Primary Health Care Center (PHCC) Location-Allocation with Multi-Objective Modelling: A Case Study in Idleb, Syria


Abstract
:1. Introduction
2. Materials and Methods
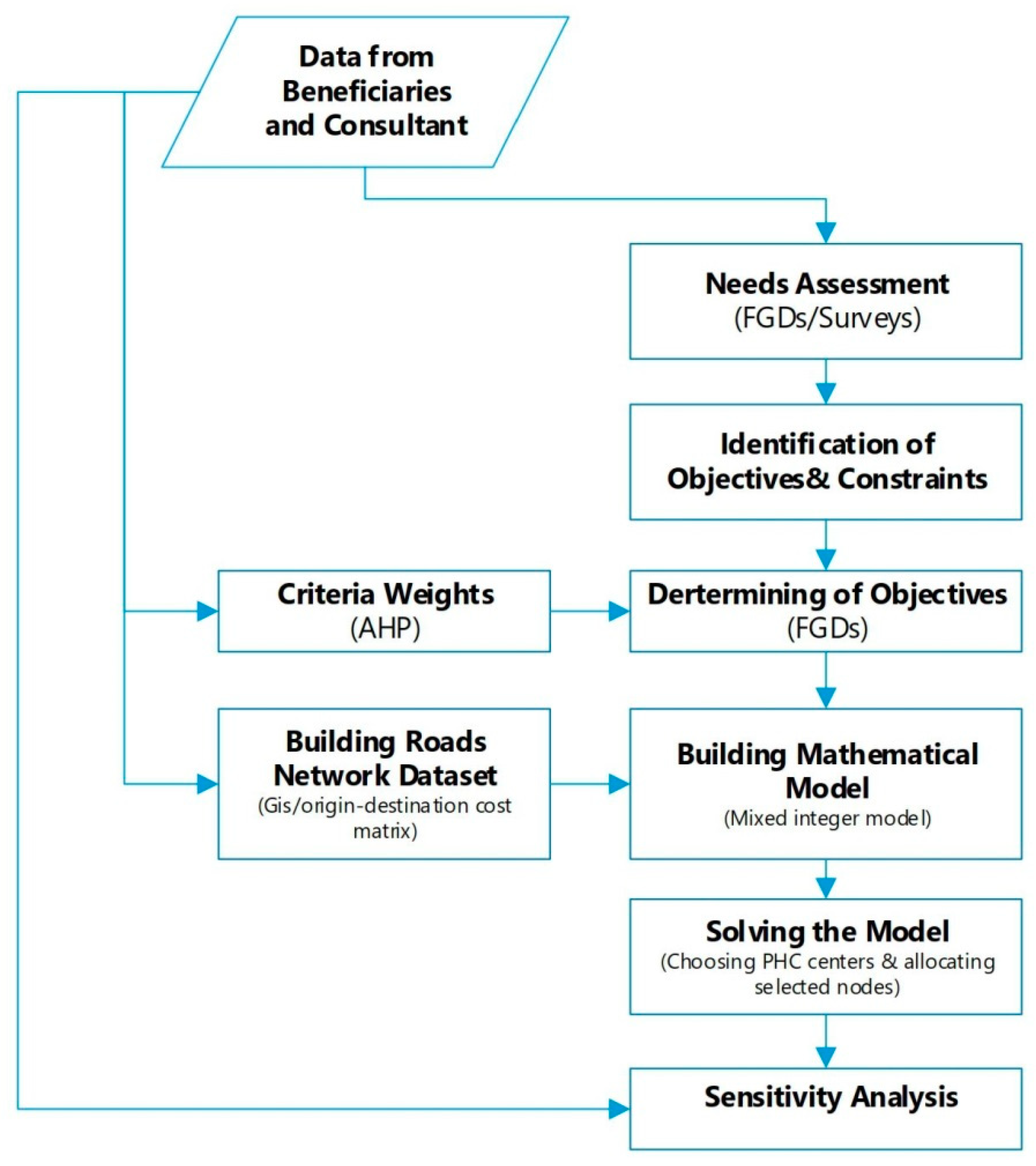
2.1. Methodology
2.2. Building the Model
- Laboratory service,
- Blood grouping service,
- Vaccination,
- Solar power,
- Basement,
- Internet service.
- Each demand node can be served as an entire unit from a PHCC or not served at all (0 or 1 without any fraction).
- Amount of each demand and its location are fixed.
- Paths throughout the updated built road networks are accessible and there is no broken or closed street.
- Variable costs for each allocated group of people at each location are related to the amount of people allocated in the PHCC irrespective of the PHCC’s location. It means that the cost of allocating a person to a certain PHCC is the same cost of allocating him/her to another PHCC in another location.
2.3. Weighted Goal Programming (WGP)
2.4. Analytic Hierarchy Process (AHP) for Identifying Criteria Weights in WGP
2.5. Weighted Goal Programming Formulation
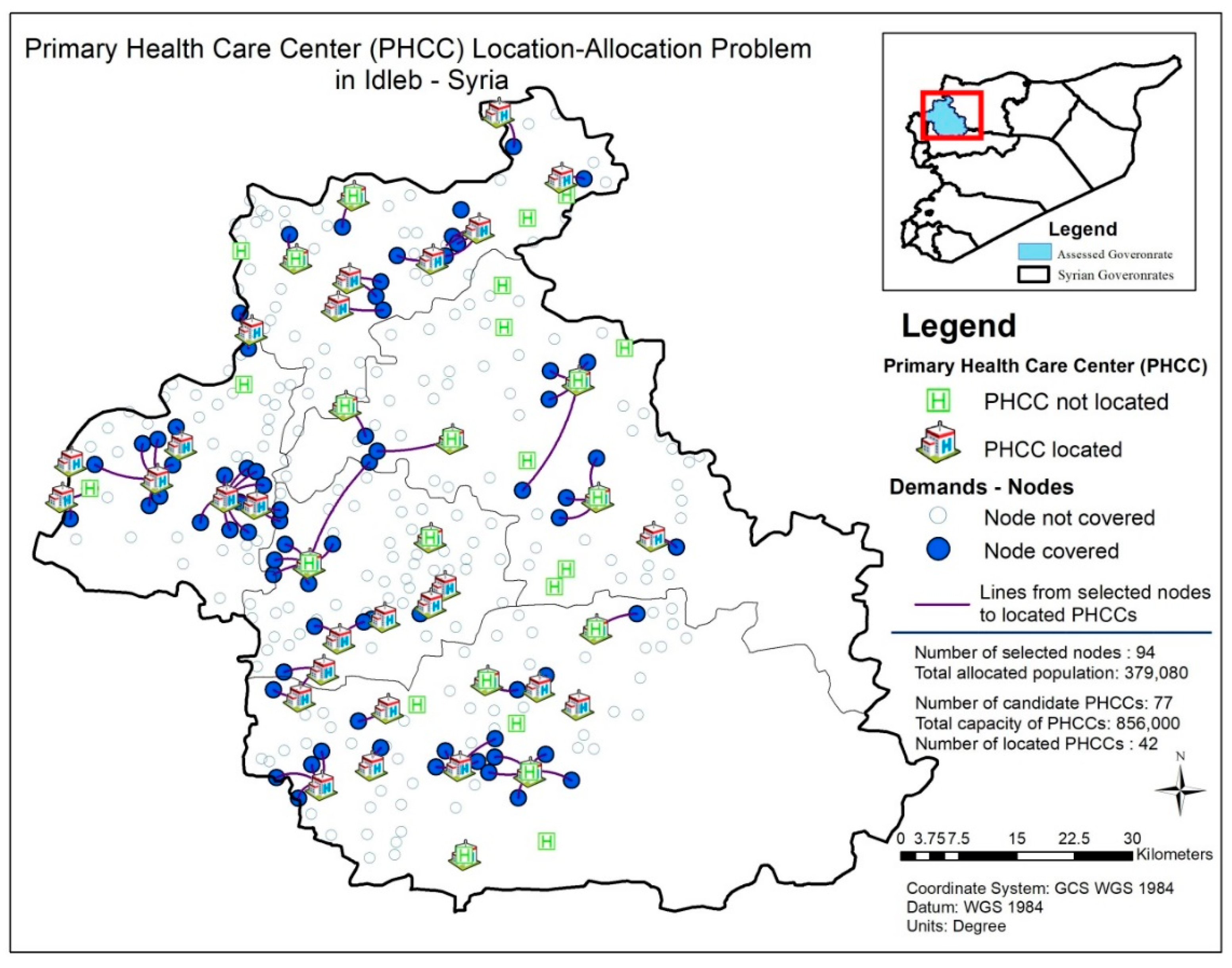
3. Case Study and Results
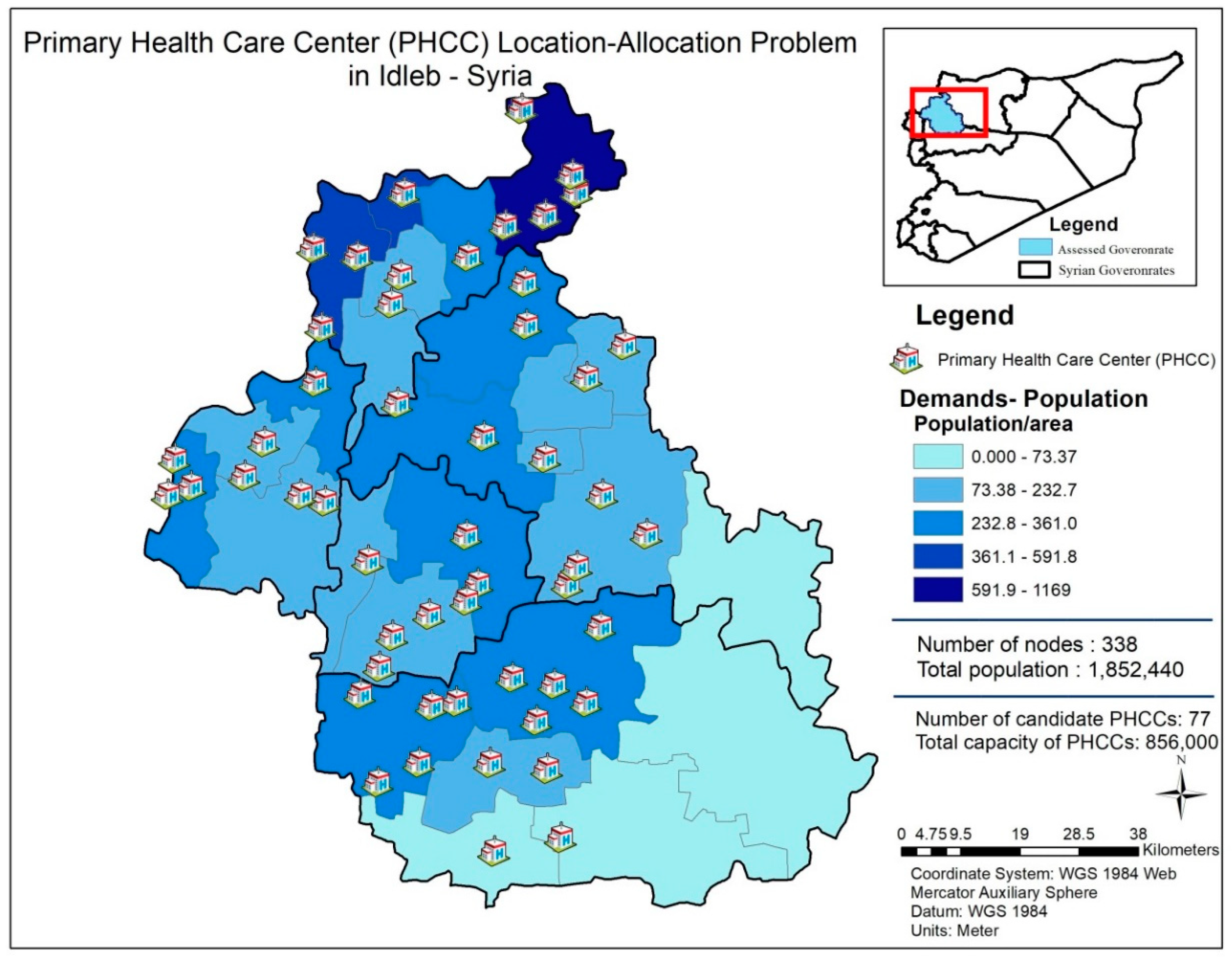
3.1. Case Study
- Demands at nodes;
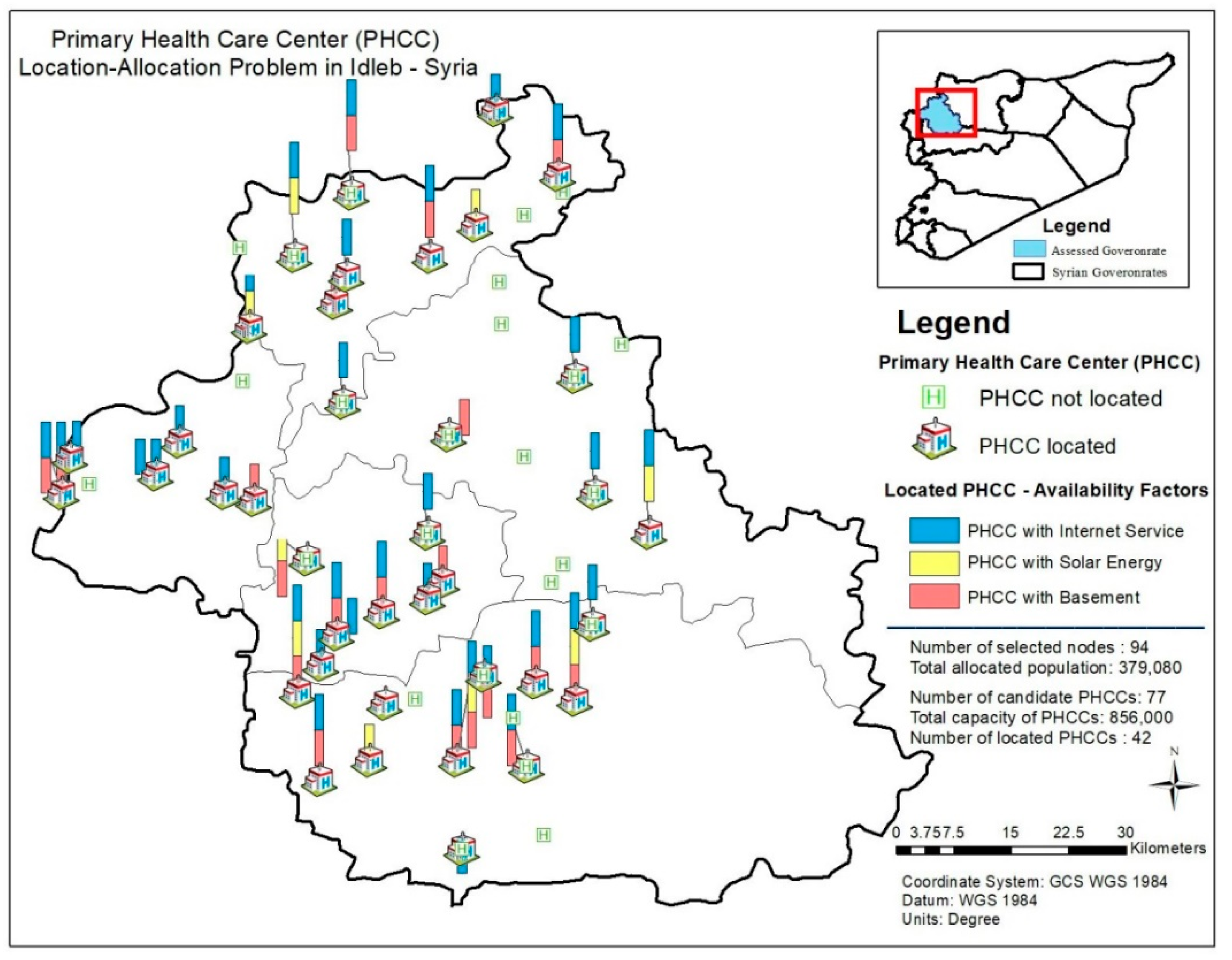
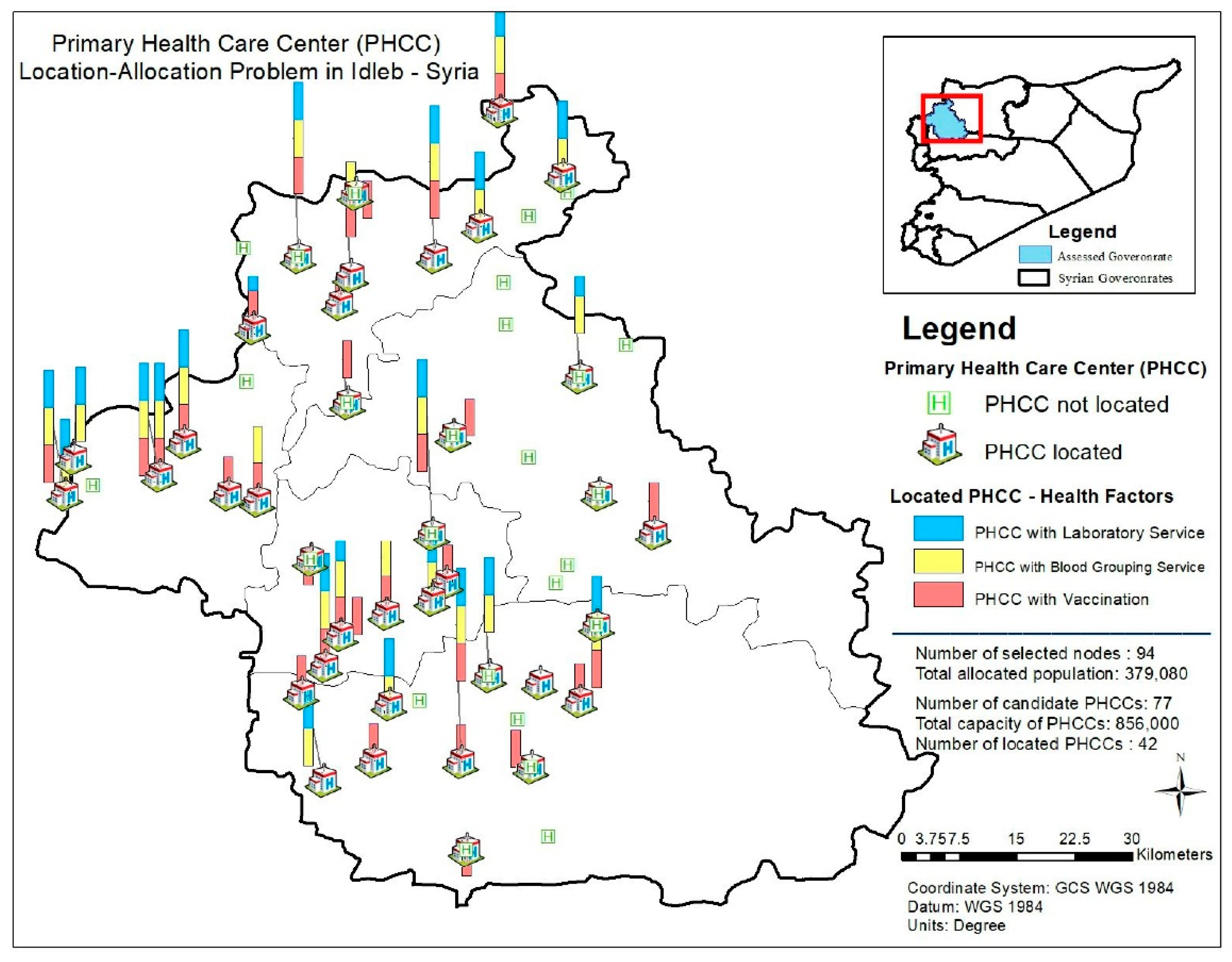
- Availability factors of candidate PHCCs (solar power, basement, internet service, laboratory service, blood grouping service and vaccination);
- Coverage distance;
- Fixed cost of locating a PHCC at candidate locations;
- Capacity of each candidate location;
- Cash for work amount at each candidate location.
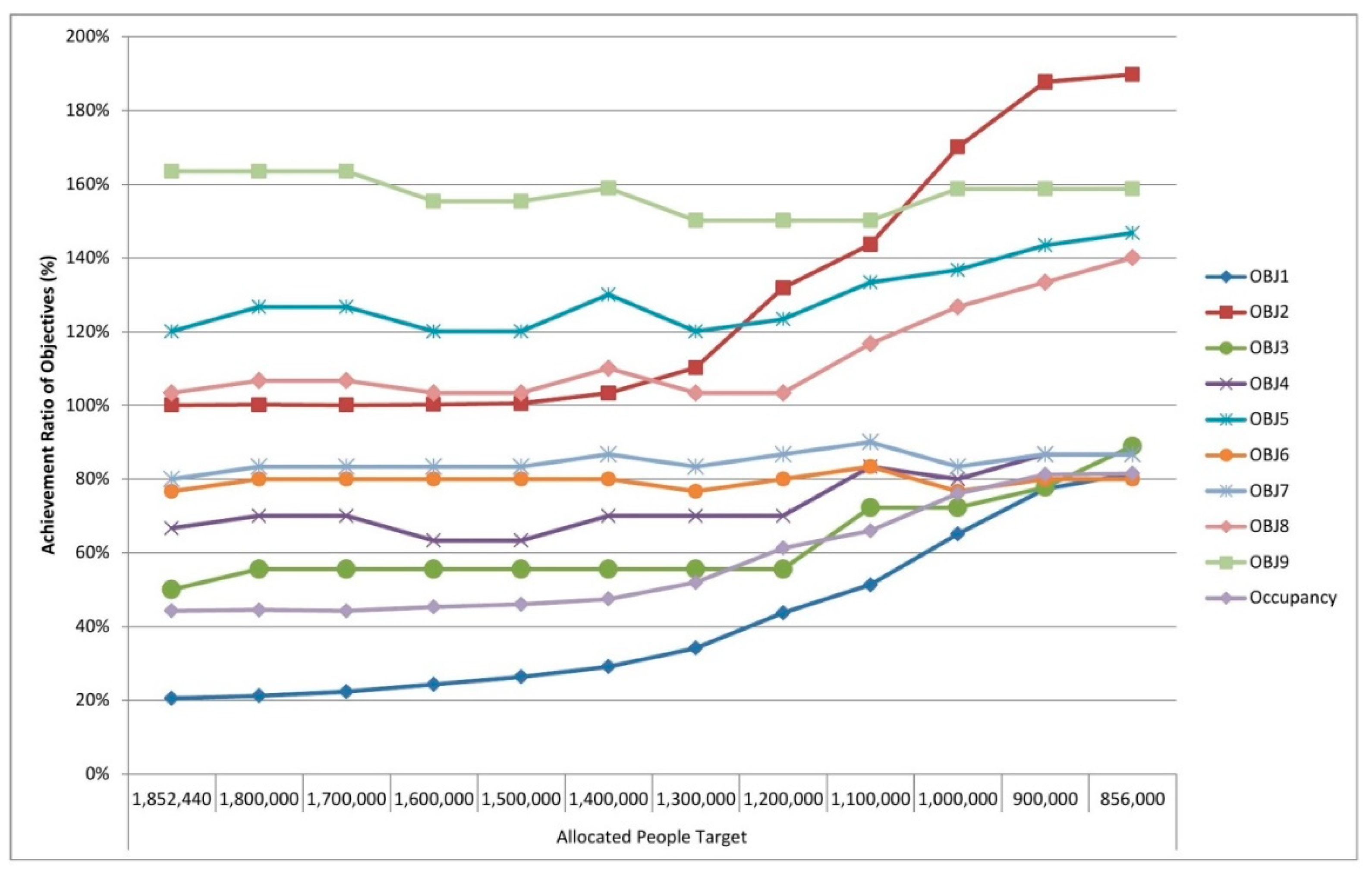
- Regarding the RHS of our first objective, the target value of allocated people, we have set our target value as 1,852,440 following data collection since we aim to allocate all people in the case study area.
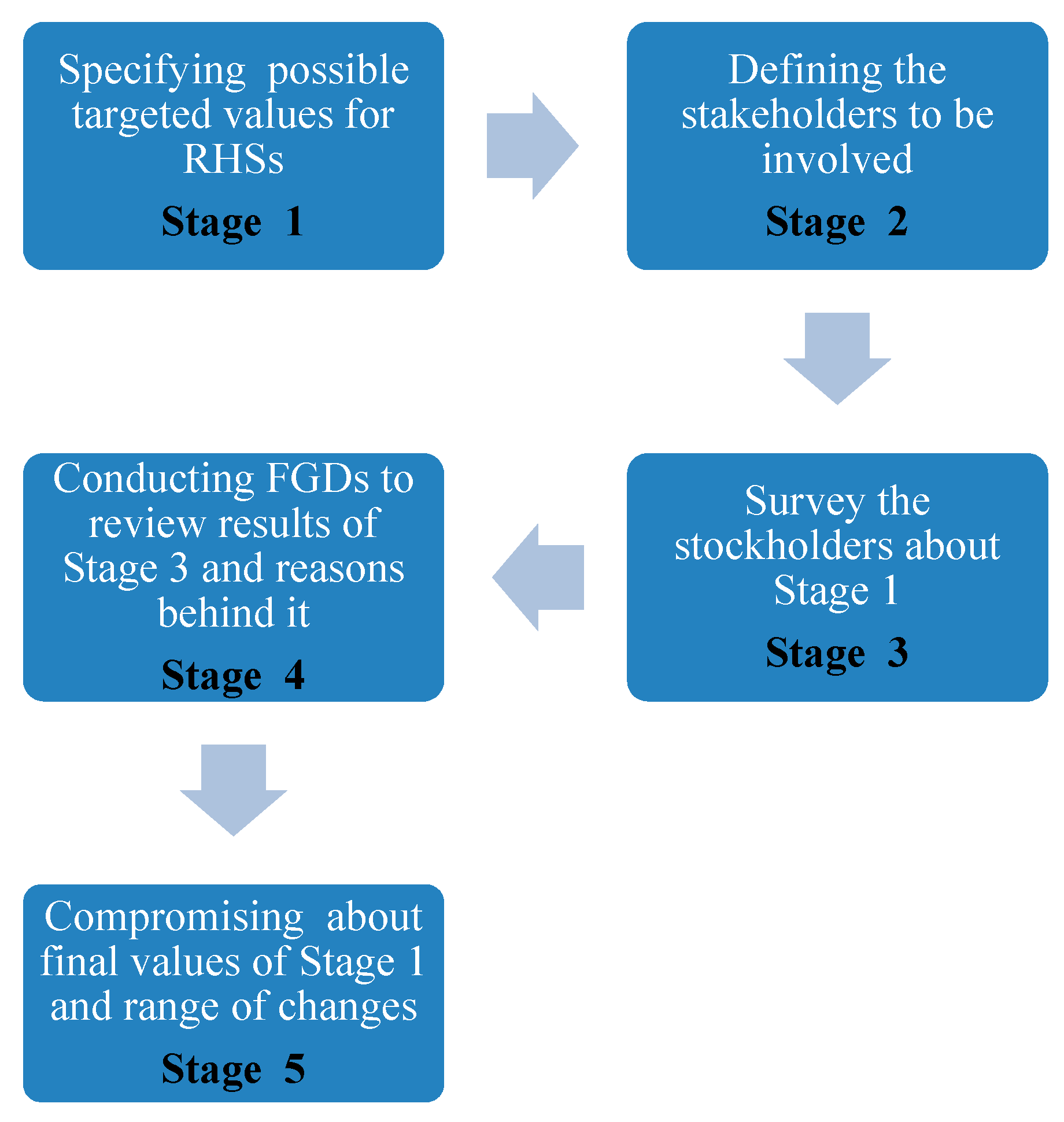
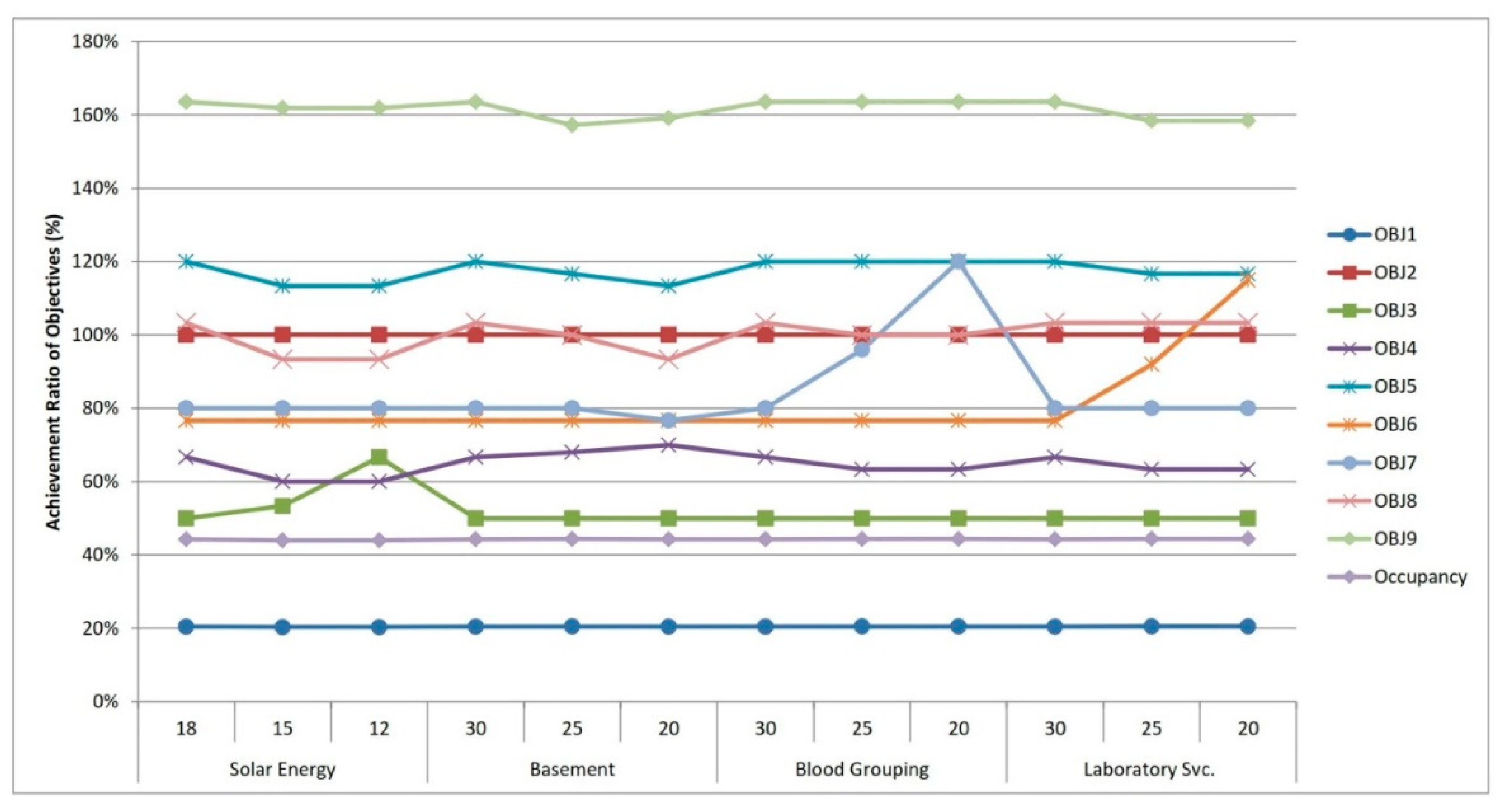
- Among candidate PHCCs; 31 have laboratory service, 33 have blood grouping service, 60 have vaccination, 18 have solar power, 36 have basement and 65 have internet service. Through the process in Figure 3, we determined these objective’s target values as: 30, 30, 30, 18, 30 and 30, respectively.
- According to the results obtained by AHP and depicted with Table 3; for every objective function(n); values are set as: 45, 0, 5, 5, 5, 5, 5, 9 and 9. values are set as: 0, 14, 0, 0, 0, 0, 0, 0 and 0. Here, goals though 1 to 9 correspond to: allocated people objective, total cost objective, cash for work, solar power, basement, internet service, laboratory service, blood grouping service and vaccination, respectively.
- Total cost budget and cash for work target values are determined as USD 1,000,000 and USD 100,000 via the process in Figure 3.
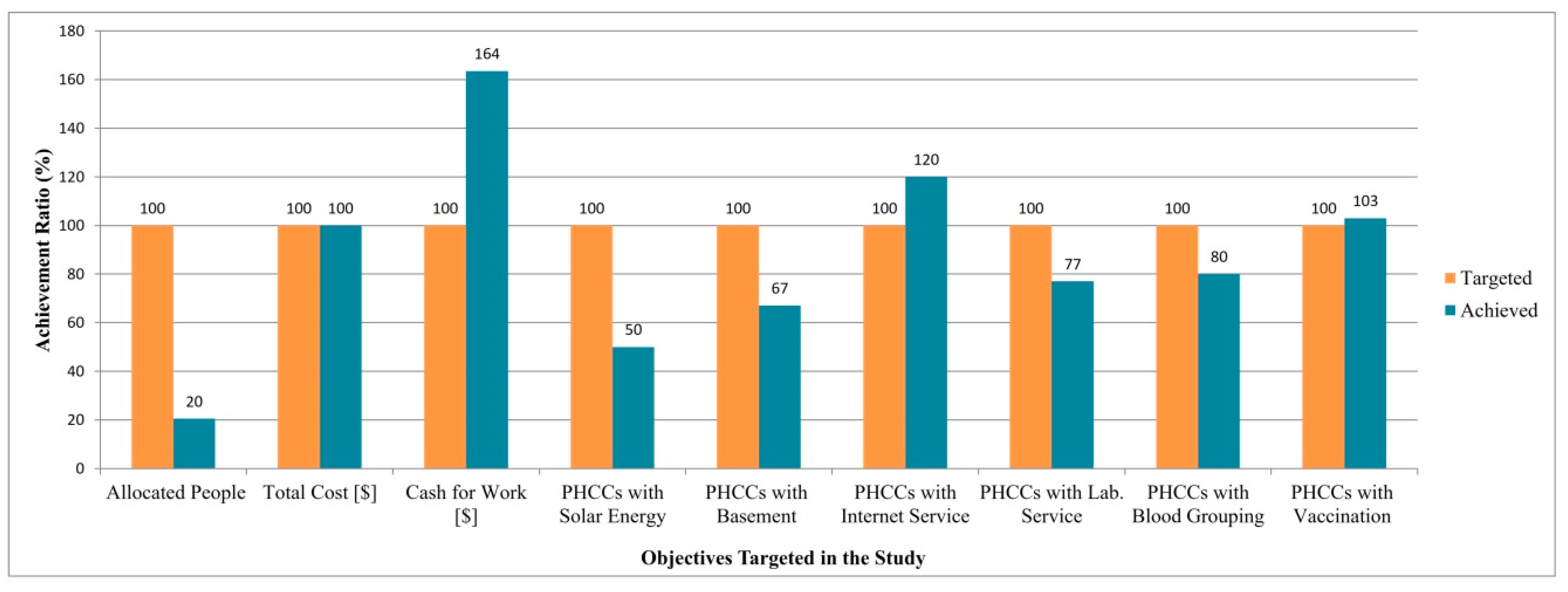
3.2. Results
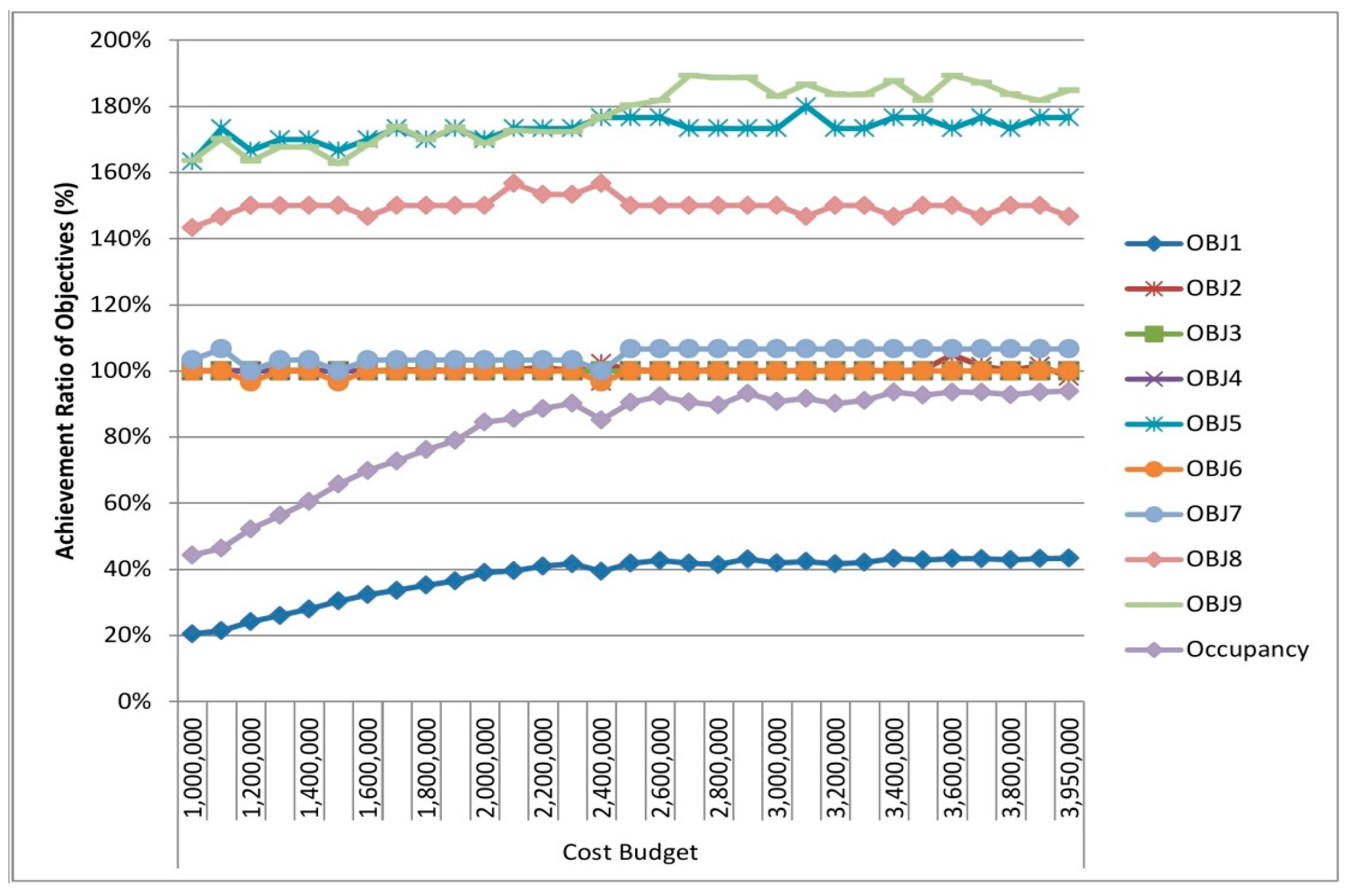
3.3. Sensitivity Analysis
4. Discussion
- PHCCs or health care facilities can be assessed with more criteria such as the availability of running water and availability of electricity in hours.
- Criteria such as education, access to food and water can also be handled alongside the criteria/objectives addressed in this study.
- In future studies, labor factors (doctors, nurses, technicians and guards) and medical resources (beds, drugs, etc.) can be included in the model.
- Sensitivity analyses can be performed by changing multiple parameters simultaneously.
- Other regions of Syria can also be added into the relevant area, which can make the paper more comprehensive.
- A web-based tool can be designed incorporating the mathematical model and GIS and adapted to various similar problems.
- A dynamic model might be proposed to deal with the high degree of uncertainty regarding such problems.
- The problem can be handled by different techniques such as heuristic, meta-heuristic methods, hybrid models and social simulations.
- A conflict risk assessment can be applied to investigate the connection between the risk of armed conflict/ongoing crisis and a set of indicators such as education, infrastructure and access to health care facilities and food.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- UNISDR. Terminology: Basic Terms of Disaster Risk Reduction; United Nations Office for Disaster Risk Reduction: Geneva, Switzerland, 2017; Available online: http://www.unisdr.org/we/inform/terminology (accessed on 23 November 2018).
- UNHCR. Global Trends: Forced Displacement in 2017; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2017; Available online: https://www.unhcr.org/5b27be547.pdf (accessed on 23 November 2018).
- Sweileh, W.M. Bibliometric analysis of medicine–related publications on refugees, asylum-seekers, and internally displaced people: 2000–2015. BMC Int. Health Hum. R. 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Beiser, M. The health of immigrants and refugees in Canada. Can. J. Public Health 2005, 96, 30–44. [Google Scholar]
- WHO. Risk Reduction and Emergency Preparedness: WHO Six-Year Strategy for the Health Sector and Community Capacity Development; World Health Organization: Geneva, Switzerland, 2007; Available online: https://www.who.int/hac/techguidance/preparedness/emergency_preparedness_eng.pdf (accessed on 23 November 2018).
- Panos, E.; Dafni, P.; Kostas, G.; Zacharoula, M. Crisis management in the Health Sector; qualities and characteristics of health crisis managers. Int. J. Caring Sci. 2009, 2, 105–107. [Google Scholar]
- UNHCR. Global Report 2017; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2017; Available online: http://reporting.unhcr.org/sites/default/files/gr2017/pdf/GR2017_English_Full_lowres.pdf (accessed on 23 November 2018).
- WHO. ICN Framework of Disaster Nursing Competencies; World Health Organization and International Council of Nurses: Geneva, Switzerland, 2009; Available online: www.wpro.who.int/hrh/documents/icn_framework.pdf (accessed on 23 November 2018).
- WHO. Definitions: Emergencies; World Health Organization: Geneva, Switzerland, 2008; Available online: https://www.who.int/hac/about/reliefweb-aug2008.pdf?ua=1 (accessed on 23 November 2018).
- Leppold, C.; Ozaki, A.; Shimada, Y.; Morita, T.; Tanimoto, T. Defining and acting on global health: The case of Japan and the refugee crisis. Int. J. Health Policy Manag. 2016, 5, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Broach, J.P.; McNamara, M.; Harrison, K. Ambulatory care by disaster responders in the tent camps of Port-au-Prince, Haiti, January 2010. Dis. Med. Public Health Prep. 2010, 4, 116–121. [Google Scholar] [CrossRef]
- Anwar, J.; Mpofu, E.; Matthews, L.R.; Shadoul, A.F.; Brock, K.E. Reproductive health and access to healthcare facilities: Risk factors for depression and anxiety in women with an earthquake experience. BMC Public Health 2011, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- Augusterfer, E.F.; Mollica, R.F.; Lavelle, J. A review of telemental health in international and post-disaster settings. Int. Rev. Psychiatry 2015, 27, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Messiah, A.; Lacoste, J.; Gokalsing, E.; Shultz, J.M.; de la Vega, P.R.; Castro, G.; Acuna, J.M. Mental health impact of hosting disaster refugees: Analyses from a random sample survey among Haitians living in Miami. South Med. J. 2016, 109, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Perez-Martın, J.J.; Romera Guirado, F.J.; Molina-Salas, Y.; Bernal-Gonzalez, P.J.; Navarro-Alonso, J.A. Vaccination campaign at a temporary camp for victims of the earthquake in Lorca (Spain). Hum. Vaccin Immunother. 2017, 13, 1714–1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porignon, D.; Noterman, J.P.; Hennart, P.; Tonlget, R.; Soron’Gane, E.M.; Lokombe, T.E. The role of Zairian health services in the Rwandan refugee crisis. Disasters 1995, 19, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Porignon, D.; Soron‘Gane, E.M.; Lokombe, T.E.; Isu, D.K.; Hennart, P.; van Lerberghe, W. How robust are district health systems? Coping with crisis and disasters in Rutshuru, Democratic Republic of Congo. Trop. Med. Int. Health 1998, 3, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Kunii, O.; Okumura, J.; Wakai, S. Refugee participation in health relief services during the post-emergency phase in Tanzania. Public Health 2004, 118, 50–61. [Google Scholar] [CrossRef]
- Chynoweth, S.K. The need for priority reproductive health services for displaced Iraqi women and girls. Reprod. Health Matters 2008, 16, 93–102. [Google Scholar] [CrossRef]
- Crooks, A.; Hailegiorgis, A. Disease modeling within refugee camps: A multi-agent systems approach. In Proceedings of the 2013 Winter Simulation Conference, Washington, DC, USA, 8–11 December 2013; pp. 1697–1706. [Google Scholar]
- Akl, E.A.; El-Jardali, F.; Bou Karroum, L.; El-Eid, J.; Brax, H.; Akik, C.; Osman, M.; Hassan, G.; Itani, M.; Farha, A.; et al. Effectiveness of mechanisms and models of coordination between organizations, agencies and bodies providing or financing health services in humanitarian crises: A systematic review. PLoS ONE 2015, 10, e0137159. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.T.; Dawson, A.; Meyers, J.; Krause, S.; Hickling, C. Inter-Agency Working Group (IAWG) on reproductive health in crisis. Developing institutional capacity for reproductive health in humanitarian settings: A descriptive study. PLoS ONE 2015, 10, e0137412. [Google Scholar] [CrossRef] [PubMed]
- Alpak, G.; Unal, A.; Bulbul, F.; Sagaltici, E.; Bez, Y.; Altindag, A.; Dalkilic, A.; Savas, H.A. Post-traumatic stress disorder among Syrian refugees in Turkey: A cross-sectional study. Int. J. Psychiatry Clin. Pract. 2015, 19, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Morand, M.B. Mental health and psychosocial support in humanitarian settings: Reflections on a review of UNHCR’s approach and activities. Intervention 2015, 13, 235–247. [Google Scholar] [CrossRef]
- Ghumman, U.; McCord, C.E.; Chang, J. Posttraumatic stress disorder in Syrian refugees: A review. Can. Psychol. 2016, 57, 246–253. [Google Scholar] [CrossRef]
- Alfadhli, K.; Drury, J. The role of shared social identity in mutual support among refugees of conflict: An ethnographic study of Syrian refugees in Jordan. J. Community Appl. Soc. Psychol. 2018, 28, 142–155. [Google Scholar] [CrossRef]
- Massey, E.; Smith, J.; Roberts, B. Health needs of older populations affected by humanitarian crises in low- and middle income countries: A systematic review. Confl. Health 2017, 11, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.Y.; Chiu, C.P.; Chan, G.K.W. Medical and health risks associated with communicable diseases of Rohingya refugees in Bangladesh 2017. Int. J. Infect. Dis. 2018, 68, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Teeter, D.S. Illnesses and injuries reported at Disaster Application Centers following the 1994 Northridge earthquake. Mil. Med. 1996, 161, 526–530. [Google Scholar] [CrossRef] [PubMed]
- Edwards, T.D.; Young, R.A.; Lowe, A.F. Caring for a surge of hurricane Katrina evacuees in primary care clinics. Ann. Fam. Med. 2007, 5, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Abbas, H.B.; Routray, J.K. A semi-quantitative risk assessment model of primary health care service interruption during flood: Case study of Aroma locality, Kassala state of Sudan. Int. J. Dis. Risk Reduct. 2013, 6, 118–128. [Google Scholar] [CrossRef]
- Wineman, N.V.; Braun, B.I.; Barbera, J.A.; Loeb, J.M. Assessing the integration of health center and community emergency preparedness and response planning. Dis. Med. Public Health Prep. 2007, 1, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Femino, M.; Sayah, A.; Weiner, D.L.; Yim, E.S.; Douthwright, S.; Molloy, M.S.; Irfan, F.B.; Karkoukli, M.A.; Lipton, R.; et al. Health care system hazard vulnerability analysis: An assessment of all public hospitals in Abu Dhabi. Disasters 2014, 38, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Kanter, R.K.; Abramson, D.M.; Redlener, I.; Gracy, D. The medical home and care coordination in disaster recovery: Hypothesis for interventions and research. Dis. Med. Public Health Prep. 2015, 9, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Al-Ali, N.M.; Abu Ibaid, A.H. Health-care providers’ perception of knowledge, skills and preparedness for disaster management in primary health-care centres in Jordan. East Mediterr. Health J. 2015, 21, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Abouteir, A.; El Yaagoubi, F.; Bioh-Johnson, I.; Kamel, A.; Godard, N.; Cormerais, L.; Robin, F.; Lesens, O. Water access and attendance for diarrhea in primary health care centers, Gaza strip. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Yagub, A.I.; Mtshali, K. The role of non-governmental organizations in providing curative health services in North Darfur State, Sudan. Afr. Health Sci. 2015, 15, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- van der Veen, A.; van Pietersom, T.; Lopes Cardozo, B.; Rushiti, F.; Ymerhalili, G.; Agani, F. Integrating staff well-being into the primary health care system: A case study in post-conflict Kosovo. Confl. Health 2015, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Jonsson, R.; Skaff, R.; Tylera, F. Community-based noncommunicable disease care for Syrian refugees in Lebanon. Glob. Health Sci. Pract. 2017, 5, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Lionis, C.; Petelos, E.; Mechili, E.A.; Sifaki-Pistolla, D.; Chatzea, V.E.; Angelaki, A.; Rurik, I.; Pavlic, D.R.; Dowrick, C.; Dückers, M.; et al. Assessing refugee healthcare needs in Europe and implementing educational interventions in primary care: A focus on methods. BMC Int. Health Hum. Rights 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.C.; Ventevogel, P.; Spiegel, P.; Bass, J.K.; van Ommeren, M.; Tol, W.A. Mental, neurological, and substance use problems among refugees in primary health care: Analysis of the Health Information System in 90 refugee camps. BMC Med. 2014, 12, 228. [Google Scholar] [CrossRef] [PubMed]
- Daw, M.A.; El-Bouzedi, A.; Dau, A.A. The assessment of efficiency and coordination within the Libyan health care system during the armed conflict-2011. Clin. Epidemiol. Glob. Health 2016, 4, 120–127. [Google Scholar] [CrossRef]
- Doocy, S.; Lyles, E.; Hanquart, B.; The LHAS Study Team; Woodman, M. Prevalence, care-seeking, and health service utilization for non-communicable diseases among Syrian refugees and host communities in Lebanon. Confl. Health 2016, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Hamdani, S.U.; Awan, N.R.; Bryant, R.A.; Dawson, K.S.; Khan, M.F.; Azeemi, M.M.; Akhtar, P.; Nazir, H.; Chiumento, A.; et al. Effect of a multicomponent behavioral intervention in adults impaired by psychological distress in a conflict-affected area of Pakistan: A randomized clinical trial. JAMA 2016, 316, 2609–2617. [Google Scholar] [CrossRef] [PubMed]
- Memari, P.; Tavakkoli-Moghaddam, R.; Partovi, M.; Zabihian, A. Fuzzy dynamic location-allocation problem with temporary multi-medical centers in disaster management. IFAC-Pap. 2018, 51, 1554–1560. [Google Scholar] [CrossRef]
- Gao, X.; Zhou, Y.; Haq Amir, M.I.; Rosyidah, F.A.; Lee, G.M. A hybrid genetic algorithm for multi-emergency medical service center location-allocation problem in disaster response. Int. J. Ind. Eng. Theory 2017, 24, 663–679. [Google Scholar]
- Tavakkoli-Moghaddam, R.; Memari, P.; Talebi, E. A bi-objective location-allocation problem of temporary emergency stations and ambulance routing in a disaster situation. In Proceedings of the 4th International Conference on Optimization and Applications (ICOA), Mohammedia, Morocco, 26–26 April 2018. [Google Scholar]
- Muafa, M.; Concho, A.L.; Ramirez-Marquez, J.E. Emergency resource allocation for disaster response: An evolutionary approach. In Proceedings of the 12th International Conference on Probabilistic Satefy Assessment and Management (PSAM), Honolulu, HI, USA, 22–27 June 2014. [Google Scholar] [CrossRef]
- Decker, B.T. Emergency Shelter Resource Allocation and Location Analysis. Master’s Thesis, University of Connnecticut Graduate School, Storrs, CT, USA, 7 May 2016. [Google Scholar]
- Mohamadi, A.; Yaghoubi, S. A new stochastic location-allocation emergency medical services healthcare system model during major disaster. J. Ind. Syst. Eng. 2016, 9, 85–99. [Google Scholar]
- Aghamohammadi, H.; Saadi Mesgari, M.; Molaei, D.; Aghamohammadi, H. Development a heuristic method to locate and allocate the medical centers to minimize the earthquake relief operation time. Iran. J. Public Health 2013, 42, 63–71. [Google Scholar]
- Rowls, C.G. Prepositioning of Emergency Supplies for Disaster Response. Ph.D. Thesis, The Faculty of the Graduate School of Cornell University, New York, NY, USA, August 2018. [Google Scholar]
- Khojasteh, S.B.; Macit, I. A stochastic programming model for decision-making concerning medical supply location and allocation in disaster management. Dis. Med. Public Health Prep. 2017, 11, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Farahani, R.Z.; SteadieSeifi, M.; Asgari, N. Multiple criteria facility location problems: A survey. Appl. Math. Model. 2010, 34, 1689–1709. [Google Scholar] [CrossRef]
- Balcik, B.; Beamon, B.M. Facility location in humanitarian relief. Int. J. Logist.-Res. Appl. 2008, 11, 101–121. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Z.; Zhu, X.; Wyatt, T. Covering models and optimization techniques for emergency response facility location and planning: A review. Math. Methods Oper. Res. 2011, 74, 281–310. [Google Scholar] [CrossRef]
- Trivedi, A.; Singh, A. Facility location in humanitarian relief: A review. Int. J. Emerg. Manag. 2018, 14, 213–232. [Google Scholar] [CrossRef]
- Boonme, C.; Arimura, A.; Asada, T. Facility location optimization model for emergency humanitarian logistics. Int. J. Dis. Risk Reduct. 2017, 24, 485–498. [Google Scholar] [CrossRef]
- Abounacer, R.; Rekik, M.; Renaud, J. An exact solution approach for multi-objective location-transportation problem for disaster response. Comput. Oper. Res. 2014, 41, 83–93. [Google Scholar] [CrossRef]
- Ulungu, E.L.; Teghem, J. Multi-objective combinatorial optimization problems: A survey. J. Multi Criteria Decis. Anal. 1994, 3, 83–104. [Google Scholar] [CrossRef]
- Aiello, G.; Enea, M.; Galante, G. A Multi-Objective approach to facility layout problem by genetic search algorithm and Electre method. Robot Comput. Integr. Manuf. 2006, 22, 447–455. [Google Scholar] [CrossRef]
- Ye, M.; Zhou, G. A local genetic approach to multi-objective, facility layout problems with fixed aisles. Int. J. Prod. Res. 2007, 45, 5243–5264. [Google Scholar] [CrossRef]
- Singh, S.P.; Singh, V.K. Three-level AHP-Based heuristic approach for a multi-objective facility layout problem. Int. J. Prod. Res. 2011, 49, 1105–1125. [Google Scholar] [CrossRef]
- Xu, J.; Li, Z. Multi-Objective dynamic construction site layout planning in fuzzy random environment. Autom. Constr. 2012, 27, 155–169. [Google Scholar] [CrossRef]
- Hathhorn, J.; Sisikoglu, E.; Sir, M.Y. A Multi-Objective mixed-integer programming model for a multi-floor facility layout. Int. J. Prod. Res. 2013, 51, 4223–4239. [Google Scholar] [CrossRef]
- Emami, S.; Nookabadi, A.S. Managing a new multi-objective model for the dynamic facility layout problem. Int. J. Adv. Manuf. Technol. 2013, 68, 2215–2228. [Google Scholar] [CrossRef]
- Xu, J.; Liu, Q.; Lei, X. A fuzzy Multi-Objective model and application for the discrete dynamic temporary facilities location planning problem. J. Civ. Eng. Manag. 2016, 22, 357–372. [Google Scholar] [CrossRef]
- Li, H.; Sun, R.J.; Dong, K.Y.; Dong, X.C.; Zhou, Z.B.; Leng, X. Selecting China’s strategic petroleum reserve sites by multi-objective programming model. Pet. Sci. 2017, 14, 622–635. [Google Scholar] [CrossRef] [Green Version]
- Ishizaka, A.; Nemery, P. Multi-Criteria Decision Analysis: Methods and Software, 1st ed.; John Wiley & Sons, Ltd.: West Sussex, UK, 2013. [Google Scholar]
- Jones, D.; Tamiz, M. Practical Goal Programming; Springer: New York, NY, USA, 2010; Volume 141. [Google Scholar]
- Gass, S. The setting of weights in linear goal-programming problems. Comput. Oper. Res. 1987, 14, 227–229. [Google Scholar] [CrossRef]
- Tamiz, M.; Jones, D.; Romero, C. Goal programming for decision making: An overview of the current state-of-the-art. Eur. J. Oper. Res. 1998, 111, 569–581. [Google Scholar] [CrossRef]
- Condon, E.; Golden, B.; Wasil, E. Visualizing group decisions in the analytic hierarchy process. Comput. Oper. Res. 2003, 30, 1435–1445. [Google Scholar] [CrossRef]
- Dyer, R.F.; Forman, E.H. Group decision support with the analytic hierarchy process. Decis. Support Syst. 1992, 8, 99–124. [Google Scholar] [CrossRef]
- Saaty, T.L. The Analytic Hierarchy Process; McGraw-Hill International: New York, NY, USA, 1980. [Google Scholar]
- Golden, B.L. The Analytic Hierarchy Process: Applications and Studies, Annotated ed.; Springer: New York, NY, USA, 1989. [Google Scholar]
- Memarian, H.; Balasundram, S.K.; Abbaspour, K.C.; Talib, J.B.; Teh Boon Sung, C.; Mohd Sood, A. Integration of analytic hierarchy process and weighted goal programming for land use optimization at the watershed scale. Turk. J. Eng. Environ. Sci. 2015, 38, 139–158. [Google Scholar] [CrossRef]
- Tajbakhsh, S.M.; Memarian, H.; Kheyrkhah, A. A GIS-based integrative approach for land use optimization in a semi-arid watershed. Glob. J. Environ. Sci Manag. 2018, 4, 31–46. [Google Scholar]
- Ho, W. Combining analytic hierarchy process and goal programming for logistics distribution network design. In Proceedings of the IEEE International Conference on Systems, Man and Cybernetics, Montreal, QC, Canada, 7–10 October 2007; pp. 714–719. [Google Scholar]
- Coyle, G. The Analytic Hierarchy Process; Pearson Education Open Access Material: Upper Saddle River, NJ, USA, 2004. [Google Scholar]
- Radcliffe, L.L.; Schniederjans, M.J. Trust evaluation: An AHP and multi-objective programming approach. Manag. Decis. 2003, 41, 587–595. [Google Scholar] [CrossRef]
- Kwak, N.K.; Lee, C.W. A multicriteria decision-making approach to university resource allocations and information infrastructure planning. Eur. J. Oper. Res. 1998, 110, 234–242. [Google Scholar] [CrossRef]
- Schniederjans, M.J.; Garvin, T. Using the analytic hierarchy process and multi-objective programming for the selection of cost drivers in activity-based costing. Eur. J. Oper. Res. 1997, 100, 72–80. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Meaning |
|---|---|
| I | Set of demand nodes; i ϵ I |
| J | Set of candidate locations; j ϵ J |
| N | Set of targeted goals; n ϵ N |
| Demand at node i | |
| Fixed cost of locating a PHCC at site j | |
| Running cost of each person at site j (constant number) | |
| Capacity of each candidate location j | |
| Amount of cash for work in each candidate location j | |
| TC | Transportation cost for a distance of 1 km (constant number) |
| Distance between node i and location j (acquired via constructing a GIS roads network dataset) | |
| (covering matrix) | |
| Penalty of not achieving the objective related to deviation | |
| Penalty of not achieving the objective related to deviation | |
| Right hand sides of targeted goal n according to goal programming | |
| Positive deviational variable—amount of an overachieved targeted goal n | |
| Negative deviational variable—amount of an underachieved targeted goal n |
| Intensity of Importance | Definition | Explanation |
|---|---|---|
| 1 | Equal importance | Two elements are equally important |
| 3 | Moderate importance | Experience and judgment slightly favor one element over another |
| 5 | Strong importance | Experience and judgment strongly favor one element over another |
| 7 | Very strong importance | One element is favored very strongly over another |
| 9 | Extreme importance | One element is absolutely more important over another |
| 2, 4 ,6, 8 | Intermediate values | When compromise is needed |
| Objectives | Weights |
|---|---|
| P1 | 44.7% |
| P2 | 14.4% |
| P3 | 4.7% |
| P4 | 4.7% |
| P5 | 4.7% |
| P6 | 4.7% |
| P7 | 4.7% |
| P8 | 8.7% |
| P9 | 8.7% |
| N | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|
| 0.58 | 0.9 | 1.12 | 1.24 | 1.32 | 1.41 | 1.45 | 1.49 | 1.51 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miç, P.; Koyuncu, M.; Hallak, J. Primary Health Care Center (PHCC) Location-Allocation with Multi-Objective Modelling: A Case Study in Idleb, Syria. Int. J. Environ. Res. Public Health 2019, 16, 811. https://doi.org/10.3390/ijerph16050811
Miç P, Koyuncu M, Hallak J. Primary Health Care Center (PHCC) Location-Allocation with Multi-Objective Modelling: A Case Study in Idleb, Syria. International Journal of Environmental Research and Public Health. 2019; 16(5):811. https://doi.org/10.3390/ijerph16050811
Chicago/Turabian StyleMiç, Pınar, Melik Koyuncu, and Jamil Hallak. 2019. "Primary Health Care Center (PHCC) Location-Allocation with Multi-Objective Modelling: A Case Study in Idleb, Syria" International Journal of Environmental Research and Public Health 16, no. 5: 811. https://doi.org/10.3390/ijerph16050811