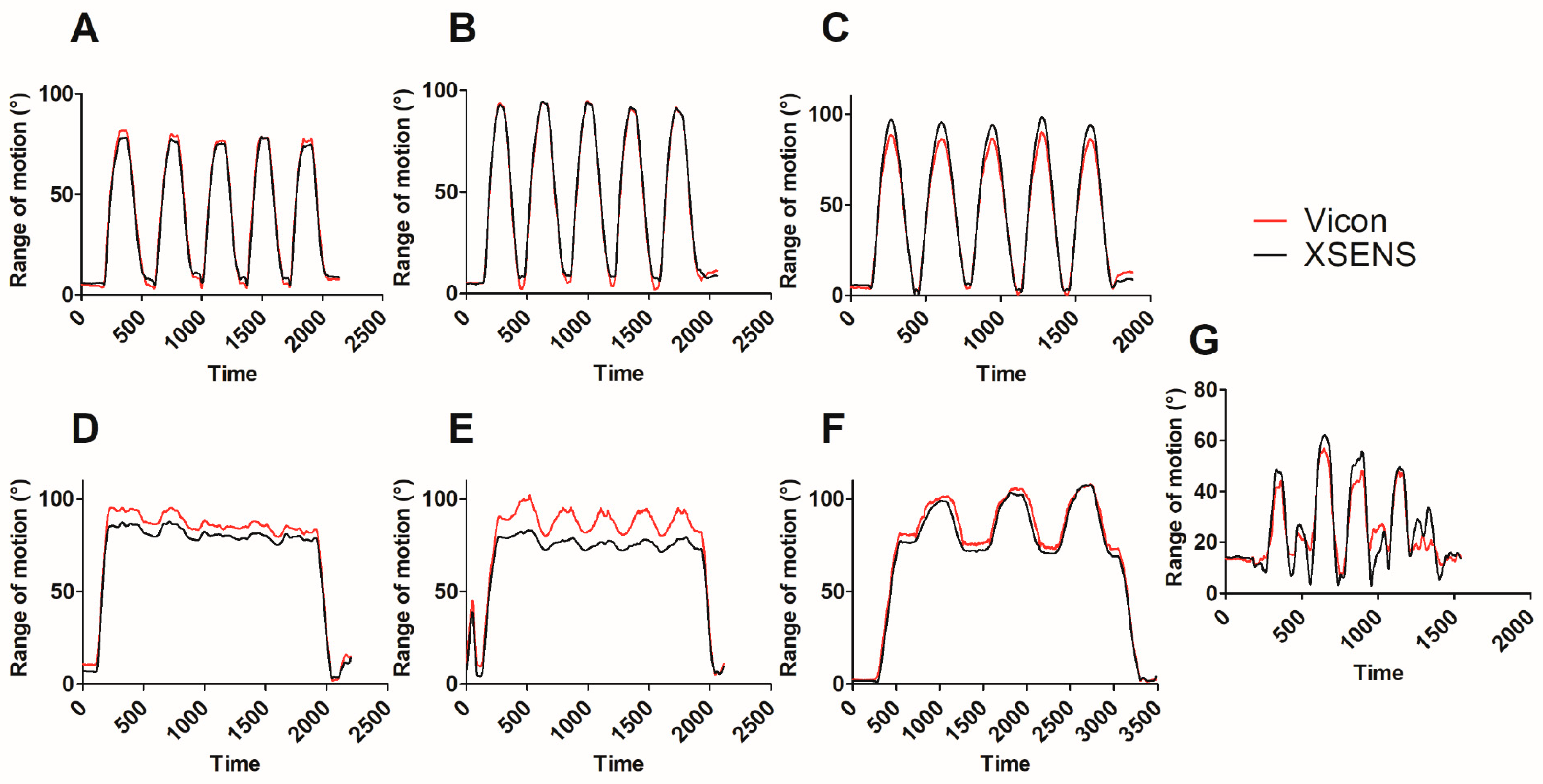
3.1. Kinematic Data
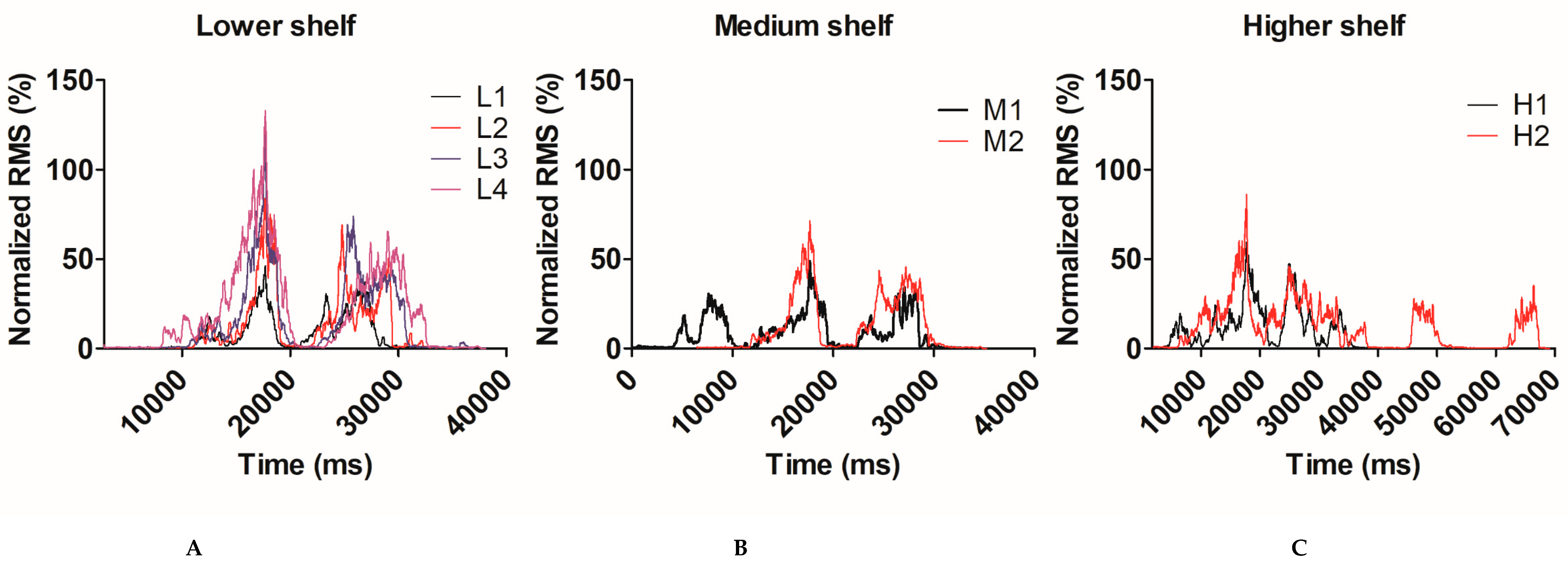
3.2. EMG Activity
3.2.1. Anterior Deltoid
3.2.2. Middle Deltoid
4. Discussion
4.1. Technical Issues to Be Considered Prior to Clinical Implantation
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bongers, P.M.; Ijmker, S.; van den Heuvel, S.; Blatter, B.M. Epidemiology of work related neck and upper limb problems: Psychosocial and personal risk factors (Part I) and effective interventions from a bio behavioural perspective (Part II). J. Occup. Rehabil. 2006, 16, 272–295. [Google Scholar] [CrossRef]
- HSE. Upper Limb Disorders in the Workplace; Health and Safety Executive (HSE): Surrey, UK, 2002; p. 89.
- Linaker, C.H.; Walker-Bone, K. Shoulder disorders and occupation. Best Pract. Res. Clin. Rheumatol. 2015, 29, 405–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, C.A.; Amick Iii, B.C.; Dennerlein, J.T.; Brewer, S.; Catli, S.; Williams, R.; Serra, C.; Gerr, F.; Irvin, E.; Mahood, Q.; et al. Systematic Review of the Role of Occupational Health and Safety Interventions in the Prevention of Upper Extremity Musculoskeletal Symptoms, Signs, Disorders, Injuries, Claims and Lost Time. J. Occup. Rehabil. 2010, 20, 127–162. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder—A systematic review of the literature. Scand. J. Work Environ. Health 2010, 36, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Van der Molen, H.F.; Foresti, C.; Daams, J.G.; Frings-Dresen, M.H.W.; Kuijer, P. Work-related risk factors for specific shoulder disorders: A systematic review and meta-analysis. Occup. Environ. Med. 2017, 74, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Hanvold, T.N.; Wærsted, M.; Mengshoel, A.M.; Bjertness, E.; Veiersted, K.B. Work with prolonged arm elevation as a risk factor for shoulder pain: A longitudinal study among young adults. Appl. Ergon. 2015, 47, 43–51. [Google Scholar] [CrossRef]
- Anglin, C.; Wyss, U.P. Review of arm motion analyses. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2000, 214, 541–555. [Google Scholar] [CrossRef]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Galán-Mercant, A.; Williams, J.M. The use of inertial sensors system for human motion analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef] [Green Version]
- Dejnabadi, H.; Jolles, B.M.; Casanova, E.; Fua, P.; Aminian, K. Estimation and visualization of sagittal kinematics of lower limbs orientation using body-fixed sensors. IEEE Trans. Biomed. Eng. 2006, 53, 1385–1393. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and Reliability of Wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [PubMed]
- Halder, M.A.; Kuhl, G.S.; Zobitz, E.M.; Larson, N.D.; An, N.K. Effects of the Glenoid Labrum and Glenohumeral Abduction on Stability of the Shoulder Joint Through Concavity-Compression: An in Vitro Study. J. Bone Jt. Surg. 2001, 83, 1062–1069. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2016. [Google Scholar] [CrossRef]
- Godwin, A.; Agnew, M.; Stevenson, J. Accuracy of inertial motion sensors in static, quasistatic, and complex dynamic motion. J. Biomech. Eng. 2009, 131, 114501. [Google Scholar] [CrossRef]
- Fantozzi, S.; Giovanardi, A.; Magalhaes, F.A.; Di Michele, R.; Cortesi, M.; Gatta, G. Assessment of three-dimensional joint kinematics of the upper limb during simulated swimming using wearable inertial-magnetic measurement units. J. Sports Sci. 2016, 34, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Ertzgaard, P.; Öhberg, F.; Gerdle, B.; Grip, H. A new way of assessing arm function in activity using kinematic Exposure Variation Analysis and portable inertial sensors—A validity study. Man. Ther. 2016, 21, 241–249. [Google Scholar] [CrossRef]
- Wattanaprakornkul, D.; Cathers, I.; Halaki, M.; Ginn, K.A. The rotator cuff muscles have a direction specific recruitment pattern during shoulder flexion and extension exercises. J. Sci. Med. Sport 2011, 14, 376–382. [Google Scholar] [CrossRef]
- Blache, Y.; Dal Maso, F.; Desmoulins, L.; Plamondon, A.; Begon, M. Superficial shoulder muscle co-activations during lifting tasks: Influence of lifting height, weight and phase. J. Electromyogr. Kinesiol. 2015, 25, 355–362. [Google Scholar] [CrossRef]
- Blache, Y.; Desmoulins, L.; Allard, P.; Plamondon, A.; Begon, M. Effects of height and load weight on shoulder muscle work during overhead lifting task. Ergonomics 2014, 58, 748–761. [Google Scholar] [CrossRef] [PubMed]
- MVN User Manual-User Guide MVN, MVN BIOMECH MVN Link, MVN Awinda; Xsens Technologies B.V.: Enschede, The Netherlands, 2015.
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European Recommendations for Surface Electromyography: Results of the SENIAM Project; Roessingh Research and Development: Enschede, The Netherlands, 1999. [Google Scholar]
- Matheson, L.N. The functional capacity evaluation. In Disability Evaluation; Smith, G.A.S.D.G., Ed.; Mosby Yearbook: Chicago, IL, USA, 2003. [Google Scholar]
- Grabiner, M.D.; Owings, T.M. EMG differences between concentric and eccentric maximum voluntary contractions are evident prior to movement onset. Exp. Brain Res. 2002, 145, 505–511. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukaka, M.M. A guide to appropriate use of Correlation coefficient in medical research. Malawi Med J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Bouvier, B.; Duprey, S.; Claudon, L.; Dumas, R.; Savescu, A. Upper Limb Kinematics Using Inertial and Magnetic Sensors: Comparison of Sensor-to-Segment Calibrations. Sensors 2015, 15, 18813–18833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A.; Sacchetti, R. Ambulatory measurement of shoulder and elbow kinematics through inertial and magnetic sensors. Med. Biol. Eng. Comput. 2008, 46, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Y.; Yen, S.C.; Tay, A.; Lee, W.; Gao, F.; Zhao, Z.; Li, J.; Hon, B.; Xu, T.T.M.; Cheong, A.; et al. Wireless wearable range-of-motion sensor system for upper and lower extremity joints: A validation study. Healthc. Technol. Lett. 2015, 2, 12–17. [Google Scholar] [CrossRef]
- Pérez, R.; Costa, U.; Torrent, M.; Solana, J.; Opisso, E.; Cáceres, C.; Tormos, J.M.; Medina, J.; Gómez, E.J. Upper limb portable motion analysis system based on inertial technology for neurorehabilitation purposes. Sensors 2010, 10, 10733–10751. [Google Scholar] [CrossRef]
- Barraza Madrigal, J.A.; Cardiel, E.; Rogeli, P.; Leija Salas, L.; Munoz Guerrero, R. Evaluation of suitability of a micro-processing unit of motion analysis for upper limb tracking. Med. Eng. Phys. 2016, 38, 793–800. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, H. Reducing drifts in the inertial measurements of wrist and elbow positions. IEEE Trans. Instrum. Meas. 2010, 59, 575–585. [Google Scholar] [CrossRef]
- Silvetti, A.; Mar, S.; Ranavolo, A.; Forzano, F.; Iavicoli, S.; Conte, C.; Draicchio, F. Kinematic and electromyographic assessment of manual handling on a supermarket green grocery shelf. Work 2015, 51, 261–271. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Effect of local magnetic field disturbances on inertial measurement units accuracy. Appl. Erg. 2017, 63, 123–132. [Google Scholar] [CrossRef]
- Kolber, M.J.; Hanney, W.J. The reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer: A technical report. Int. J. Sports Phys. 2012, 7, 306–313. [Google Scholar]
- Ligorio, G.; Zanotto, D.; Sabatini, A.M.; Agrawal, S.K. A novel functional calibration method for real-time elbow joint angles estimation with magnetic-inertial sensors. J. Biomech. 2017, 54, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Van der Windt, D.A.; Koes, B.W.; de Jong, B.A.; Bouter, L.M. Shoulder disorders in general practice: Incidence, patient characteristics, and management. Ann. Rheum. Dis. 1995, 54, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.L.; Halaki, M.; Ginn, K.A. The use of surface electrodes to record infraspinatus activity is not valid at low infraspinatus activation levels. J. Electromyogr. Kinesiol. 2011, 21, 112–118. [Google Scholar] [CrossRef]
- Nieminen, H.; Takala, E.P.; Niemi, J.; Viikari-Juntura, E. Muscular synergy in the shoulder during a fatiguing static contraction. Clin. Biomech. 1995, 10, 309–317. [Google Scholar] [CrossRef]
- Minning, S.; Eliot, C.A.; Uhl, T.L.; Malone, T.R. EMG analysis of shoulder muscle fatigue during resisted isometric shoulder elevation. J. Electromyogr. Kinesiol. 2007, 17, 153–159. [Google Scholar] [CrossRef]
- Hawkes, D.H.; Alizadehkhaiyat, O.; Kemp, G.J.; Fisher, A.C.; Roebuck, M.M.; Frostick, S.P. Electromyographic assessment of muscle fatigue in massive rotator cuff tear. J. Electromyogr. Kinesiol. 2015, 25, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Movement/Task | Range of Motion (°)/Movement Combined | r (Mean [SD]) | RMSE Arm Elevation (Mean [SD]) (°) | Average Error of Estimate (Mean [SD]) (°) |
|---|---|---|---|---|
| Flexion | 60 | 0.968 [0.066] | 5.17 [2.81] | 4.38 [2.26] |
| 90 | 0.998 [0.002] | 4.67 [2.95] | 3.86 [2.33] | |
| 120 | 0.997 [0.003] | 6.21 [3.90] | 4.97 [3.01] | |
| Abduction | 60 | 0.998 [0.001] | 2.77 [1.28] | 2.37 [1.13] |
| 90 | 0.999 [0.0003] | 3.75 [2.86] | 2.97 [2.18] | |
| 120 | 0.999 [0.0004] | 4.92 [3.02] | 3.95 [2.35] | |
| Scaption | 60 | 0.997 [0.002] | 3.95 [2.89] | 3.17 [2.16] |
| 90 | 0.998 [0.001] | 5.16 [4.12] | 4.18 [3.45] | |
| 120 | 0.999 [0.001] | 6.72 [4.20] | 5.46 [3.53] | |
| Trunk movements | Anterior flexion | 0.974 [0.057] | 7.05 [3.81] | 6.08 [3.53] |
| Lateral bending | 0.970 [0.041] | 11.63 [5.56] | 9.72 [4.85] | |
| Rotation | 0.917 [0.099] | 12.82 [7.61] | 10.15 [6.12] | |
| Complex tasks | Mean | 0.846 [0.103] | 11.48 [2.42] | 9.18 [2.02] |
| Lower shelf | 0.851 [0.111] | 9.62 [3.79] | 7.77 [2.99] | |
| Medium shelf | 0.840 [0.087] | 11.33 [4.04] | 9.03 [3.01] | |
| Higher shelf | 0.870 [0.057] | 12.68 [2.96] | 10.24 [2.35] | |
| p-value | 0.621 | 0.067 | 0.054 |
| L1 | L2 | L3 | L4 | M1 | M2 | H1 | H2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Anterior deltoid | RMS (% of MVC) | Mean | 32.41 | 49.60 | 67.86 | 90.70 | 45.97 | 65.88 | 64.90 | 119.38 |
| SD | 10.85 | 35.67 | 37.00 | 58.02 | 40.89 | 40.31 | 24.32 | 44.66 | ||
| Peak EMG activity (% of MVC) | Mean | 37.93 | 65.45 | 75.71 | 87.35 | 39.91 | 54.02 | 56.66 | 87.28 | |
| SD | 13.05 | 44.40 | 42.11 | 50.49 | 30.79 | 35.68 | 17.90 | 34.74 | ||
| Middle deltoid | RMS (% of MVC) | Mean | 35.13 | 43.16 | 34.04 | 46.63 | 32.92 | 55.52 | 50.83 | 100.87 |
| SD | 28.39 | 32.20 | 40.91 | 44.91 | 32.51 | 46.14 | 32.17 | 62.23 | ||
| Peak EMG activity (% of MVC) | Mean | 38.84 | 50.08 | 47.55 | 53.86 | 27.63 | 43.64 | 41.39 | 68.50 | |
| SD | 29.15 | 42.58 | 38.14 | 36.28 | 23.21 | 33.61 | 26.19 | 40.30 | ||
| One-Way ANOVA p-value | One-Way ANOVA η2 | Two-Way ANOVA p-value | Two-Way ANOVA η2 | Post-Hoc Analysis | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L1 vs L2 | L1 vs L3 | L1 vs L4 | L1 vs M1 | L1 vs H1 | L2 vs M2 | L2 vs H2 | L2 vs L3 | L2 vs L4 | L3 vs L4 | M1 vs M2 | M1 vs H1 | M2 vs H2 | H1 vs H2 | |||||||
| Anterior deltoid | RMS (p-value) | Weight effect | <0.001 | 0.505 | <0.001 | 0.889 | ||||||||||||||
| Height effect | - | - | <0.001 | 0.480 | ||||||||||||||||
| Weight x Height effect | - | - | 0.001 | 0.361 | 0.003 | 0.001 | <0.001 | 0.042 | 0.197 | 0.928 | <0.001 | 0.021 | <0.001 | 0.03 | 0.124 | 0.678 | <0.001 | <0.001 | ||
| Peak EMG activity (p-value) | Weight effect | <0.001 | 0.460 | 0.001 | 0.540 | |||||||||||||||
| Height effect | - | - | 0.003 | 0.317 | ||||||||||||||||
| Weight x Height effect | - | - | 0.001 | 0.383 | 0.077 | 0.001 | <0.001 | 0.012 | 0.793 | 0.764 | 0.002 | 0.115 | 0.001 | 0.102 | 0.361 | 0.011 | <0.001 | <0.001 | ||
| Middle deltoid | RMS (p-value) | Weight effect | 0.159 | 0.917 | 0.002 | 0.523 | ||||||||||||||
| Height effect | - | - | 0.028 | 0.241 | ||||||||||||||||
| Weight x Height | - | - | 0.003 | 0.352 | 0.143 | 0.791 | 0.626 | 0.302 | 0.834 | 0.723 | 0.002 | 0.754 | 0.810 | 0.576 | 0.378 | 0.325 | 0.004 | <0.001 | ||
| Peak EMG activity (p-value) | Weight effect | 0.244 | 0.093 | 0.121 | 0.163 | |||||||||||||||
| Height effect | - | - | 0.539 | 0.037 | ||||||||||||||||
| Weight x Height | - | - | 0.001 | 0.388 | 0.647 | 0.274 | 0.027 | 0.206 | 0.194 | 0.788 | 0.013 | 0.783 | 0.562 | 0.383 | 0.408 | 0.054 | 0.015 | 0.001 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poitras, I.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity of Wearable Sensors at the Shoulder Joint: Combining Wireless Electromyography Sensors and Inertial Measurement Units to Perform Physical Workplace Assessments. Sensors 2019, 19, 1885. https://doi.org/10.3390/s19081885
Poitras I, Bielmann M, Campeau-Lecours A, Mercier C, Bouyer LJ, Roy J-S. Validity of Wearable Sensors at the Shoulder Joint: Combining Wireless Electromyography Sensors and Inertial Measurement Units to Perform Physical Workplace Assessments. Sensors. 2019; 19(8):1885. https://doi.org/10.3390/s19081885
Chicago/Turabian StylePoitras, Isabelle, Mathieu Bielmann, Alexandre Campeau-Lecours, Catherine Mercier, Laurent J. Bouyer, and Jean-Sébastien Roy. 2019. "Validity of Wearable Sensors at the Shoulder Joint: Combining Wireless Electromyography Sensors and Inertial Measurement Units to Perform Physical Workplace Assessments" Sensors 19, no. 8: 1885. https://doi.org/10.3390/s19081885