Microgrooves and Microrugosities in Titanium Implant Surfaces: An In Vitro and In Vivo Evaluation

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
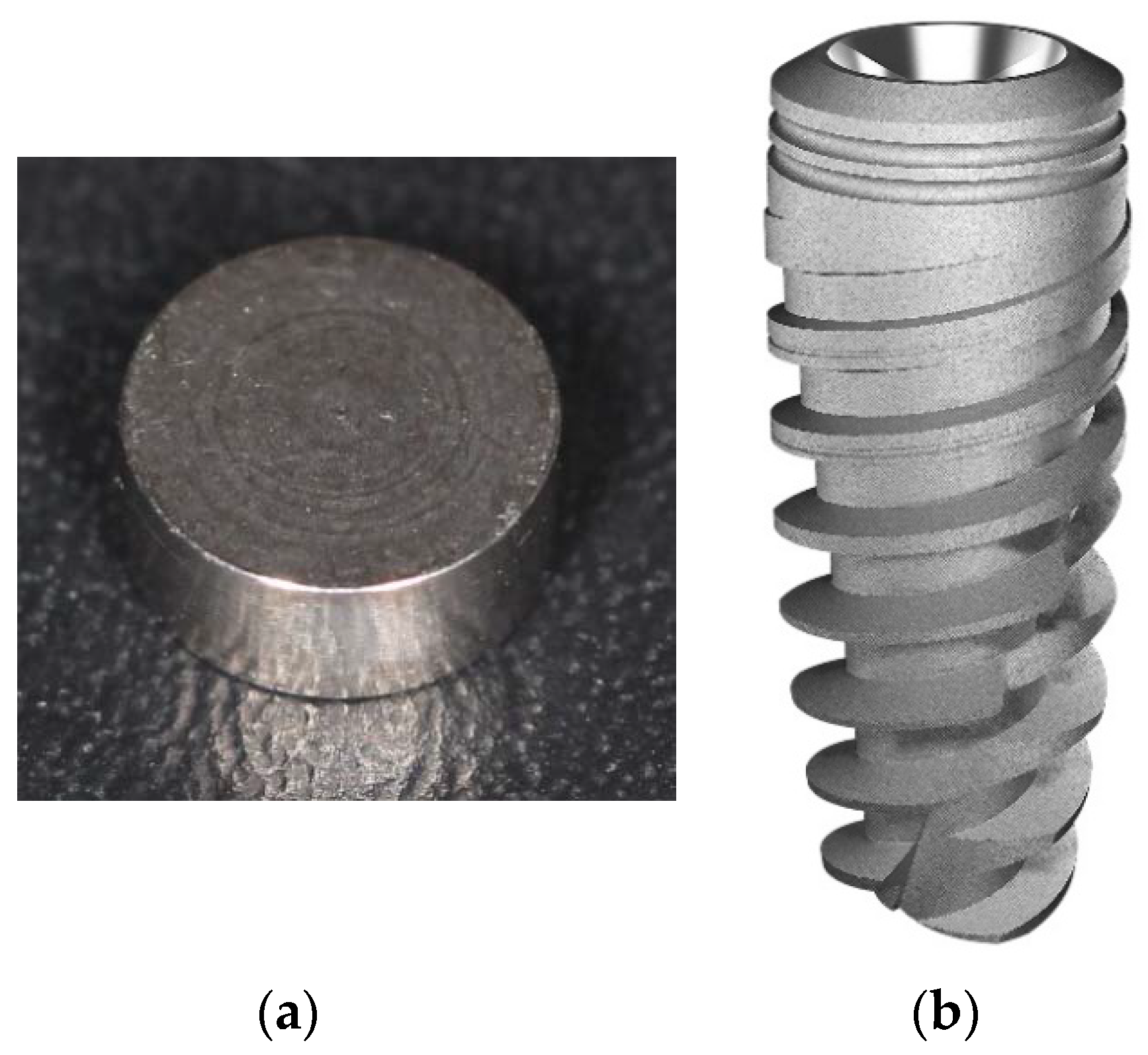
2. Materials and Methods
3. Results
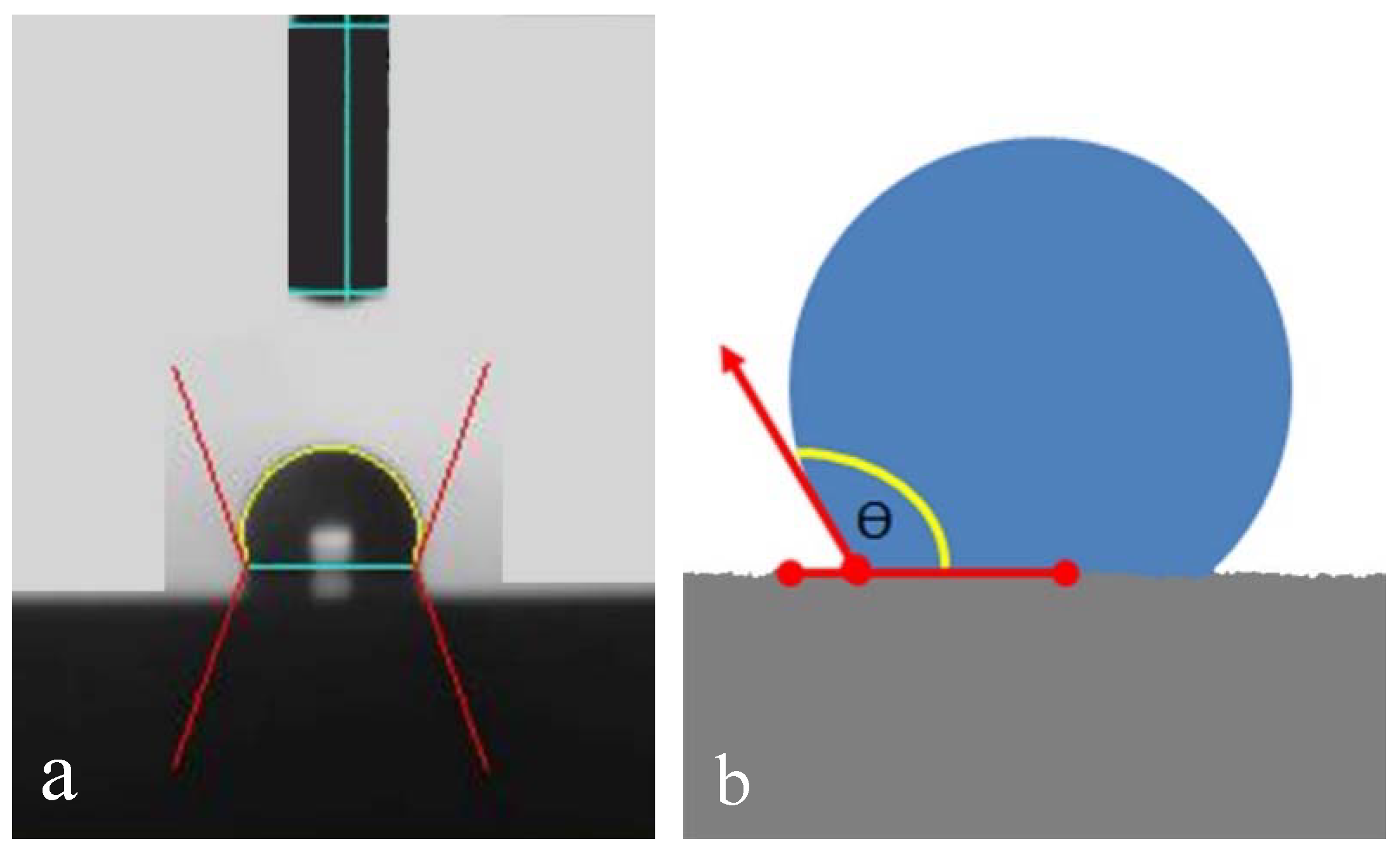
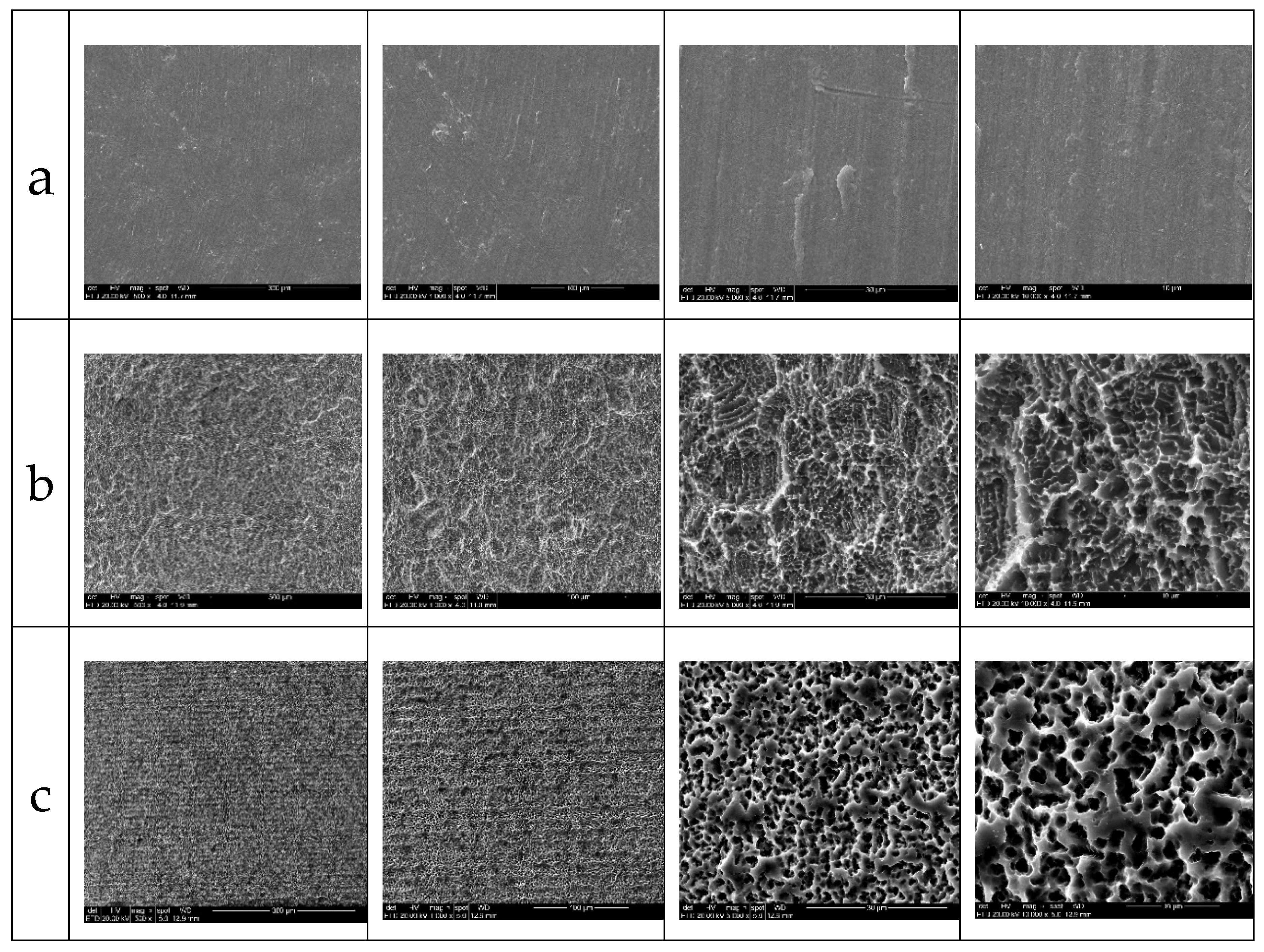
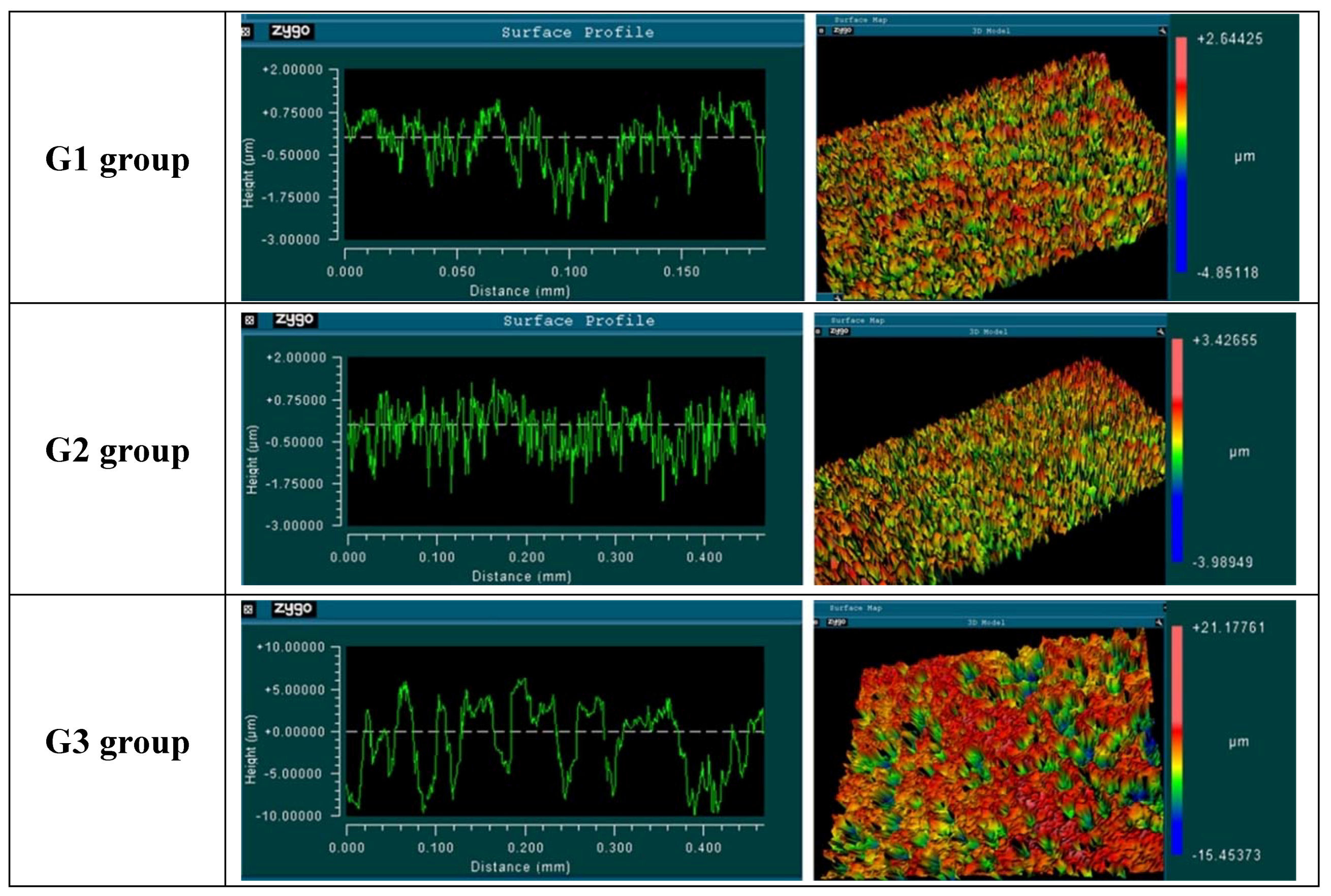
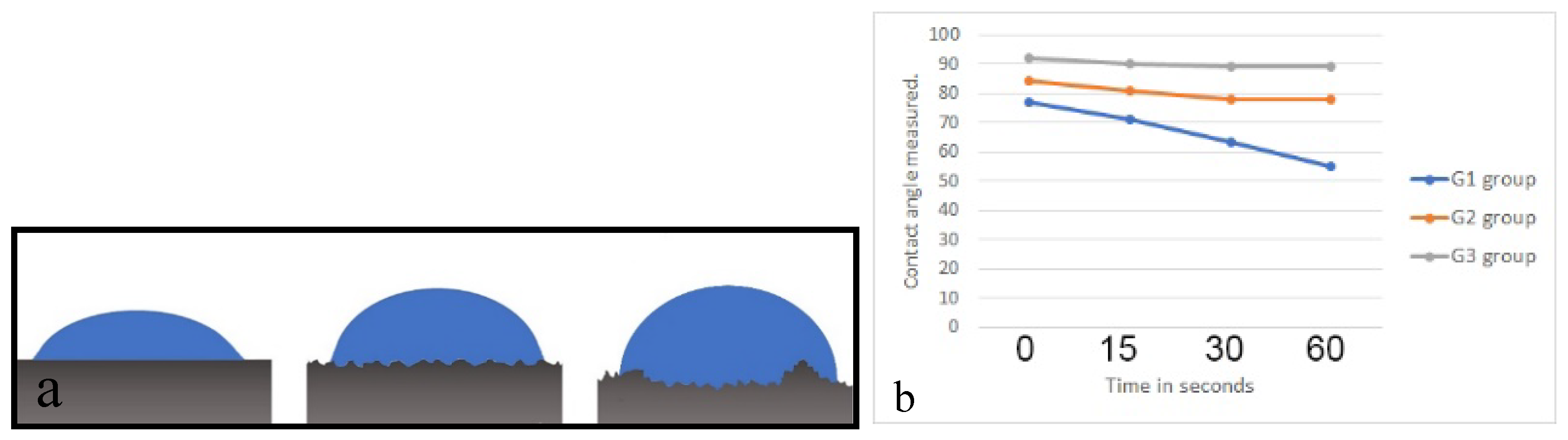
3.1. In Vitro Characterization of the Surfaces
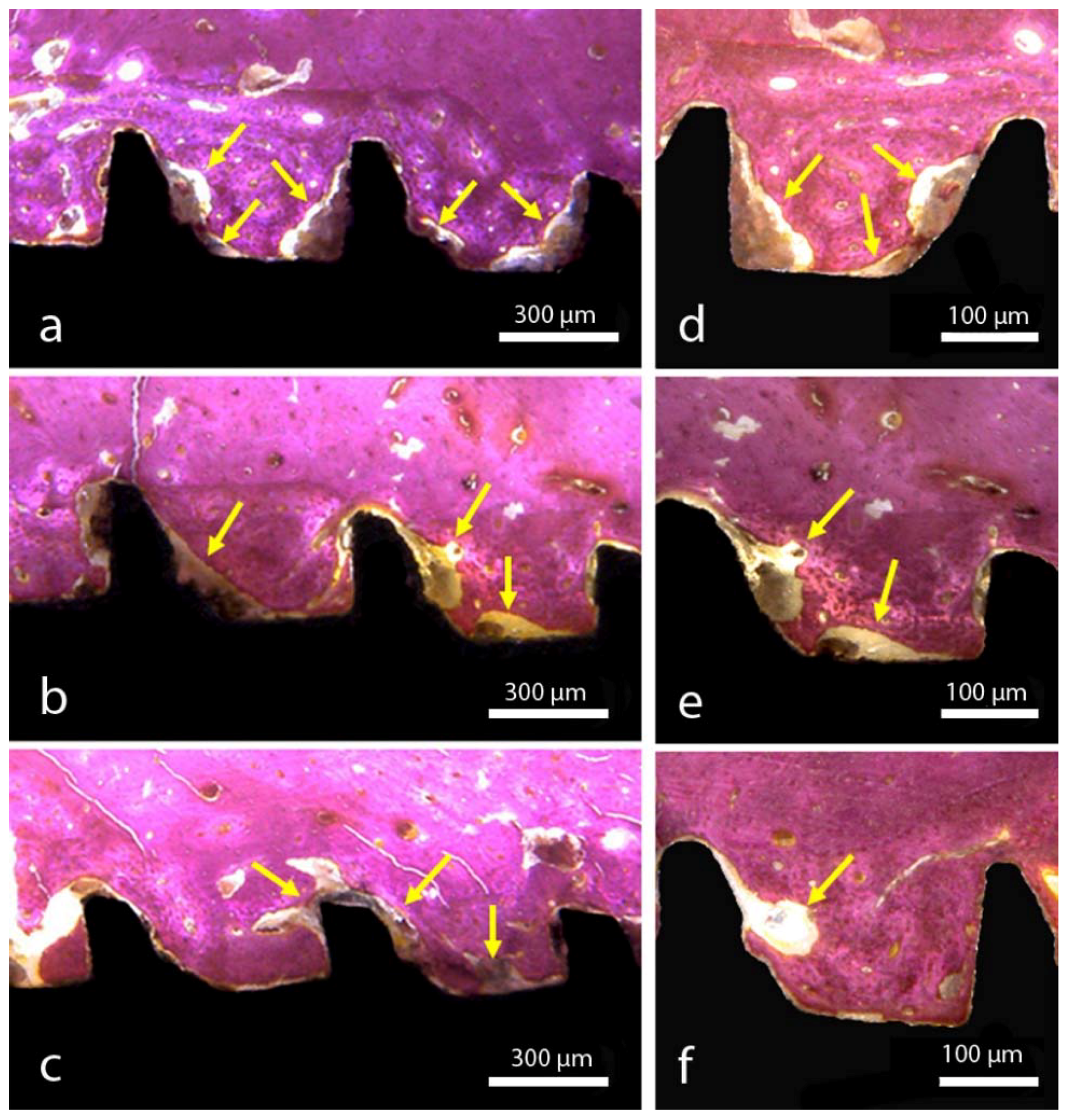
3.2. Histomorphological Analysis and Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gehrke, S.A.; Prados-Frutos, J.C.; Prados-Privado, M.; Calvo-Guirado, J.L.; Aramburú Júnior, J.; Pérez-Díaz, L.; Mazón, P.; Aragoneses, J.M.; De Aza, P.N. Biomechanical and Histological Analysis of Titanium (Machined and Treated Surface) Versus Zirconia Implant Materials: An In Vivo Animal Study. Materials 2019, 12, 856. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Dedavid, B.A.; Aramburú, J.S., Jr.; Pérez-Díaz, L.; Calvo Guirado, J.L.; Canales, P.M.; De Aza, P.N. Effect of Different Morphology of Titanium Surface on the Bone Healing in Defects Filled Only with Blood Clot: A New Animal Study Design. BioMed Res. Int. 2018, 2018, 4265474. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Bettach, R.; Aramburú, J.S., Jr.; Prados-Frutos, J.C.; Del Fabbro, M.; Shibli, J.A. Peri-Implant Bone Behavior after Single Drill versus Multiple Sequence for Osteotomy Drill. BioMed Res. Int. 2018, 2018, 9756043. [Google Scholar] [CrossRef]
- Orsini, G.; Piattelli, M.; Scarano, A.; Petrone, G.; Kenealy, J.; Piattelli, A.; Caputi, S. Randomized, controlled histologic and histomorphometric evaluation of implants with nanometer-scale calcium phosphate added to the dual acid-etched surface in the human posterior maxilla. J. Periodontol. 2007, 78, 209–218. [Google Scholar] [CrossRef]
- Alshammari, Y.; Yang, F.; Bolzoni, L. Mechanical properties and microstructure of Ti-Mn alloys produced via powder metallurgy for biomedical applications. J. Mech. Behav. Biomed. Mater. 2019, 91, 391–397. [Google Scholar] [CrossRef]
- Li, Y.; Yang, C.; Zhao, H.; Qu, S.; Li, X.; Li, Y. New Developments of Ti-Based Alloys for Biomedical Applications. Materials 2014, 7, 1709–1800. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.A.; Jung, S.K. A removal torque of the laser-treated titanium implants in rabbit tibia. Biomaterials 2003, 24, 4859–4863. [Google Scholar] [CrossRef]
- Gotfredsen, K.; Berglundh, T.; Lindhe, J. Bone reactions adjacent to titanium implants with different surface characteristics subjected to static load. A study in the dog (II). Clin. Oral Implants Res. 2001, 12, 196–201. [Google Scholar] [CrossRef]
- Torensma, R.; Ter Brugge, P.J.; Jansen, J.A.; Figdor, C.G. Ceramic hydroxyapatite coating on titanium implants drives selective bone marrow stromal cell adhesion. Clin. Oral Implants Res. 2003, 14, 569–577. [Google Scholar] [CrossRef]
- Gaggl, A.; Schultes, G.; Muller, W.D.; Karcher, H. Scanning electron microscopical analysis of laser-treated titanium implant surfaces—A comparative study. Biomaterials 2000, 21, 1067–1073. [Google Scholar] [CrossRef]
- Hallgren, C.; Reimers, H.; Chakarov, D.; Gold, J.; Wennerberg, A. An in vivo study of bone response to implants topographically modified by laser micromachining. Biomaterials 2003, 24, 701–710. [Google Scholar] [CrossRef]
- Novaes, A.B., Jr.; de Souza, S.L.; de Barros, R.R.; Pereira, K.K.; Iezzi, G.; Piattelli, A. Influence of implant surfaces on osseointegration. Braz. Dent. J. 2010, 21, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Gittens, R.A.; Olivares-Navarrete, R.; Cheng, A.; Anderson, D.M.; McLachlan, T.; Stephan, I.; Geis-Gerstorfer, J.; Sandhage, K.H.; Fedorov, A.G.; Rupp, F.; et al. The roles of titanium surface micro/nanotopography and wettability on the differential response of human osteoblast lineage cells. Acta Biomater. 2013, 9, 6268–6277. [Google Scholar] [CrossRef]
- Lukaszewska-Kuska, M.; Wirstlein, P.; Majchrowski, R.; Dorocka-Bobkowska, B. Osteoblastic cell behaviour on modified titanium surfaces. Micron 2018, 105, 55–63. [Google Scholar] [CrossRef]
- Soboyejo, W.O.; Nemetski, B.; Allameh, S.; Marcantonio, N.; Mercer, C.; Ricci, J. Interactions between MC3T3-E1 cells and textured Ti6Al4V surfaces. J. Biomed. Mater. Res. 2002, 62, 56–72. [Google Scholar] [CrossRef]
- Gotfredsen, K.; Nimb, L.; Hjörting-Hansen, E.; Jensen, J.S.; Holmén, A. Histomorphometric and removal torque analysis for TiO2-blasted titanium implants. An experimental study on dogs. Clin. Oral Implants Res. 1992, 3, 77–84. [Google Scholar] [CrossRef]
- Klokkevold, P.R.; Nishimura, R.D.; Adachi, M.; Caputo, A. Osseointegration enhanced by chemical etching of the titanium surface. A torque removal study in the rabbit. Clin. Oral Implants Res. 1997, 8, 442–447. [Google Scholar] [CrossRef]
- Cooper, L.F. A role for surface topography in creating and maintaining bone at titanium endosseous implants. J. Prosthet. Dent. 2000, 84, 522–534. [Google Scholar] [CrossRef]
- Frenkel, S.R.; Simon, J.; Alexander, H.; Dennis, M.; Ricci, J.L. Osseointegration on metallic implant surfaces: Effects of microgeometry and growth factor treatment. J. Biomed. Mater. Res. 2002, 63, 706–713. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Zizzari, V.L.; Iaculli, F.; Mortellaro, C.; Tetè, S.; Piattelli, A. Relationship between the surface energy and the histologic results of different titanium surfaces. J. Craniofac. Surg. 2014, 25, 863–867. [Google Scholar] [CrossRef]
- Song, E.Y.; Yoon, J.; Yoon, J.; Lee, M.; Lee, S.W.; Oh, N. The effect of microgrooves on osseointegration of titanium surfaces in rabbit calvaria. Tissue Eng. Regen. Med. 2013, 10, 347–352. [Google Scholar] [CrossRef]
- Sun, L.; Pereira, D.; Wang, Q.; Barata, D.B.; Truckenmüller, R.; Li, Z.; Xu, X.; Habibovic, P. Controlling Growth and Osteogenic Differentiation of Osteoblasts on Microgrooved Polystyrene Surfaces. PLoS ONE 2016, 11, e0161466. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Aoyama, T.; Yasuda, T.; Oike, M.; Ito, A.; Tajino, J.; Nagai, M.; Fujioka, R.; Iijima, H.; Yamaguchi, S.; et al. Effect of microfabricated microgroove-surface devices on the morphology of mesenchymal stem cells. Biomed. Microdevices 2015, 17, 116. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Lee, J.; Lee, J.T.; Hong, J.S.; Lim, B.S.; Park, H.J.; Kim, Y.K.; Kim, T.I. Microgrooves on titanium surface affect peri-implant cell adhesion and soft tissue sealing; an in vitro and in vivo study. J. Periodontal Implant Sci. 2015, 45, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Bereznai, M.; Pelsoczi, I.; Toth, Z.; Turzo, K.; Radnai, M.; Bor, Z.; Fazekas, A. Surface modifications induced by ns and sub-ps excimer laser pulses on titanium implant material. Biomaterials 2003, 24, 4197–4203. [Google Scholar] [CrossRef]
- Pérez del Pino, A.; Serra, P.; Morenza, J.L. Oxidation of titanium Through Nd:YAG laser irradiation. Appl. Surf. Sci. 2002, 197, 887–890. [Google Scholar] [CrossRef]
- Davies, J.E. Mechanisms of endosseous integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar]
- Schneirder, G.B.; Zaharias, R.; Seabold, D.; Keller, J.; Stanford, C. Differentiation of preosteoblasts is affected by implant surface microtopographies. J. Biomed. Mater. Res. A 2004, 69, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Grassi, S.; De Figueiredo, L.C.; Feres, M.; Marcantonio, E., Jr.; Iezzi, G.; Piattelli, A. Influence of implant surface topography on early osseointegration: A histological study in human jaws. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 80, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Aoki, K.; Ohya, K. Effects of surface roughness of titanium implants on bone remodeling activity of femur in rabbits. Bone 1997, 21, 507–514. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 2—review focusing on clinical knowledge of different surfaces. Int. J. Prosthodontics 2004, 17, 544–564. [Google Scholar]
- Kubiak, K.J.; Wilson, M.C.T.; Mathia, T.G.; Carval, P. Wettability versus roughness of engineering surfaces. Wear 2011, 271, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Buser, D.; Broggini, N.; Wieland, M.; Schenk, R.K.; Denzer, A.J.; Cochran, D.L.; Hoffmann, B.; Lussi, A.; Steinemann, S.G. Enhanced bone apposition to a chemically modified SLA titanium surface. J. Dent. Res. 2004, 83, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Gottlow, J.; Barkarmo, S.; Sennerby, L. An experimental comparison of two different clinically used implant designs and surfaces. Clin. Implant Dent. Relat. Res. 2012, 14, 204–212. [Google Scholar] [CrossRef]
- Sartoretto, S.C.; Alves, A.T.; Resende, R.F.; Calasans-Maia, J.; Granjeiro, J.M.; Calasans-Maia, M.D. Early osseointegration driven by the surface chemistry and wettability of dental implants. J. Appl. Oral Sci. 2015, 23, 279–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implants Res. 2011, 22, 349–356. [Google Scholar] [CrossRef]
- Shanbhag, S.; Shanbhag, V.; Stavropoulos, A. Genomic analyses of early periimplant bone healing in humans: A systematic review. Int. J. Implant Dent. 2015, 1, 5. [Google Scholar] [CrossRef]
- Wenzel, R.N. Resistance of solid surfaces to wetting by water. Ind. Eng. Chem. 1936, 28, 988–994. [Google Scholar] [CrossRef]
- Cassie, A.B.D.; Baxter, S. Wettability of porous surfaces. Trans. Faraday Soc. 1944, 40, 546–551. [Google Scholar] [CrossRef]
- Kulkarni, M.; Patil-Sen, Y.; Junkar, I.; Kulkarni, C.V.; Lorenzetti, M.; Iglič, A. Wettability studies of topologically distinct titanium surfaces. Colloids Surf. B Biointerfaces 2015, 129, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implants Res. 2009, 20, 172–184. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
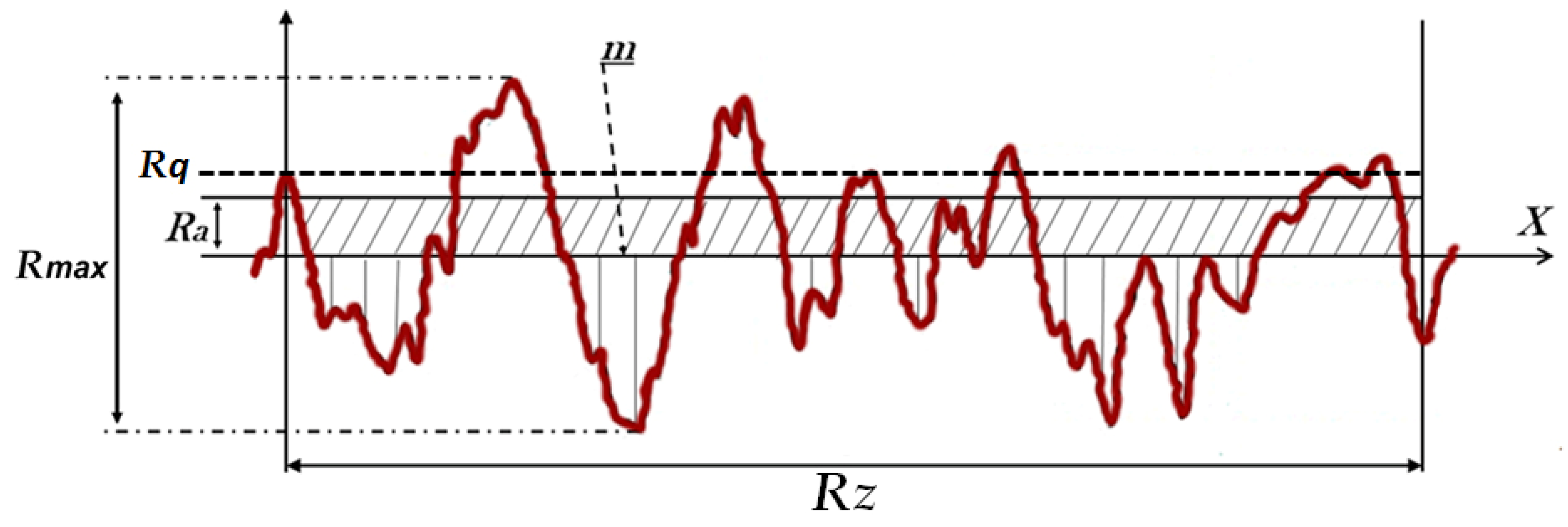
| Parameters | Ra (µm) | Rq (µm) | Rz (µm) | Rmax (µm) | |
|---|---|---|---|---|---|
| Group | |||||
| G1 | 0.56 ± 0.02 | 0.75 ± 0.12 | 5.96 ± 0.42 | 7.91 ± 0.95 | |
| G2 | 0.66 ± 0.05 | 0.78 ± 0.10 | 4.77 ± 0.58 | 6.77 ± 0.52 | |
| G3 | 0.67 ± 0.05 | 0.81 ± 0.07 | 11.02 ± 0.59 | 19.02 ± 0.88 | |
| p-value (ANOVA) | 0.0081 | 0.7318 | 0.0022 | 0.0045 | |
| Variables | BIC (%) | BAFO (%) | ||
|---|---|---|---|---|
| Group | Mean ± SD | Median | Mean ± SD | Median |
| G1 | 50.45 ± 9.67 | 50.60 | 54.87 ± 9.56 | 54.86 |
| G2 | 55.32 ± 10.31 | 55.51 | 59.09 ± 10.13 | 59.15 |
| G3 | 68.65 ± 9.98 | 68.83 | 70.12 ± 11.07 | 70.33 |
| Statistic | p-value | -- | p-value | -- |
| G1 × G2 | 0.2438 | -- | 0.3078 | -- |
| G1 × G3 | <0.0001 * | -- | 0.0005 * | -- |
| G2 × G3 | 0.0033 * | -- | 0.0109 * | -- |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gehrke, S.A.; Cavalcanti de Lima, J.H.; Rodriguez, F.; Calvo-Guirado, J.L.; Aramburú Júnior, J.; Pérez-Díaz, L.; Mazón, P.; Aragoneses, J.M.; De Aza, P.N. Microgrooves and Microrugosities in Titanium Implant Surfaces: An In Vitro and In Vivo Evaluation. Materials 2019, 12, 1287. https://doi.org/10.3390/ma12081287
Gehrke SA, Cavalcanti de Lima JH, Rodriguez F, Calvo-Guirado JL, Aramburú Júnior J, Pérez-Díaz L, Mazón P, Aragoneses JM, De Aza PN. Microgrooves and Microrugosities in Titanium Implant Surfaces: An In Vitro and In Vivo Evaluation. Materials. 2019; 12(8):1287. https://doi.org/10.3390/ma12081287
Chicago/Turabian StyleGehrke, Sergio Alexandre, José Henrique Cavalcanti de Lima, Fernando Rodriguez, José Luis Calvo-Guirado, Jaime Aramburú Júnior, Leticia Pérez-Díaz, Patricia Mazón, Juan Manuel Aragoneses, and Piedad N. De Aza. 2019. "Microgrooves and Microrugosities in Titanium Implant Surfaces: An In Vitro and In Vivo Evaluation" Materials 12, no. 8: 1287. https://doi.org/10.3390/ma12081287