
Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China

 ,
,
Abstract
:1. Introduction
2. Methods
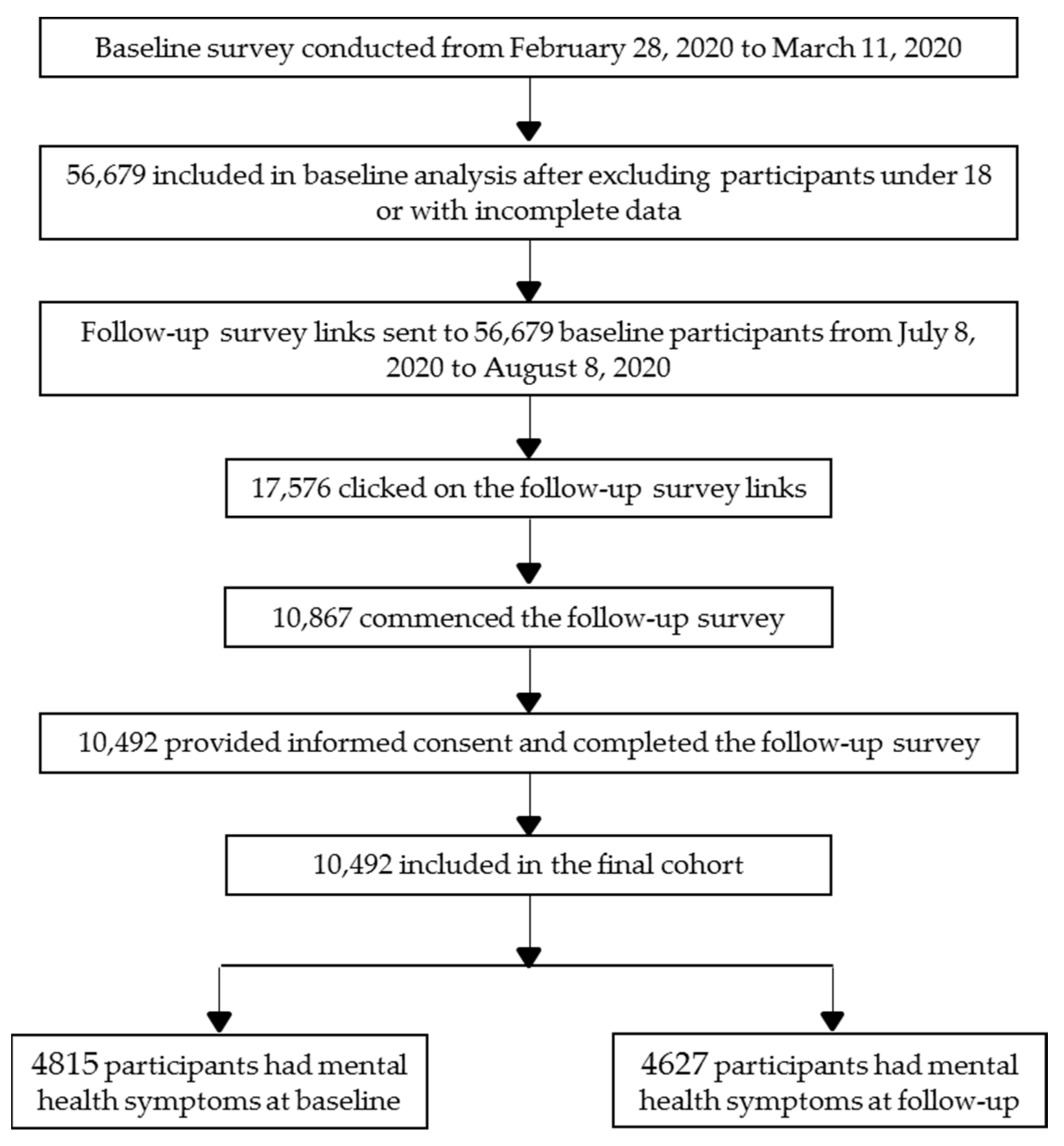
2.1. Study Design
2.2. Participants
2.3. Measures and Variables
2.4. Statistical Analyses
3. Results
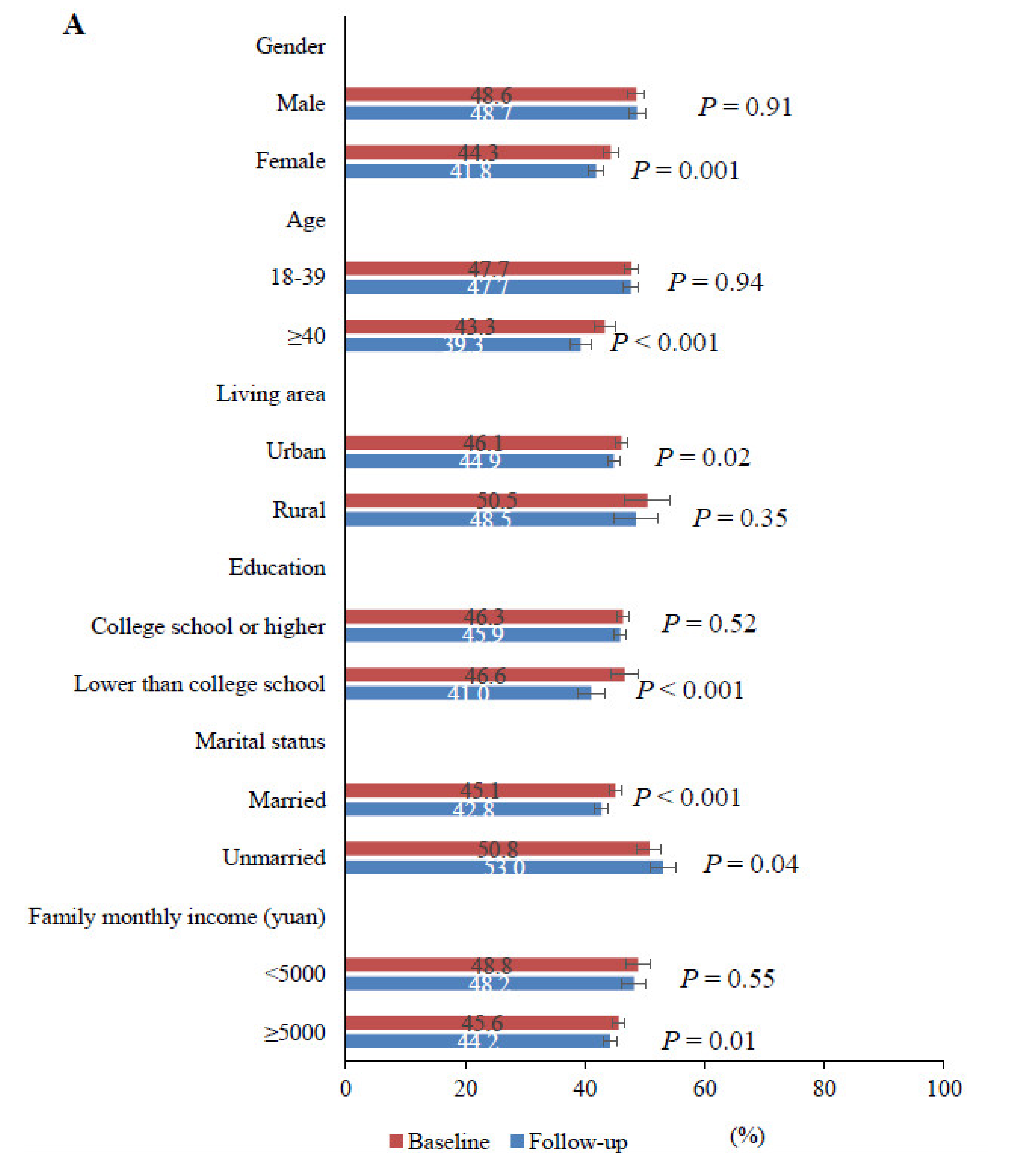
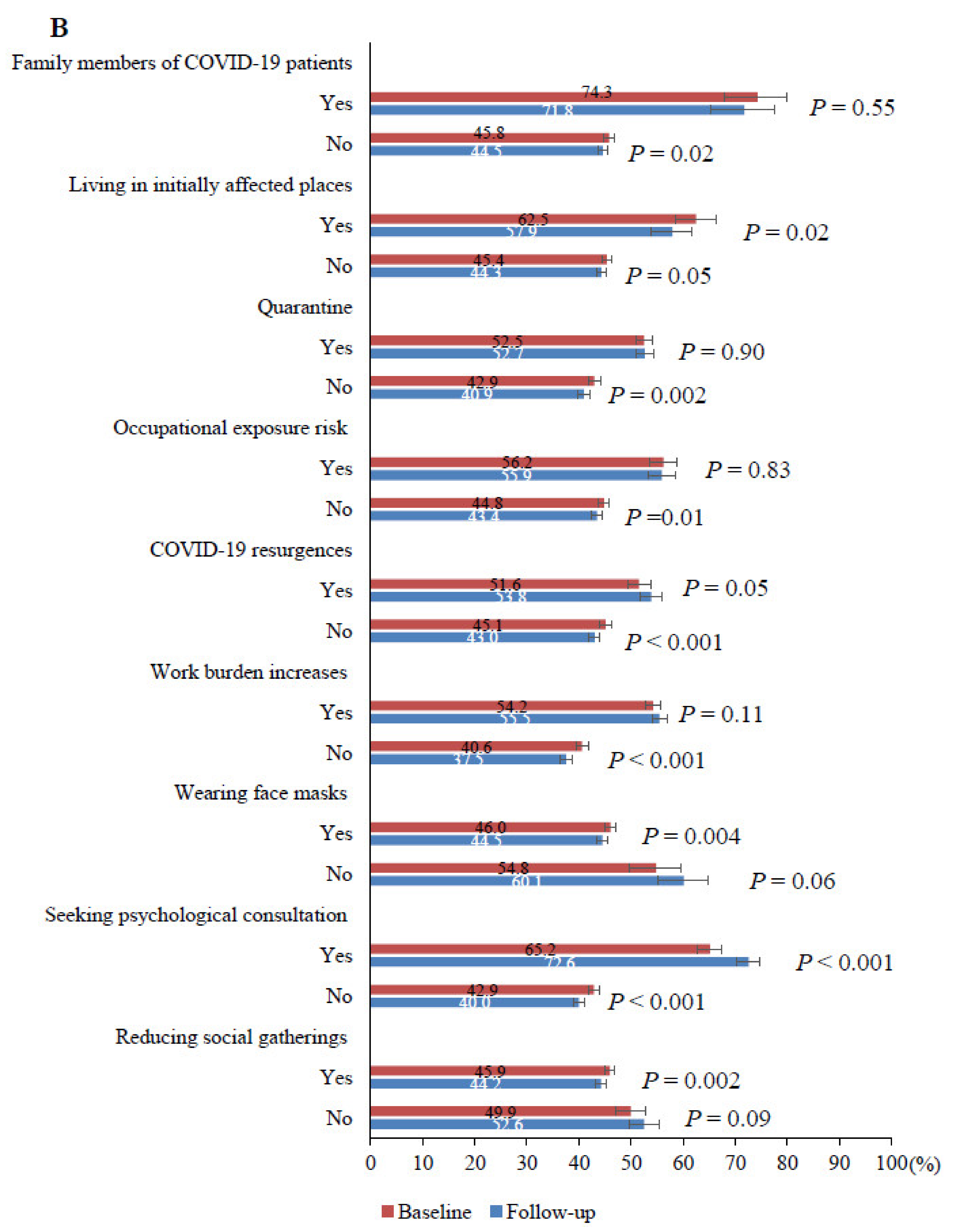
3.1. Demographic and Epidemic-Related Characteristics of Participants
3.2. Change in Mental Health Symptoms from Baseline to Follow-Up Survey
3.3. Proportions of New Onset and Persistent Mental Health Symptoms from Baseline to Follow-Up Survey
3.4. Factors Associated with Long-Term Positive of Mental Health Symptoms during the Course of COVID-19
3.5. Factors Associated with Scores of Depression, Anxiety and Insomnia Symptoms during the Course of COVID-19
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 7 August 2021).
- Meo, S.A.; Alhowikan, A.M.; Al-Khlaiwi, T.; Meo, I.M.; Halepoto, D.M.; Iqbal, M.; Usmani, A.M.; Hajjar, W.; Ahmed, N. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 2012–2019. [Google Scholar] [CrossRef] [PubMed]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.J.; Bao, Y.; Huang, X.; Shi, J.; Lu, L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc. Health 2020, 4, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lu, Z.A.; Que, J.Y.; Huang, X.L.; Liu, L.; Ran, M.S.; Gong, Y.M.; Yuan, K.; Yan, W.; Sun, Y.K.; et al. Prevalence of and Risk Factors Associated With Mental Health Symptoms Among the General Population in China During the Coronavirus Disease 2019 Pandemic. JAMA Netw. Open 2020, 3, e2014053. [Google Scholar] [CrossRef]
- Gupta, S.; Goren, A.; Dong, P.; Liu, D. Prevalence, awareness, and burden of major depressive disorder in urban China. Expert Rev. Pharm. Outcomes Res. 2016, 16, 393–407. [Google Scholar] [CrossRef]
- Zhou, X.; Bi, B.; Zheng, L.; Li, Z.; Yang, H.; Song, H.; Sun, Y. The prevalence and risk factors for depression symptoms in a rural Chinese sample population. PLoS ONE 2014, 9, e99692. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Singh, S.S.; Calhoun, S.; Zhang, H.; Zhao, X.; Yang, F. Generalized anxiety disorder in urban China: Prevalence, awareness, and disease burden. J. Affect. Disord. 2018, 234, 89–96. [Google Scholar] [CrossRef]
- Cao, X.L.; Wang, S.B.; Zhong, B.L.; Zhang, L.; Ungvari, G.S.; Ng, C.H.; Li, L.; Chiu, H.F.; Lok, G.K.; Lu, J.P.; et al. The prevalence of insomnia in the general population in China: A meta-analysis. PLoS ONE 2017, 12, e0170772. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Cheng, C.; Zeng, Y.; Li, Y.; Zhu, M.; Yang, W.; Xu, H.; Li, X.; Leng, J.; Monroe-Wise, A.; et al. Mental Health Disorders and Associated Risk Factors in Quarantined Adults During the COVID-19 Outbreak in China: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e20328. [Google Scholar] [CrossRef]
- Venkatesh, A.; Edirappuli, S. Social distancing in COVID-19: What are the mental health implications? BMJ 2020, 369, m1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of Covid-19 Lockdown on Mental Health and Sleep Disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, L.; Que, J.; Lu, Q.; Liu, L.; Lu, Z.; Xu, Y.; Liu, J.; Sun, Y.; Meng, S.; et al. The impact of quarantine on mental health status among general population in China during the COVID-19 pandemic. Mol. Psychiatry 2021, 1–10. [Google Scholar] [CrossRef]
- Lee, A.M.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.M.; Wong, P.C.; Tsang, K.W.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef] [PubMed]
- Kwek, S.K.; Chew, W.M.; Ong, K.C.; Ng, A.W.; Lee, L.S.; Kaw, G.; Leow, M.K. Quality of life and psychological status in survivors of severe acute respiratory syndrome at 3 months postdischarge. J. Psychosom. Res. 2006, 60, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Psychological distress and adaptation to the COVID-19 crisis in the United States. J. Psychiatr. Res. 2021, 136, 603–609. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, e87. [Google Scholar] [CrossRef] [PubMed]
- McGinty, E.E.; Presskreischer, R.; Anderson, K.E.; Han, H.; Barry, C.L. Psychological Distress and COVID-19-Related Stressors Reported in a Longitudinal Cohort of US Adults in April and July 2020. JAMA 2020, 324, 2555–2557. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.L.; Ao, M.Y.; Zhou, X.; Zhu, W.F.; Nie, H.Y.; Fang, J.H.; Sun, X.; Zheng, B.; Chen, X.F. China’s practice to prevent and control COVID-19 in the context of large population movement. Infect. Dis. Poverty 2020, 9, 115. [Google Scholar] [CrossRef]
- Shen, J.; Duan, H.; Zhang, B.; Wang, J.; Ji, J.S.; Wang, J.; Pan, L.; Wang, X.; Zhao, K.; Ying, B.; et al. Prevention and control of COVID-19 in public transportation: Experience from China. Environ. Pollut. 2020, 266 (Pt 2), 115291. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, S.; Xu, L. Asymptomatic carriers of COVID-19 as a concern for disease prevention and control: More testing, more follow-up. Biosci. Trends 2020, 14, 206–208. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, C.; Bélanger, L.; Ivers, H.; Morin, C.M. Validation of the Insomnia Severity Index in primary care. J. Am. Board Fam. Med. 2013, 26, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef]
- The, L. Social media, screen time, and young people’s mental health. Lancet 2019, 393, 611. [Google Scholar] [CrossRef] [Green Version]
- Ganson, K.T.; Tsai, A.C.; Weiser, S.D.; Benabou, S.E.; Nagata, J.M. Job Insecurity and Symptoms of Anxiety and Depression Among U.S. Young Adults During COVID-19. J. Adolesc. Health 2021, 68, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Saha, S. Improving literacy as a means to reducing health disparities. J. Gen. Intern. Med. 2006, 21, 893–895. [Google Scholar] [CrossRef] [Green Version]
- Tang, B.; Xia, F.; Tang, S.; Bragazzi, N.L.; Li, Q.; Sun, X.; Liang, J.; Xiao, Y.; Wu, J. The effectiveness of quarantine and isolation determine the trend of the COVID-19 epidemics in the final phase of the current outbreak in China. Int. J. Infect. Dis. 2020, 95, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol. Infect. 2008, 136, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; Gan, Y.; Wang, C.; Bachmann, M.; Wei, S.; Gong, J.; Huang, Y.; Wang, T.; Li, L.; Lu, K.; et al. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat. Commun. 2020, 11, 5917. [Google Scholar] [CrossRef] [PubMed]
- Spittlehouse, J.K.; Joyce, P.R.; Vierck, E.; Schluter, P.J.; Pearson, J.F. Ongoing adverse mental health impact of the earthquake sequence in Christchurch, New Zealand. Aust. N. Z. J. Psychiatry 2014, 48, 756–763. [Google Scholar] [CrossRef]
- Tang, W.; Zhao, J.; Lu, Y.; Yan, T.; Wang, L.; Zhang, J.; Xu, J. Mental health problems among children and adolescents experiencing two major earthquakes in remote mountainous regions: A longitudinal study. Compr. Psychiatry 2017, 72, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Qian, W.; Li, Z.; Liu, Z.; Zhou, Y.; Wang, R.; Qi, L.; Yang, J.; Song, X.; Zeng, L.; et al. Public mental health under the long-term influence of COVID-19 in China: Geographical and temporal distribution. J. Affect. Disord. 2020, 277, 893–900. [Google Scholar] [CrossRef]
- Kim, A.W.; Nyengerai, T.; Mendenhall, E. Evaluating the mental health impacts of the COVID-19 pandemic: Perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol. Med. 2020, 34, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Iob, E.; Frank, P.; Steptoe, A.; Fancourt, D. Levels of Severity of Depressive Symptoms Among At-Risk Groups in the UK During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2026064. [Google Scholar] [CrossRef]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Que, J.; Shi, L.; Deng, J.; Liu, J.; Zhang, L.; Wu, S.; Gong, Y.; Huang, W.; Yuan, K.; Yan, W.; et al. Psychological impact of the COVID-19 pandemic on healthcare workers: A cross-sectional study in China. Gen. Psychiatr. 2020, 33, e100259. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Shaw, W.S.; Main, C.J.; Findley, P.A.; Collie, A.; Kristman, V.L.; Gross, D.P. Opening the Workplace After COVID-19: What Lessons Can be Learned from Return-to-Work Research? J. Occup. Rehabil. 2020, 30, 299–302. [Google Scholar] [CrossRef]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Wu, K.K.; Chan, S.K.; Ma, T.M. Posttraumatic stress after SARS. Emerg. Infect. Dis. 2005, 11, 1297–1300. [Google Scholar] [CrossRef] [Green Version]
- Tanoue, Y.; Nomura, S.; Yoneoka, D.; Kawashima, T.; Eguchi, A.; Shi, S.; Harada, N.; Miyata, H. Mental health of family, friends, and co-workers of COVID-19 patients in Japan. Psychiatry Res. 2020, 291, 113067. [Google Scholar] [CrossRef]
- Singer, J.; Spiegel, J.A.; Papa, A. Preloss grief in family members of COVID-19 patients: Recommendations for clinicians and researchers. Psychol. Trauma 2020, 12, S90–S93. [Google Scholar] [CrossRef]
- Endomba, F.T.; Wafeu, G.S.; Efon-Ekangouo, A.; Djune-Yemeli, L.; Donfo-Azafack, C.; Nana-Djeunga, H.C.; Kamgno, J. Support for families of isolated or deceased COVID-19 patients in sub-Saharan Africa. Health Psychol. Open 2020, 7, 2055102920975293. [Google Scholar] [CrossRef]
- Lam, S.C.; Arora, T.; Grey, I.; Suen, L.K.P.; Huang, E.Y.; Li, D.; Lam, K.B.H. Perceived Risk and Protection From Infection and Depressive Symptoms Among Healthcare Workers in Mainland China and Hong Kong During COVID-19. Front. Psychiatry 2020, 11, 686. [Google Scholar] [CrossRef] [PubMed]
- Scheid, J.L.; Lupien, S.P.; Ford, G.S.; West, S.L. Commentary: Physiological and Psychological Impact of Face Mask Usage during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6655. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Barile, J.P.; Guerin, R.J.; Vanden Esschert, K.L.; Jeffers, A.; Tian, L.H.; Garcia-Williams, A.; Gurbaxani, B.; Thompson, W.W.; Prue, C.E. Factors Associated with Cloth Face Covering Use Among Adults During the COVID-19 Pandemic—United States, April and May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 933–937. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.Z.; Wong, J.Y.H.; Wu, Y.; Choi, E.P.H.; Wang, M.P.; Lam, T.H. Social Distancing Compliance under COVID-19 Pandemic and Mental Health Impacts: A Population-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 6692. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factors | Total Number of Participants at Baseline (%) | Number of Baseline Participants Who Responded to Follow-Up Survey (%) | Number of Baseline Participants Who Did Not Respond to Follow-Up Survey (%) | p-Value a | Weighted Number of Participants (%) b |
|---|---|---|---|---|---|
| Overall | 56,679 (100.0) | 10,492 (100.0) | 46,187 (100.0) | - | 10,492 (100.0) |
| Mean (SD) for age, years | 35.97 (8.22) | 36.87 (8.21) | 35.76 (8.21) | <0.001 c | - |
| Age, years | |||||
| 18–39 | 39,468 (69.6) | 6815 (65.0) | 32,653 (70.7) | <0.001 | 7306 (69.6) |
| ≥40 | 17,211 (30.4) | 3677 (35.0) | 13,534 (29.3) | 3186 (30.4) | |
| Gender | |||||
| Male | 27,149 (47.9) | 4465 (42.6) | 22,684 (49.1) | <0.001 | 5026 (47.9) |
| Female | 29,530 (52.1) | 6027 (57.4) | 23,503 (50.9) | 5466 (52.1) | |
| Living area | |||||
| Urban | 52,839 (93.2) | 9769 (93.1) | 43,070 (93.3) | 0.60 | 9781 (93.2) |
| Rural | 3840 (6.8) | 723 (6.9) | 3117 (6.7) | 711 (6.8) | |
| Education | |||||
| Lower than college school | 9540 (16.8) | 2101 (20.0) | 7439 (16.1) | <0.001 | 1766 (16.8) |
| College school or higher | 47,139 (83.2) | 8391 (80.0) | 38,748 (83.9) | 8726 (83.2) | |
| Marital status | |||||
| Married | 43,763 (77.2) | 8467 (80.7) | 35,296 (76.4) | <0.001 | 8101 (77.2) |
| Unmarried | 12,916 (22.8) | 2025 (19.3) | 10,891 (23.6) | 2391 (22.8) | |
| Monthly income, yuan | |||||
| 0–4999 | 13,016 (23.0) | 2444 (23.3) | 10,572 (22.9) | 0.37 | 2402 (22.9) |
| ≥5000 | 43,663 (77.0) | 8048 (76.7) | 35,615 (77.1) | 8090 (77.1) | |
| Geographical region | |||||
| Eastern China | 23,172 (40.9) | 4283 (40.8) | 18,889 (40.9) | 0.01 | 4289 (40.9) |
| Northern China | 10,227 (18.0) | 1849 (17.6) | 8378 (18.1) | 1893 (18.0) | |
| Northeastern China | 3921 (6.9) | 781 (7.4) | 3140 (6.8) | 726 (6.9) | |
| Northwestern China | 1348 (2.4) | 219 (2.1) | 1129 (2.4) | 250 (2.4) | |
| Central China | 4803 (8.5) | 873 (8.3) | 3930 (8.5) | 889 (8.5) | |
| Southern China | 10,028 (17.7) | 1935 (18.4) | 8093 (17.5) | 1856 (17.7) | |
| South west China | 3156 (5.6) | 547 (5.2) | 2609 (5.6) | 584 (5.6) | |
| Missing values | 24 (0.0) | 5 (0.0) | 19 (0.0) | 4 (0.0) | |
| History of chronic diseases | |||||
| Yes | 3274 (5.8) | 664 (6.3) | 2610 (5.7) | 0.007 | 606 (5.8) |
| Unknown/No | 53,405 (94.2) | 9828 (93.7) | 43,577 (94.3) | 9886 (94.2) | |
| History of psychiatric disorders | |||||
| Yes | 161 (0.3) | 31 (0.3) | 130 (0.3) | 0.81 | 32 (0.3) |
| Unknown/No | 56,518 (99.7) | 10,461 (99.7) | 46,057 (99.7) | 10,460 (99.7) | |
| Family history of psychiatric disorders | |||||
| Yes | 396 (0.7) | 64 (0.6) | 332 (0.7) | 0.23 | 64 (0.6) |
| Unknown/No | 56,283 (99.3) | 10,428 (99.4) | 45,855 (99.3) | 10,428 (99.4) |
| Mental Health Symptoms | Number of Participants with Mental Health Symptoms (%, 95%CI) | Median Scores (IQR) | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline (N = 10,492) | Follow-Up (N = 10,492) | p-Value b | Baseline | Follow-Up | p-Value c | |||
| Unweighted | Weighted a | Unweighted | Weighted a | |||||
| Depression | 3071 (29.3, 28.4–30.2) | 3151 (30.0, 29.2–30.9) | 3421 (32.6, 31.7–33.5) | 3528 (33.6, 32.7–34.5) | <0.001 | 0.0 (0.0–6.0) | 0.0 (0.0–8.0) | <0.001 |
| Anxiety | 3654 (34.8, 33.9–35.7) | 3693 (35.2, 34.3–36.1) | 3320 (31.6, 30.8–32.5) | 3415 (32.5, 31.7–33.5) | <0.001 | 1.0 (0.0–7.0) | 0.0 (0.0–7.0) | <0.001 |
| Insomnia | 3066 (29.2, 28.4–30.1) | 3127 (29.8, 28.9–30.7) | 3610 (34.4, 33.5–35.3) | 3701 (35.3, 34.4–36.2) | <0.001 | 4.0 (1.0–8.0) | 4.0 (1.0–9.0) | <0.001 |
| Any mental health symptoms | 4815 (45.9, 44.9–46.9) | 4865 (46.4, 45.4–47.3) | 4627 (44.1, 43.1–45.1) | 4733 (45.1, 44.2–46.1) | 0.01 | - | - | - |
| Mental Health Symptoms | Proportion of New Onset Symptoms among Baseline Negative Participants | Proportion of Persistent Symptoms among Baseline Positive Participants | ||
|---|---|---|---|---|
| Unweighted n/N (%) | Weighted n/N (%) a | Unweighted n/N (%) | Weighted n/N (%) a | |
| Depression | 1445/7421 (19.5) | 1475/7341(20.1) | 1976/3071 (64.3) | 2052/3151 (65.1) |
| Anxiety | 1220/6838 (17.8) | 1256/6799 (18.5) | 2100/3654 (57.5) | 2159/3693 (58.5) |
| Insomnia | 1528/7426 (20.6) | 1562/7365 (21.2) | 2082/3066 (67.9) | 2139/3127 (68.4) |
| Any mental health symptoms | 1346/5677 (23.7) | 1374/5627 (24.4) | 3281/4815 (68.1) | 3359/4865 (69.0) |
| Factors | Depression | Anxiety | Insomnia | Any Mental Health Symptoms | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Gender: male (vs. female) | 1.19 (1.11–1.28) | <0.001 | 1.04 (0.97–1.12) | 0.30 | 1.18 (1.10–1.27) | <0.001 | 1.08 (1.01–1.16) | 0.03 |
| Age(years) | 0.99 (0.98–0.99) | <0.001 | 0.99 (0.99–1.00) | <0.001 | 1.00 (1.00–1.01) | 0.62 | 1.00 (0.99–1.00) | 0.08 |
| Marital status: married (vs. unmarried) | 0.85 (0.77–0.94) | 0.001 | 0.95 (0.86–1.04) | 0.25 | 0.78 (0.71–0.86) | <0.001 | 0.83 (0.75–0.91) | <0.001 |
| Family members of COVID-19 patients: yes (vs. no) | 1.79 (1.38–2.33) | <0.001 | 1.75 (1.37–2.22) | <0.001 | 1.86 (1.43–2.42) | <0.001 | 2.10 (1.61–2.74) | <0.001 |
| Experiences of quarantine: yes (vs. no) | 1.35 (1.25–1.46) | <0.001 | 1.34 (1.24–1.44) | <0.001 | 1.29 (1.20–1.40) | <0.001 | 1.31 (1.22–1.41) | <0.001 |
| Living in province most severely affected by initial peak: yes (vs. no) | 1.28 (1.10–1.49) | 0.002 | 1.32 (1.14–1.53) | <0.001 | 1.19 (1.02–1.39) | 0.03 | 1.21 (1.04–1.41) | 0.01 |
| Self-perceived occupational exposure risk to COVID-19: yes (vs. no) | 1.33 (1.20–1.48) | <0.001 | 1.39 (1.26–1.54) | <0.001 | 1.18 (1.06–1.31) | 0.002 | 1.26 (1.14–1.40) | <0.001 |
| Living in places with COVID-19 resurgences: yes (vs. no) | 1.36 (1.24–1.49) | <0.001 | 1.30 (1.18–1.42) | <0.001 | 1.37 (1.25–1.50) | <0.001 | 1.38 (1.26–1.50) | <0.001 |
| Increases in work burden after resuming work: yes (vs. no) | 1.79 (1.66–1.92) | <0.001 | 1.76 (1.64–1.90) | <0.001 | 1.78 (1.66–1.92) | <0.001 | 1.77 (1.65–1.90) | <0.001 |
| Wearing face masks voluntarily when going out: yes (vs. no) | 0.70 (0.58–0.85) | <0.001 | 0.71 (0.59–0.87) | <0.001 | 0.75 (0.62–0.90) | 0.003 | 0.74 (0.61–0.90) | 0.003 |
| Reducing social gatherings voluntarily: yes (vs. no) | 0.84 (0.74–0.95) | 0.004 | 0.92 (0.82–1.03) | 0.16 | 0.83 (0.74–0.94) | 0.003 | 0.93 (0.83–1.04) | 0.22 |
| Seeking psychological consultation since COVID-19: yes (vs. no) | 2.81 (2.55–3.10) | <0.001 | 2.78 (2.52–3.06) | <0.001 | 2.36 (2.14–2.60) | <0.001 | 2.57 (2.33–2.85) | <0.001 |
| Factors | Depression | Anxiety | Insomnia | |||
|---|---|---|---|---|---|---|
| b (SE) | p-Value | b (SE) | p-Value | b (SE) | p-Value | |
| Gender: male (vs. female) | 0.37 (0.08) | <0.001 | 0.06 (0.07) | 0.39 | 0.34 (0.09) | <0.001 |
| Age (years) | −0.02 (0.01) | <0.001 | −0.01 (0.00) | 0.007 | 0.01 (0.01) | 0.15 |
| Marital status: married (vs unmarried) | −0.38 (0.11) | <0.001 | −0.02 (0.09) | 0.82 | −0.70 (0.12) | <0.001 |
| Family members of COVID-19 patients: yes (vs. no) | 1.48 (0.30) | <0.001 | 1.44 (0.25) | <0.001 | 1.99 (0.31) | <0.001 |
| Experiences of quarantine: yes (vs. no) | 0.74 (0.08) | <0.001 | 0.64 (0.07) | <0.001 | 0.58 (0.09) | <0.001 |
| Living in province most severely affected by initial peak: yes (vs. no) | 0.81 (0.18) | <0.001 | 1.04 (0.16) | <0.001 | 0.71 (0.20) | <0.001 |
| Self-perceived occupational exposure risk to COVID-19: yes (vs. no) | 0.87 (0.12) | <0.001 | 0.70 (0.10) | <0.001 | 0.38 (0.13) | 0.003 |
| Living in places with COVID-19 resurgences: yes (vs. no) | 0.69 (0.10) | <0.001 | 0.45 (0.09) | <0.001 | 0.83 (0.11) | <0.001 |
| Increases in work burden after resuming work: yes (vs. no) | 1.07 (0.08) | <0.001 | 1.02 (0.07) | <0.001 | 1.27 (0.09) | <0.001 |
| Wearing face masks voluntarily when going out: yes (vs. no) | −0.93 (0.23) | <0.001 | −0.56 (0.20) | 0.004 | −0.72 (0.24) | 0.003 |
| Reducing social gatherings voluntarily: yes (vs. no) | −0.51 (0.14) | <0.001 | −0.15 (0.12) | 0.21 | −0.22 (0.15) | 0.14 |
| Seeking psychological consultation since COVID-19: yes (vs. no) | 2.72 (0.12) | <0.001 | 2.03 (0.11) | <0.001 | 1.82 (0.13) | <0.001 |
| Educational level × time: college school or higher (vs. lower than college school) | 0.02 (0.01) | 0.03 | 0.03 (0.01) | 0.003 | 0.05 (0.01) | 0.001 |
| Living in places with COVID-19 resurgences × time: yes (vs. no) | 0.03 (0.01) | 0.003 | 0.04 (0.01) | 0.002 | 0.03 (0.02) | 0.10 |
| Increases in work burden after resuming work × time: yes (vs. no) | 0.04 (0.01) | <0.001 | 0.02 (0.01) | 0.04 | 0.09 (0.01) | <0.001 |
| Wearing face masks voluntarily when going out × time: yes (vs. no) | −0.07 (0.03) | 0.005 | −0.07 (0.03) | 0.02 | −0.05 (0.04) | 0.17 |
| Reducing social gatherings voluntarily × time: yes (vs. no) | −0.02 (0.01) | 0.15 | −0.05 (0.02) | 0.003 | −0.08 (0.02) | <0.001 |
| Seeking psychological consultation since COVID-19 × time: yes (vs. no) | 0.21 (0.02) | <0.001 | 0.19 (0.02) | <0.001 | 0.21 (0.02) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Lu, Q.-D.; Liu, L.; Zheng, Y.-B.; Liu, W.-J.; Ran, M.-S.; Yuan, K.; et al. Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China. Int. J. Environ. Res. Public Health 2021, 18, 8790. https://doi.org/10.3390/ijerph18168790
Shi L, Lu Z-A, Que J-Y, Huang X-L, Lu Q-D, Liu L, Zheng Y-B, Liu W-J, Ran M-S, Yuan K, et al. Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China. International Journal of Environmental Research and Public Health. 2021; 18(16):8790. https://doi.org/10.3390/ijerph18168790
Chicago/Turabian StyleShi, Le, Zheng-An Lu, Jian-Yu Que, Xiao-Lin Huang, Qing-Dong Lu, Lin Liu, Yong-Bo Zheng, Wei-Jian Liu, Mao-Sheng Ran, Kai Yuan, and et al. 2021. "Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China" International Journal of Environmental Research and Public Health 18, no. 16: 8790. https://doi.org/10.3390/ijerph18168790