
Smartphone Applications with Sensors Used in a Tertiary Hospital—Current Status and Future Challenges

Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of AMC Healthcare Apps

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| My Cancer Diary | Point-of-Care HIV Check | Blood Culture | mAMIS | |
|---|---|---|---|---|
| Description | Personal health management application for cancer patients | Point-of-Care HIV check | Point-of-Care blood culture sampling application | Mobile electronic medical record system |
| Target users | Patients | Nurses | Physicians | Physicians and nurses |
| Period of usage | Since October 2012 | Since September 2013 | Since May 2012 | Since September 2014 * |
| Type of sensor | Camera (barcode or QR code recognition) | Camera (barcode recognition and image acquisition) | Camera (barcode recognition) | Touch ID (Fingerprint recognition) |
| Purpose of sensor | Log-in | Patient identification, result image acquisition | Patient and blood sample identification | Log-in |
| Supported OS | Android, iOS | Android | Android, iOS | iOS (8.0 and up) |
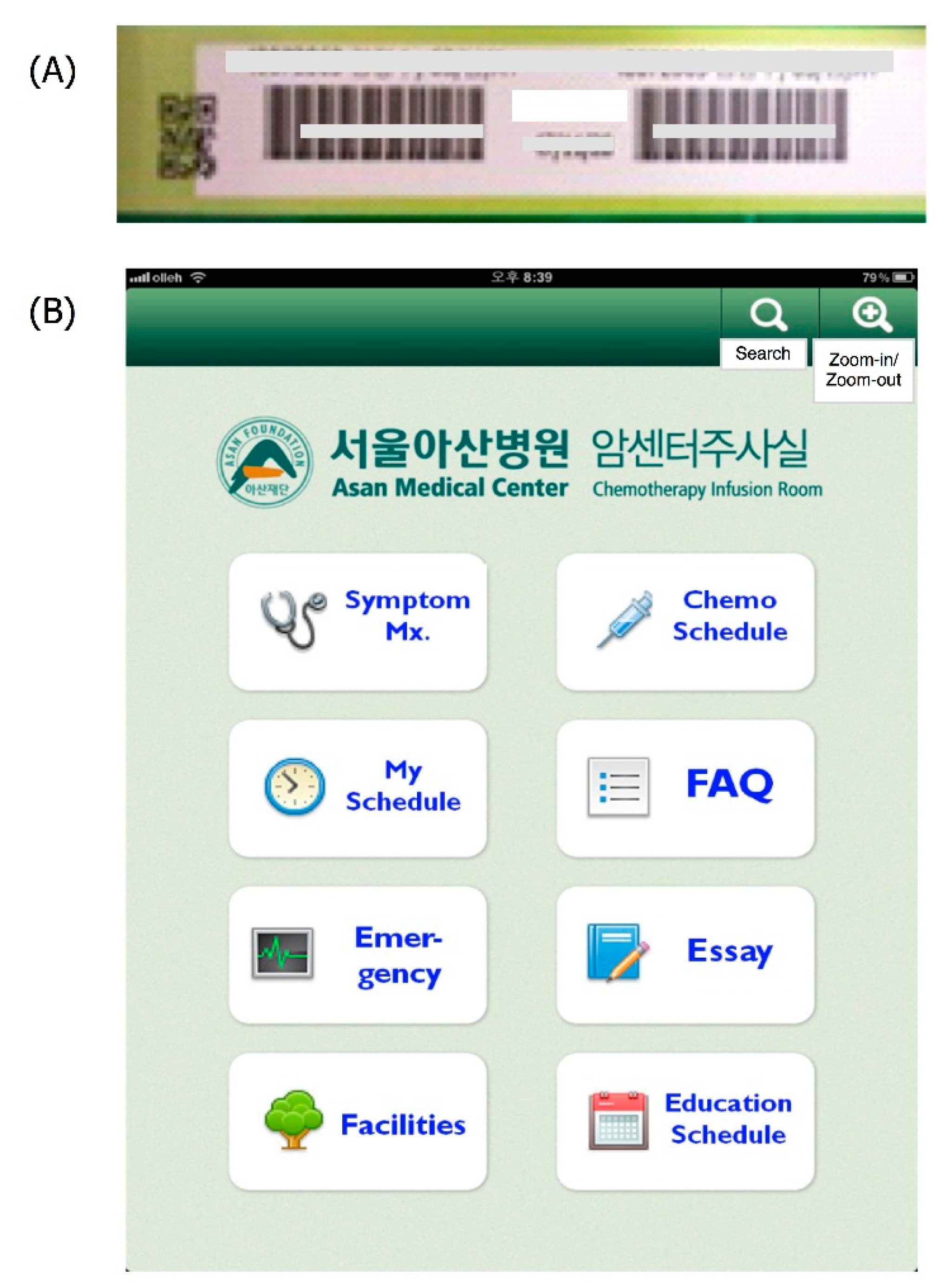
2.1.1. My Cancer Diary

2.1.2. Point-of-Care HIV Check

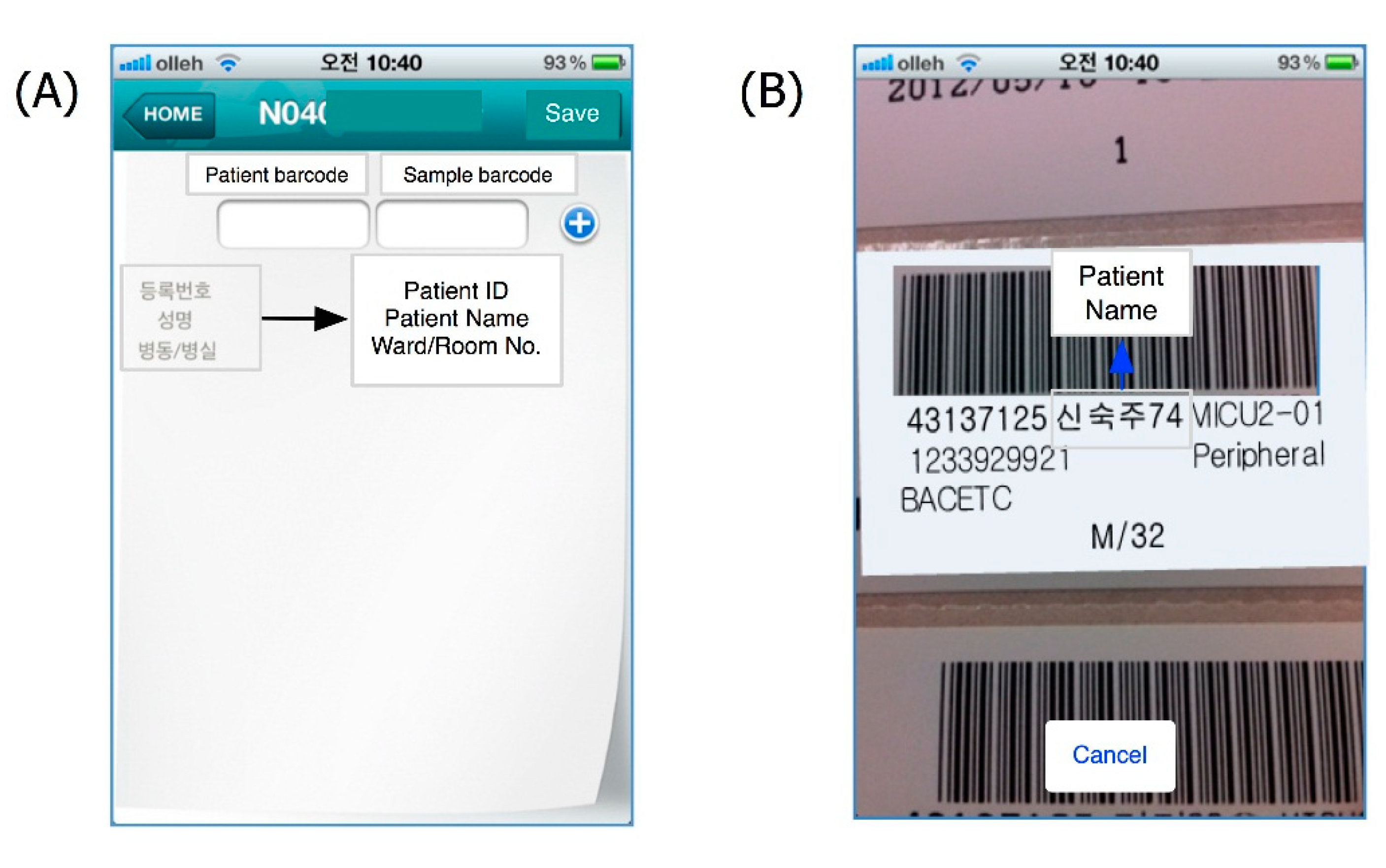
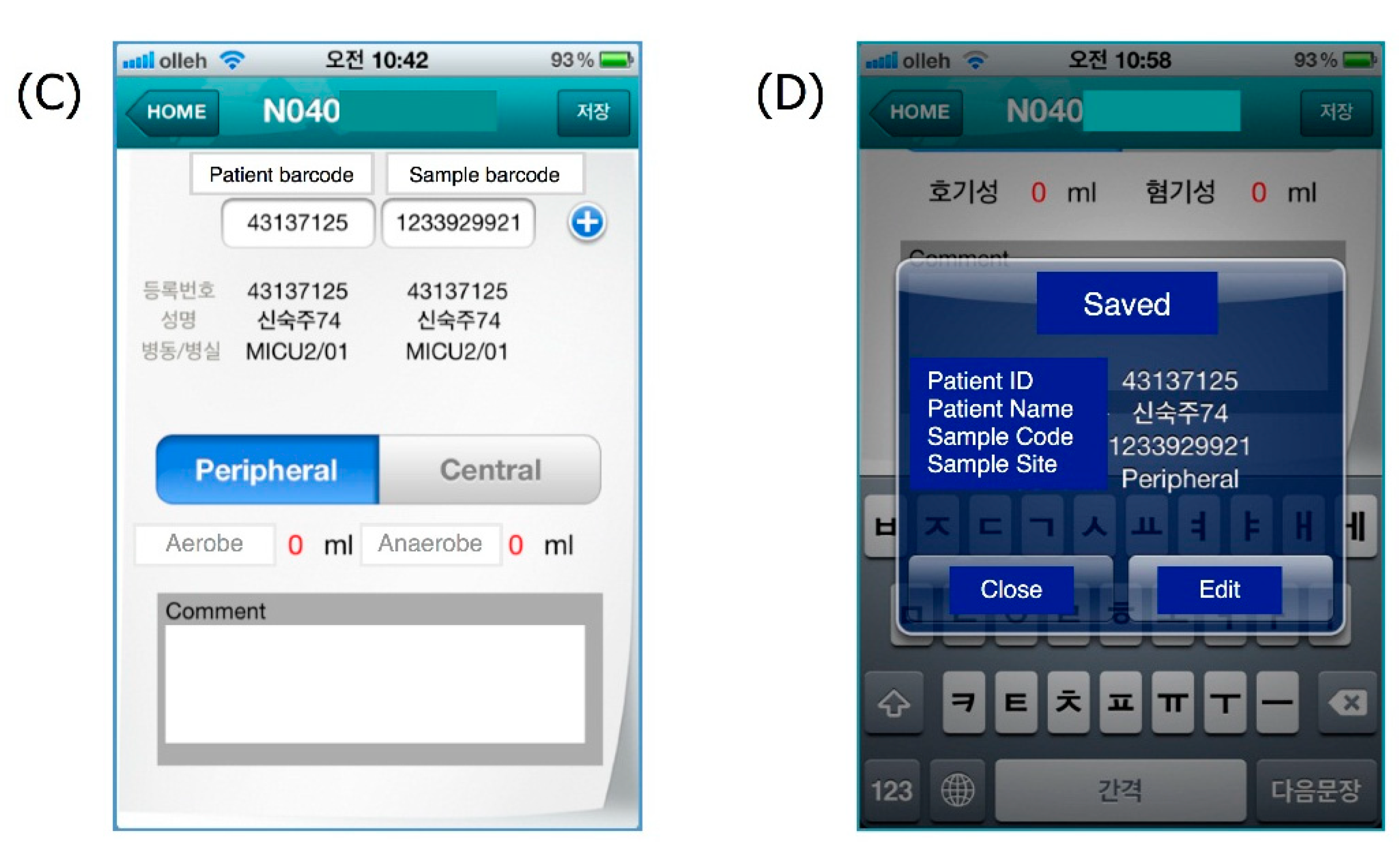
2.1.3. Blood Culture


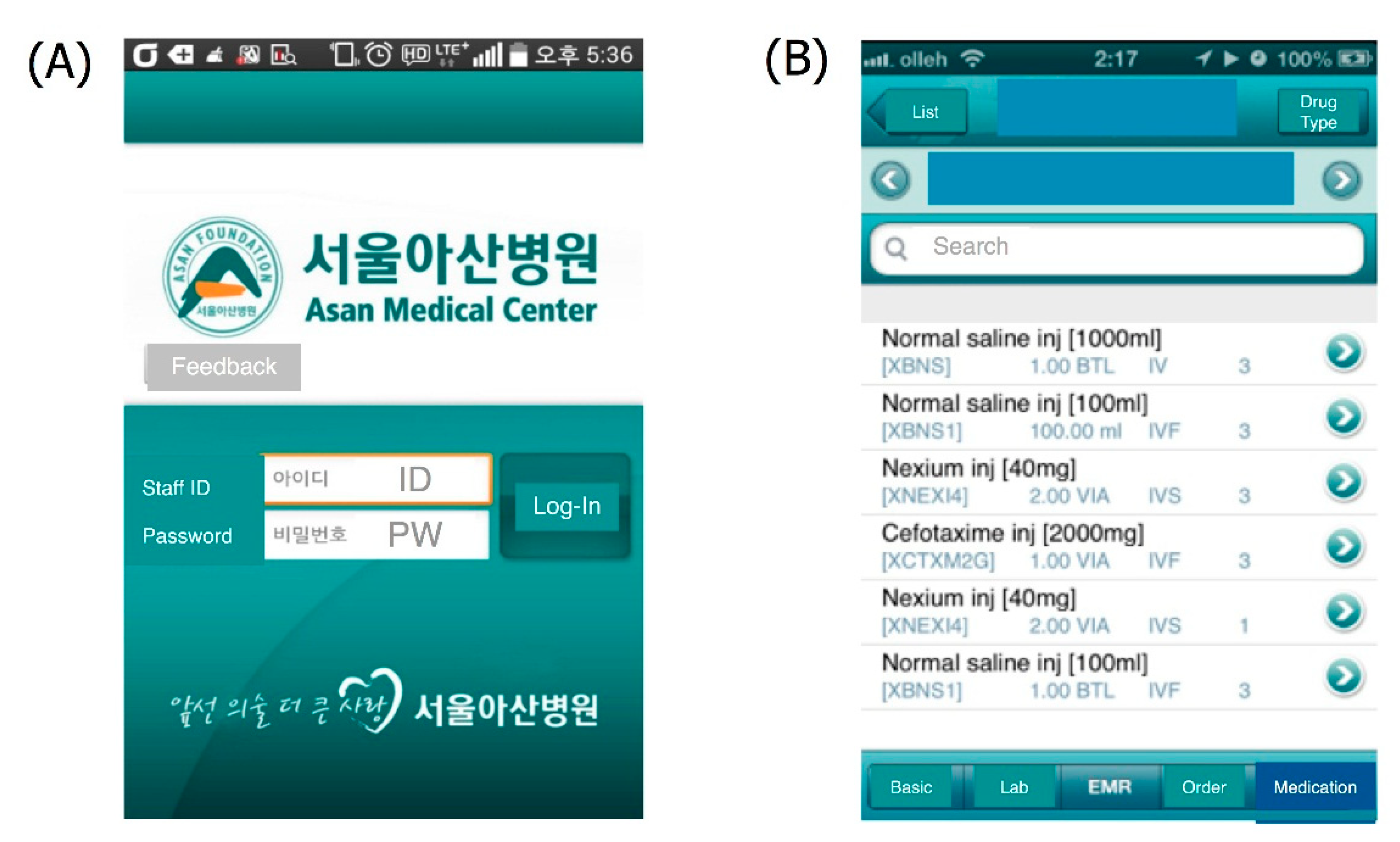
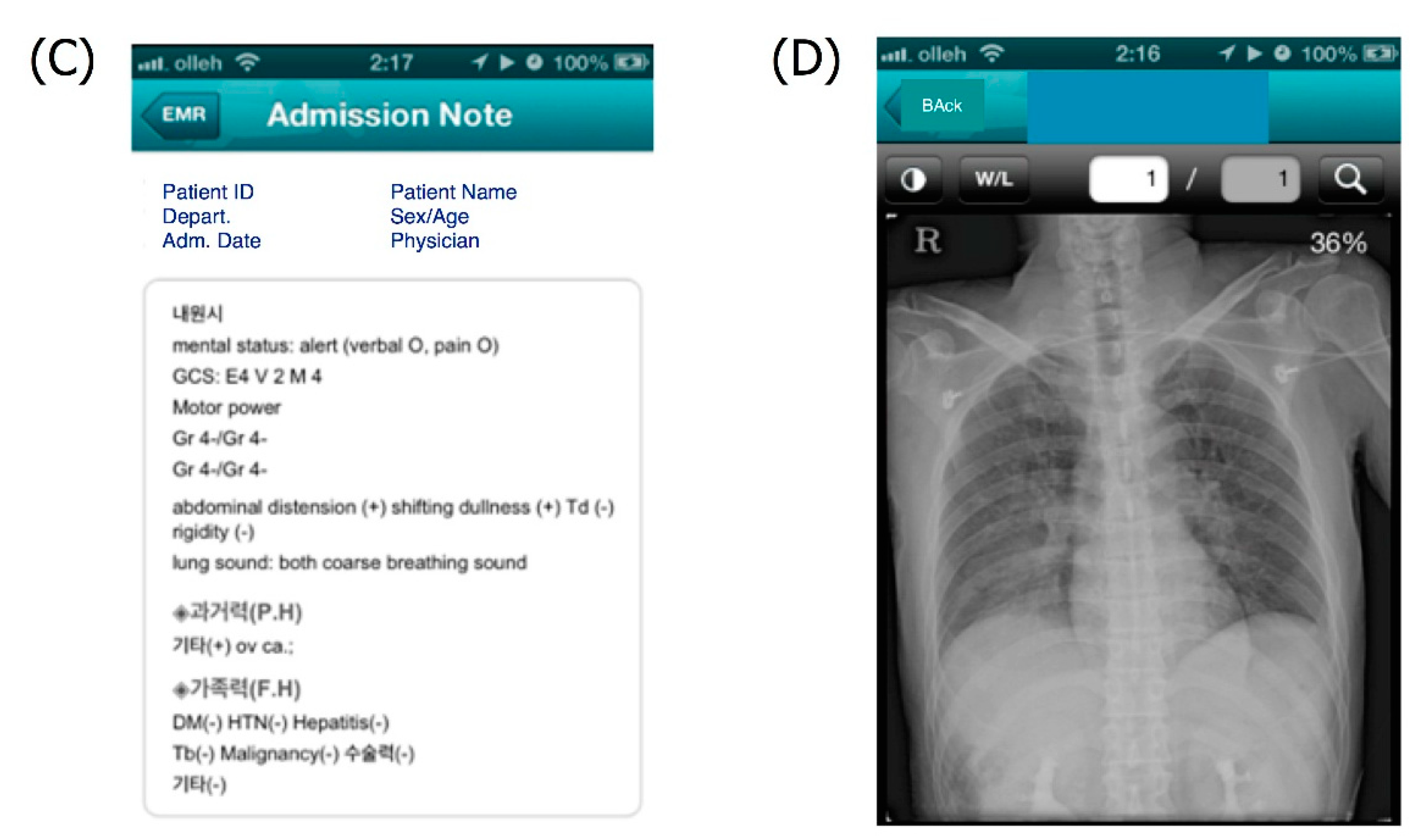
2.1.4. mAMIS


2.2. Collection and Analysis of Usage Data
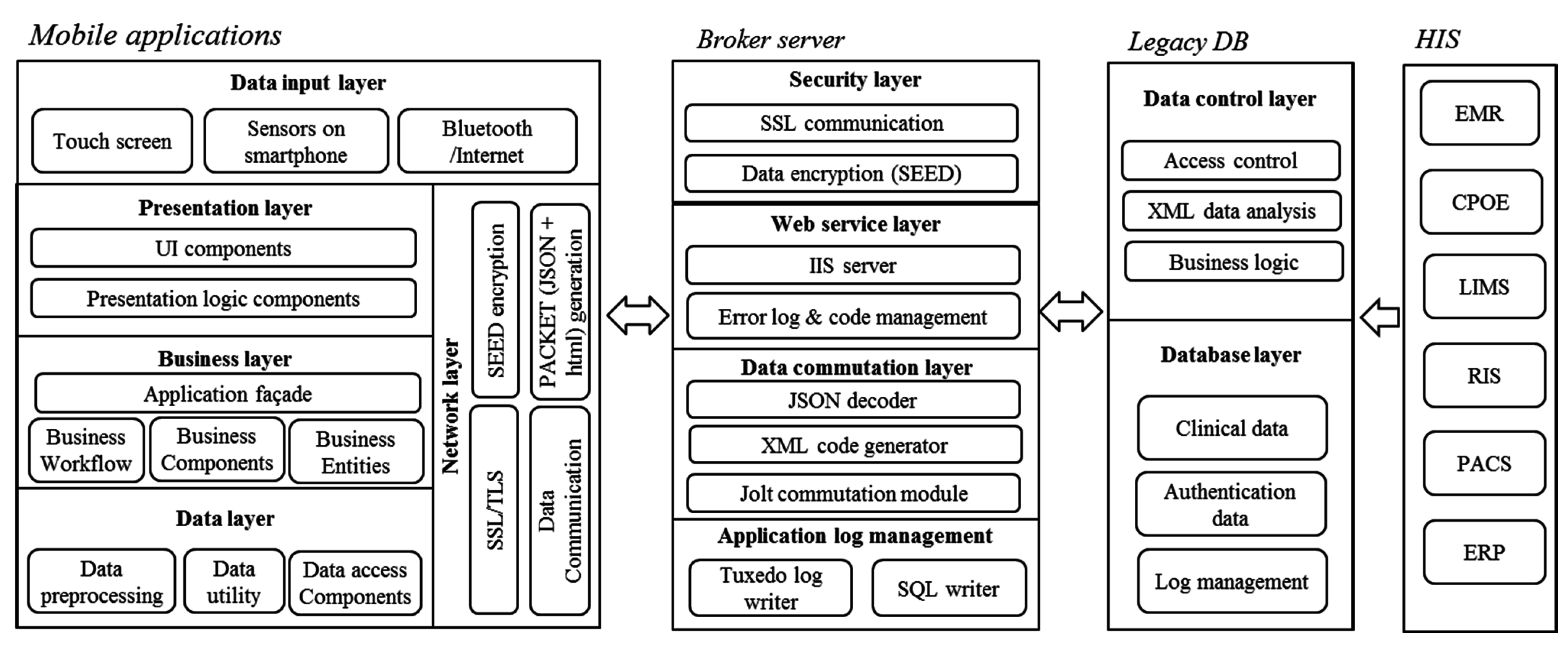
2.3. System Architecture of AMC Mobile Applications

3. Results and Discussion
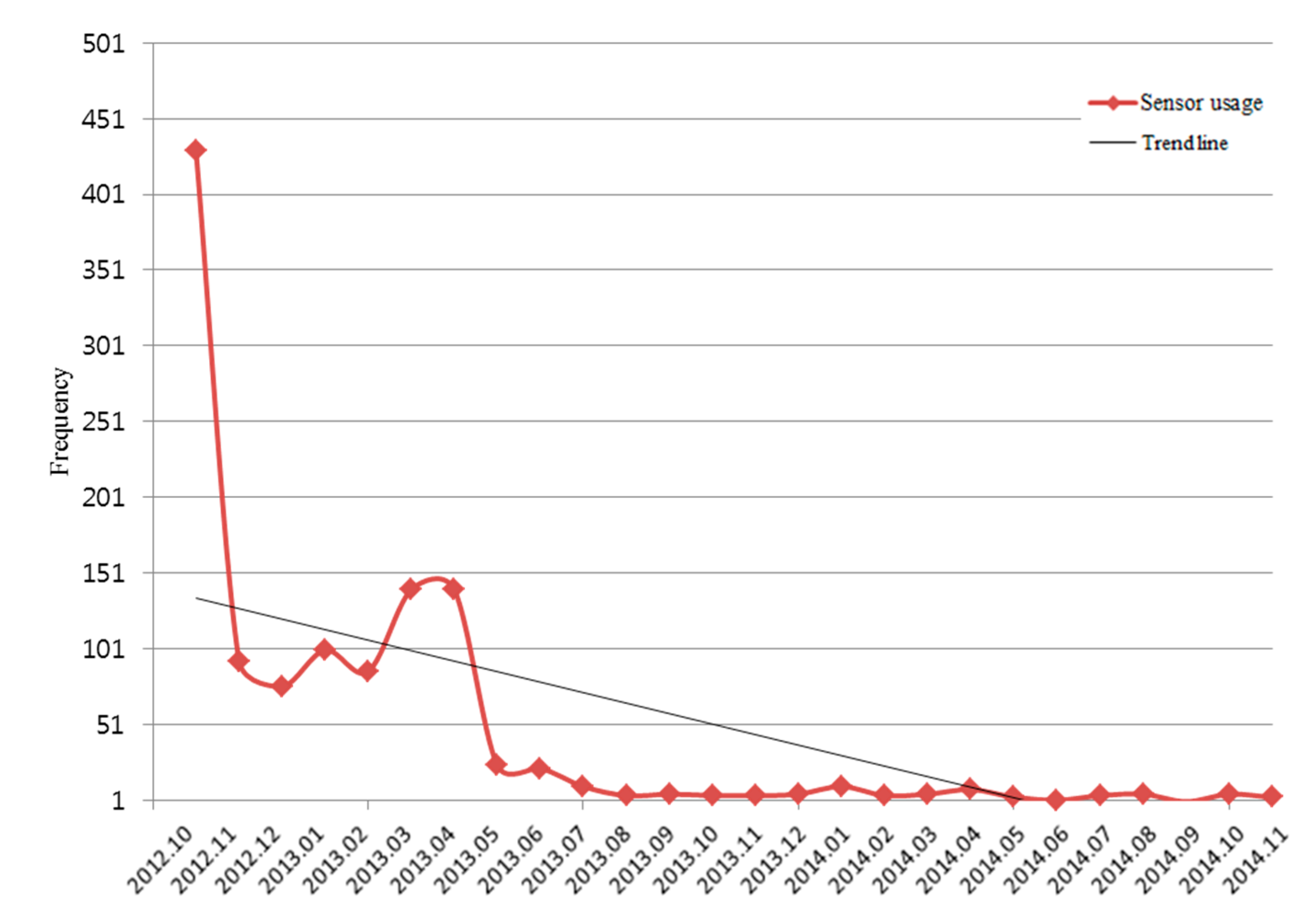
3.1. My Cancer Diary

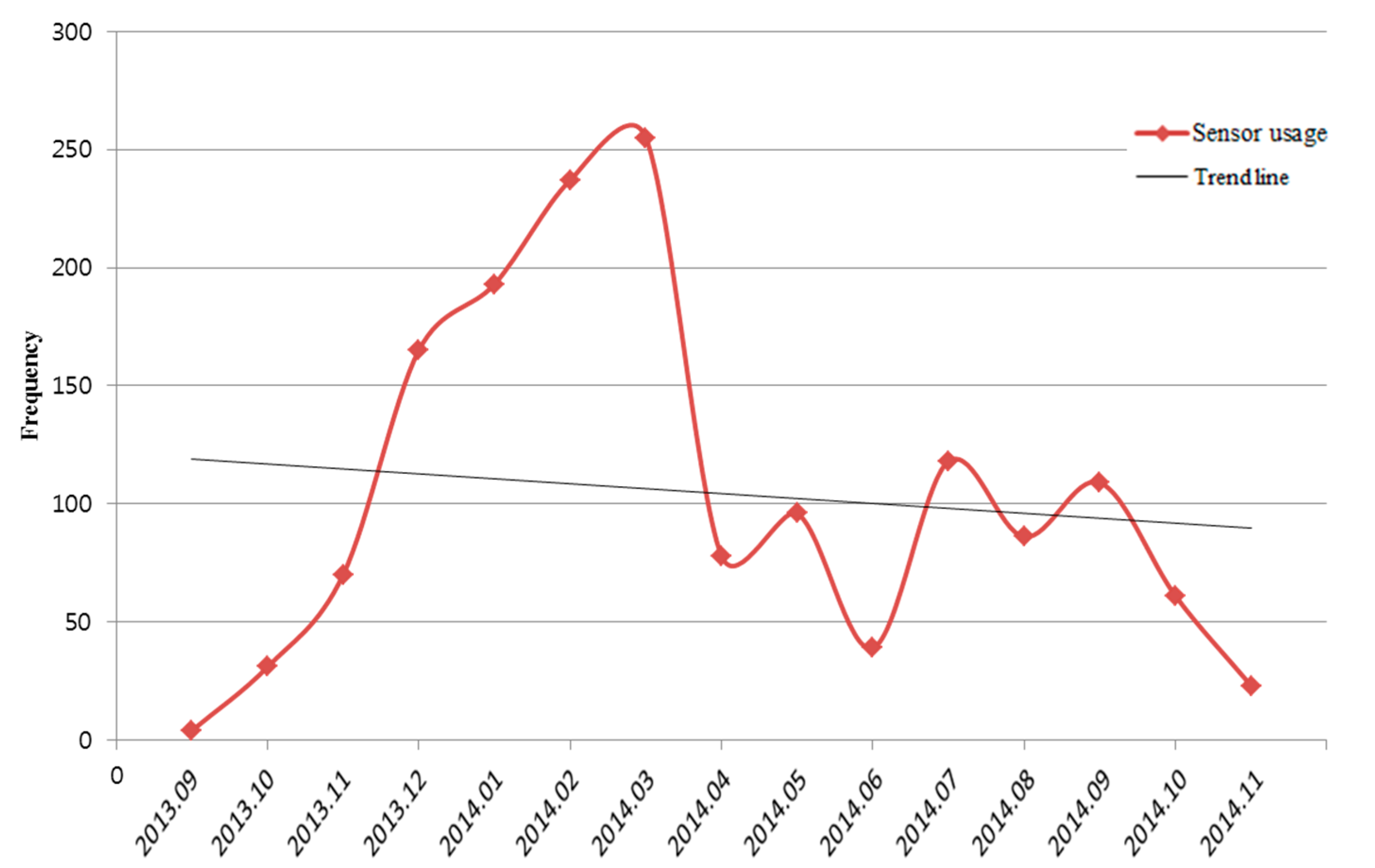
3.2. Point-of-Care HIV Check App

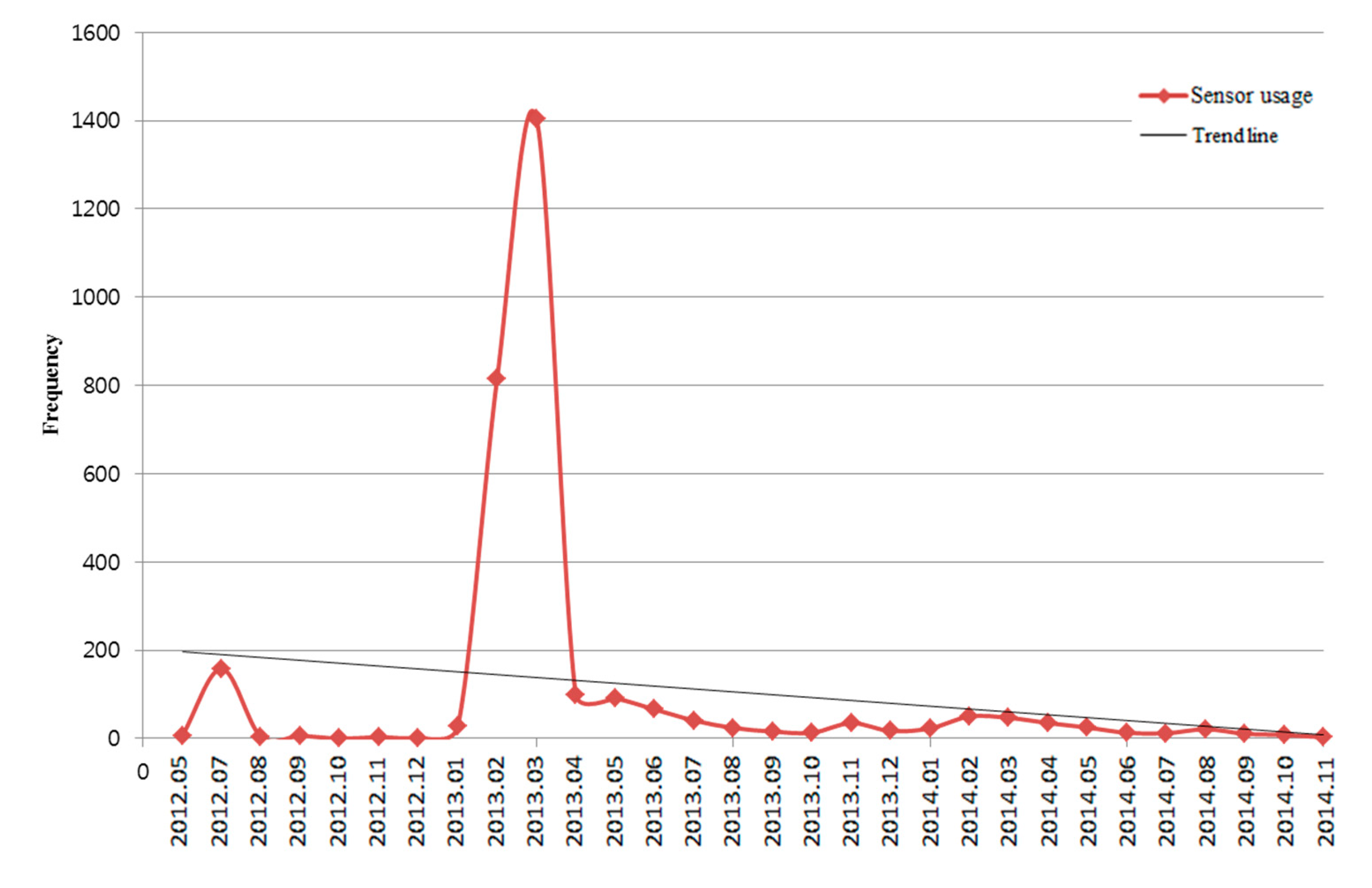
3.3. Blood Culture App

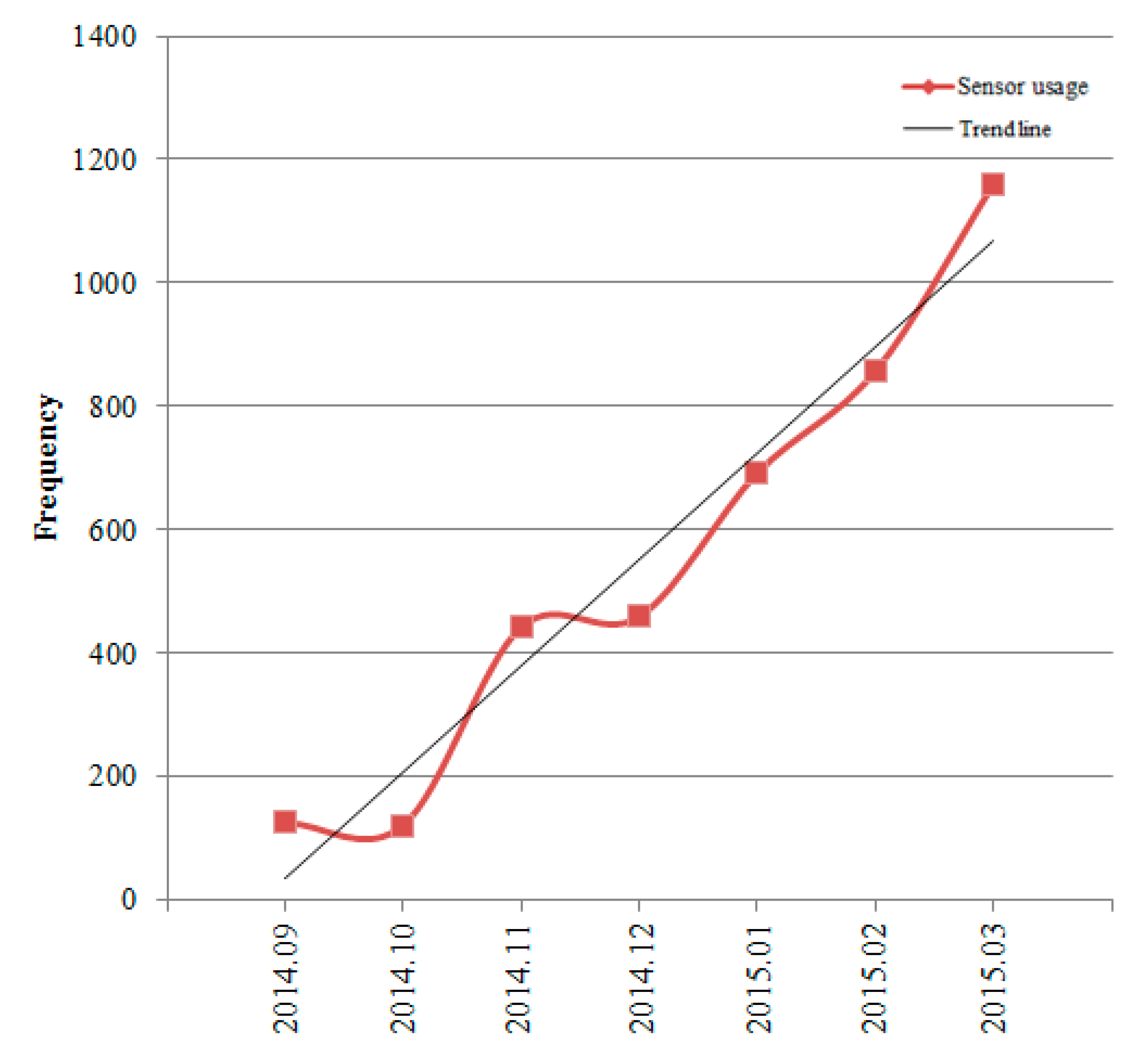
3.4. mAMIS

3.5. Analysis of Usage Patterns of Healthcare Apps with Smartphone-Based Sensors

4. Conclusions and Outlook
Author Contributions
Conflicts of Interest
References
- Forrester Research. World Mobile and Smartphone Adoption Forecast, 2014 To 2015 (Global). Available online: https://www.forrester.com/Forrester+Research+World+Mobile+And+Smart-phone+Adoption+Forecast+2014+To+2019+Global/fulltext/-/E-RES118252 (accessed on 15 December 2014).
- Topol, E.J.; Steinhubl, S.R.; Torkamani, A. Digital medical tools and sensors. JAMA 2015, 313, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Ozdalga, E.; Ozdalga, A.; Ahuja, N. The smartphone in medicine: A review of current and potential use among physicians and students. J. Med. Internet Res. 2012, 14. [Google Scholar] [CrossRef] [PubMed]
- How are Physicians Using Mobile Apps for Professional Purposes? Available online: http://www.kantarmedia-healthcare.com/more-physicians-value-and-use-mobile-apps-for-professional-purposes (accessed on 12 December 2014).
- Ventola, C.L. Mobile devices and apps for health care professionals: Uses and benefits. P&T 2014, 39, 356–364. [Google Scholar]
- Global Mobile Health Market to Grow to $49B by 2020. Available online: http://mobihealthnews.com/30616/global-mobile-health-market-to-grow-to-49b-by-2020/ (accessed on 12 December 2014).
- Emerging mHealth: Paths for Growth. Available online: http://www.pwc.com/gx/en/healthcare/mhealth/assets/pwc-emerging-mhealth-full.pdf (accessed on 12 December 2014).
- Chung, E.H.; Guise, K.D. QTC intervals can be assessed with the AliveCor heart monitor in patients on dofetilide for atrial fibrillation. J. Electrocardiol. 2015, 48, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Implanted Sensor Could Monitor Glaucoma and Prevent Blindness. Available online: http://mashable.com/2014/09/01/glaucoma-chip/ (accessed on 9 January 2015).
- Examples of MMAs the FDA HAS Cleared or Approved. Available online: http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ConnectedHealth/MobileMedicalApplications/ucm368784.htm (accessed on 15 December 2014).
- Bennet, Hatch Introduce Bill to Cut Red Tape, Boost Innovation in Health IT. Available online: http://www.hatch.senate.gov/public/index.cfm/releases?ID=750a5957-08e0-4a77-95ba-5806a7f 3ffa7 (accessed on 15 December 2014).
- Did You Know How Many Different Kinds of Sensors Go Inside a Smartphone? Available online: http://www.phonearena.com/news/Did-you-know-how-many-different-kinds-of-sensors-go-inside-a-smartphone_id57885 (accessed on 20 January 2015).
- Sebrook, H.J.; Stromer, J.N.; Shevkenek, C.; Bharwani, A.; de Grood, J.; Ghali, W.A. Medical applications: A database and characterization of apps in Apple iOS and Android platforms. BMC Res. Notes 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.J.; Kim, W.S.; Lee, J.H.; Min, S.W.; Kim, S.J.; Lee, Y.H.; Nam, S.W.; Eo, G.S.; Seo, S.G.; Nam, M.H. Asan medical information system for healthcare quality improvement. Healthc. Inf. Res. 2010, 16, 191–197. [Google Scholar] [CrossRef]
- Park, J.-Y.; Lee, G.; Shin, S.-Y.; Kim, J.H.; Han, H.-W.; Kwon, T.-W.; Kim, W.S.; Lee, J.H. Lessons learned from the development of health applications in a tertiary hospital. Telemed. J. E Health 2014, 20, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Hasan, S.; Dubey, D.; Sarangi, S. Smartphone apps as a source of cancer information: Changing trends in health information-seeking behavior. J. Cancer Educ. 2013, 28, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Porta, C.; Handelman, E.; McGovern, P. Needlestick injuries among health care workers: A literature review. AAOHN J. 1999, 47, 237–244. [Google Scholar] [PubMed]
- Trim, J.C.; Elliott, T.S. A review of sharps injuries and preventative strategies. J. Hosp. Infect. 2003, 53, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Do, A.N.; Ciesielski, C.A.; Metler, R.P.; Hammett, T.A.; Li, J.; Fleming, P.L. Occupationally acquired human immunodeficiency virus (HIV) infection: national case surveillance data during 20 years of the HIV epidemic in the United States. Infect. Control Hosp. Epidemiol. 2003, 24, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Jang, D.; Shin, S.-Y.; Seo, D.-W.; Joo, S.; Huh, S.-J. A Smartphone-based system for the automated management of point of care test results in hospitals. Telemed. J. E Health 2015, 21, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Karchmer, A.W. Infective Endocarditis. In Harrison’s Principles of Internal Medicine, 18th ed.; Longo, D.L., Fauci, A.S., Kasper, D.L., Hauser, S.L., Jameson, J., Loscalzo, J., Eds.; McGraw-Hill: New York, NY, USA, 2012; pp. 1056–1057. [Google Scholar]
- Lee, J.; Chong, Y.; Jang, S.; Kim, M.; Lee, G.; Kim, J.; Kwon, T.; Kim, W. Development of Smartphone Blood Culture Application Using Barcode and Hospital Information System: A University Hospital Experience. In Proceedings of the American Medical Informatics Association Annual Symposium, Washington, DC, USA, 16–20 November 2013; p. 851.
- Introducing Oracle Jolt. Available online: http://docs.oracle.com/cd/E13161_01/tuxedo/docs10gr3/jdg/dvintro.html (accessed on 10 April 2015).
- Ritter, F.E.; Schooler, L.J. The learning curve. In International Encyclopedia of the Social and Behavioral Sciences; Pergamon: Amsterdam, The Netherlands, 2002; pp. 8602–8605. [Google Scholar]
- Hudson, J.; Nguku, S.M.; Sleiman, J.; Karlen, W.; Dumont, G.A.; Petersen, C.L.; Warriner, C.B.; Ansermino, J.M. Usability testing of a prototype Phone Oximeter with healthcare providers in high- and low-medical resource environments. Anaesthesia 2012, 67, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Newmark, J.L.; Ahn, Y.K.; Adams, M.C.; Bittner, E.A.; Wilcox, S.R. Use of Video Laryngoscopy and Camera Phones to Communicate Progression of Laryngeal Edema in Assessing for Extubation: A Case Series. J. Intensive Care Med. 2013, 28, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Minarro-Gimenez, J.A.; Blagec, K.; Boyce, R.D.; Adlassnig, K.P.; Samwald, M. An ontology-based, mobile-optimized system for pharmacogenomic decision support at the point-of-care. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Are QR Codes Dead? Available online: http://www.forbes.com/sites/ilyapozin/2012/03/08/are-qr-codes-dead/ (accessed on 10 April 2015).
- Laksanasopin, T.; Guo, T.W.; Nayak, S.; Sridhara, A.A.; Xie, S.; Olowookere, O.O.; Cadinu, P.; Meng, F.; Chee, N.H.; Kim, J.; et al. A smartphone dongle for diagnosis of infectious diseases at the point of care. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef]
- Adhikari, S.; Blaivas, M.; Lyon, M.; Shiver, S. Transfer of real-time ultrasound video of FAST examinations from a simulated disaster scene via a mobile phone. Prehosp. Disaster Med. 2014, 29, 290–293. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.R.; Lee, Y.; Lee, G.; Lee, J.H.; Shin, S.-Y. Smartphone Applications with Sensors Used in a Tertiary Hospital—Current Status and Future Challenges. Sensors 2015, 15, 9854-9869. https://doi.org/10.3390/s150509854
Park YR, Lee Y, Lee G, Lee JH, Shin S-Y. Smartphone Applications with Sensors Used in a Tertiary Hospital—Current Status and Future Challenges. Sensors. 2015; 15(5):9854-9869. https://doi.org/10.3390/s150509854
Chicago/Turabian StylePark, Yu Rang, Yura Lee, Guna Lee, Jae Ho Lee, and Soo-Yong Shin. 2015. "Smartphone Applications with Sensors Used in a Tertiary Hospital—Current Status and Future Challenges" Sensors 15, no. 5: 9854-9869. https://doi.org/10.3390/s150509854