
Summary
We address, from a pharmacokinetic viewpoint, the important question of why some patients with clinical idiopathic Parkinson's disease experience a fall off in benefit from levodopa maintenance therapy.
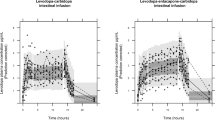
Thirteen such patients, of mean age 78 y, without overt fluctuations in motor control in temporal relation to dosing with a levodopa/decarboxylase inhibitor combination, were studied. Levodopa (currently 400 to 800 mg daily) had been started at between 61 and 81 y of age, the mean duration of therapy being 54 months. Plasma concentrations of levodopa and its peripheral metabolite, 3-0-methyldopa, were measured before a morning dose of levodopa (100 mg)/carbidopa (25 mg) and at hourly intervals for 6 h after.
There was a significant negative regression between duration of levodopa therapy (but not age or severity of disease) and the area under the plasma concentration/time curve (AUC) for levodopa attributed to the test dose. A significant negative regression was also seen of duration of therapy on the dose absorbed per unit distribution volume, but not on the elimination rate constant, indicating a decrease in bioavailability and/or an increase in distribution volume with duration. There was a tendency for the plasma 3-0-methyldopa concentration, standardised for daily dose, [30MD], to increase with duration of therapy. Although, the regression of duration on [30MD] did not reach statistical significance, that on the ratio, [30MD]/AUC, did so at the 0.01 level.
The amount by, and time for which, the plasma levodopa concentration exceeds any critical threshold for the competitive active uptake process into the brain may thus decrease with duration of therapy. This may explain in part the limited reversal of the neurological deficit, which is more typical of later onset Parkinsonism, and, possibly, the decrement in biological half time with duration of therapy, typical of early onset disease. 3-0-Methyldopa is known to compete for active uptake with levodopa; the ratio, [30MD]/AUC, may be a measure of this competition. Intrinsic activity of neuronal uptake mechanisms, capacity of the basal ganglia for storage of dopamine, and post synaptic neuronal activity may, of course, also be determinants of clinical outcome.
Similar content being viewed by others


References
Direnfeld L, Spero L, Marotha J, Seeman P (1978) The L-dopa ‘on-off’ effect in Parkinson's disease: treatment by transient drug withdrawal and dopamine receptor resensitization. Ann Neurol 4: 573–575
Evans MA, Triggs EJ, Broe GA, Saines N (1980) Systemic availability of orally administered L-dopa in the elderly Parkinsonian patient. Eur J Clin Pharmacol 17: 215–221
Evans MA, Broe GA, Triggs EJ, Cheung M, Creasey H, Pacell PD (1981) Gastric emptying rate and systemic availability of levodopa in the elderly Parkinsonian patient. Neurology 31: 1288–1294
Hughes JR, Bowes SG, Leeman AL, O'Neill CJA, Deshmukh AA, Nicholson PW, Dobbs SM, Dobbs RJ (1990) Parkinsonian abnormality of foot strike: a phenomenon of ageing and/or one responsive to levodopa therapy? Br J Clin Pharmacol 29: 179–186
Kempster PA, Frankel JP, Bovingdon M, Webster R, Lees AJ, Stern GM (1989) Levodopa peripheral pharmacokinetics and duration of motor response in Parkinson's disease. J Neurol Neurosurg Psychiat 52: 718–723
Kuruma I, Bartholini G, Tissot R, Pletscher A (1971) The metabolism of L-3-0-methyldopa, a precursor of dopa in man. Clin Pharmacol Ther 12: 678–682
Lee T, Seeman P, Rajput A, Farley IJ, Hornykiewicz O (1978) Receptor basis of dopaminergic supersensitivity in Parkinson's disease. Nature 273: 59–61
Lewitt PA (1989) The pharmacology of levodopa in treatment of Parkinson's disease: An update. In: Calne DB (ed) Drugs for the treatment of Parkinson's disease. Springer, New York, pp 325–384
Meunter MD, Sharpless NS, Tyce GM (1972) Plasma 3-0-methyldopa in L-dopa therapy of Parkinson's disease. Mayo Clinic Proc 47: 389–395
Quinn NP, Hussain FA (1986) Parkinson's disease. Br med J 293: 379–382
Rivera-Calimlim L, Tandon D, Anderson F, Joynt R (1977) The clinical picture and plasma levodopa metabolite profile of Parkinsonian non-responders. Treatment with levodopa and decarboxylase inhibitor. Arch Neurol 34: 228–232
Robertson DRC, Higginson I, Macklin BS, Waller DG, Renwick AG (1990b) The influence of protein on the absorption of levodopa. Br J Clin Pharmacol 29: 608P
Robertson DRC, Renwick AG, Wood ND, Cross N, Macklin BS, Fleming JS, Waller DG, George CF (1990a) The influence of levodopa on gastric emptying in man. Br J Clin Pharmacol 29: 47–53
Robertson DRC, Wood ND, Everest H, Monks K, Waller DG, Renwick AG, George CF (1989) The effect of age on the pharmacokinetics of levodopa administered alone and in the presence of carbidopa. Br J Clin Pharmacol 28: 61–69
Wade DN, Mearrick PT, Morris JL (1973) Active transport of L-dopa in the intestine. Nature 242: 463–465
Wade LA, Katzman R (1975) Synthetic amino acids and the nature of L-dopa transport at the blood-brain barrier. J Neurochem 25: 837–842
Weiner WJ, Koller WC, Perlik S, Nausieda PA, Klawans HL (1980) Drug holiday and management of Parkinson's disease. Neurology 30: 1257–1261
Yahr MD (1981) Pharmacological treatment of Parkinson's disease in early and late phases. In: Rose FC, Capildeo R (eds) Research progress in Parkinson's disease. Pitman Medical, London (Progress in Neurology series) pp 233–240
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bowes, S.G., O'Neill, C.J.A., Nicholson, P.W. et al. Effect of duration of levodopa/decarboxylase inhibitor therapy on the pharmacokinetic handling of levodopa in elderly patients with idiopathic Parkinson's disease. Eur J Clin Pharmacol 41, 459–462 (1991). https://doi.org/10.1007/BF00626369
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00626369