
Abstract
This study assessed whether self-propelled wheelchair driving can be validly detected by a new method using a set of two commonly used accelerometers.
In a rehabilitation centre, 10 wheelchair-bound persons with spinal cord injury (SCI) (aged 29–63 years) performed a series of representative daily activities according to a protocol including self-propelled wheelchair driving and other activities. Two ActiGraph GT3X+ accelerometers were used; one was attached at the wrist, the other to the spokes of the wheelchair wheel. Based on the movement intensity of the two accelerometers, a custom-made algorithm in MatLab differentiated between self-propelled wheelchair driving and other activities (e.g. being pushed or arm movements not related to wheelchair driving). Video recordings were used for reference. Validity scores between the accelerometer output and the video analyses were expressed in terms of agreement, sensitivity and specificity scores.
Overall agreement for the detection of self-propelled wheelchair driving was 85%; sensitivity was 88% and specificity 83%. Disagreement between accelerometer output and video analysis was largest for wheelchair driving at very low speed on a treadmill, wheelchair driving on a slope on a treadmill, and being pushed in the wheelchair whilst making excessive arm movements.
Valid detection of self-propelled wheelchair driving is provided by two accelerometers and a simple algorithm. Disagreement with the video analysis was largest during three atypical daily activities.
Export citation and abstract BibTeX RIS
1. Introduction
Self-propelled wheelchair driving is generally the most important physical activity for persons who are unable to walk, such as those with a SCI. Wheelchair-bound persons are at higher risk of an inactive lifestyle, which might result in deconditioning and health problems (Tasiemski et al 2005, van den Berg-Emons et al 2008, Lannem et al 2009, Tawashy et al 2009). It is important to identify to what extent wheelchair-bound people are physically active in their daily living, e.g. to tailor treatment and evaluate interventions. Different methods are available to gain insight into the amount of wheelchair driving. Although, for example, questionnaires are used, they are limited with respect to their validity and reliability (Bussmann et al 2001). For objective evaluation of wheelchair driving, various accelerometer-based systems are available. However, these devices differ depending on which aspect of wheelchair driving is being measured. For example, the amount of wheelchair driving can be measured by attaching an accelerometer to the spokes of a wheelchair wheel (Coulter et al 2011). However, this method does not allow to distinguish between self-propelled wheelchair driving and passive wheelchair driving (e.g. being pushed). Another option is to attach an accelerometer to the wrist(s); however, with this method self-propelled wheelchair driving cannot be distinguished from upper-limb activities (Warms and Belza 2004).
These limitations can be solved by the use of activity monitors consisting of several accelerometers distributed over the body (e.g. at the arms, waist and legs) (Bussmann et al 2001, Postma et al 2005). In this way, different postures can be detected and wheelchair driving can be deduced. Validity studies have shown that, although such monitors are valid for quantifying self-propelled wheelchair driving (Bussmann et al 2001, Postma et al 2005), they are complex with respect to configuration and data analysis, are a considerable burden to wear, and are relatively expensive.
Theoretically, it can be assumed that objective and methodologically sound measurement of self-propelled wheelchair driving is possible with a less complex accelerometer configuration. A simple device consisting of one accelerometer attached to the wrist and another attached to the spokes of the wheelchair seems feasible to measure the amount of self-propelled wheelchair driving. However, this latter method has not yet been described and tested for validity.
The aim of this study therefore is to assess whether this new method including a set of two accelerometers yields a valid detection of self-propelled wheelchair driving. To achieve this we performed a validation study where 10 people with a SCI performed daily activities.
2. Methods
2.1. Participants
Ten persons with SCI were selected on availability from the Rijndam Rehabilitation Center; both inpatients and outpatients were allowed to participate. Inclusion criteria were: age 18–65 years, experience with wheelchair driving for at least 3 months (wheelchair driving is the primarily mobility method), and wheelchair driving by use of two hands. Exclusion criteria were: individuals not able to use a hand-rim propelled wheelchair independently for longer distances (i.e. >100 m).
The study was approved by the Medical Ethics Committee of the Erasmus MC, University Medical Center Rotterdam. Informed consent was obtained from all patients.
2.2. Theoretical background
Wheelchair-bound persons can perform several physical activities while sitting in their wheelchair. For example, they can use their arms for self-propelled wheelchair driving or for different types of upper-limb activities related to e.g. self-care, office work and arm exercises. . Self-propelling a wheelchair differs from other upper-limb activities by simultaneous movement of the arms and the wheelchair wheels. This concept can be used to distinguish self-propelled wheelchair driving from other activities. Other 'activities' include all activities (with the exception of self-propelled wheelchair driving), such as upper-limb activities, sitting in a wheelchair without arm movements, and passive wheelchair driving such as being pushed with or without upper-limb activities.
Accelerometers are sensitive to detect accelerations due to movement and allow prolonged measurement in daily life. The number of counts per time interval (mostly used in accelerometer research and which expresses the intensity of movement) seems appropriate for the purpose of detecting self-propelled wheelchair driving. By attaching and synchronizing one accelerometer to the wrist and the other accelerometer to the spokes of the wheelchair, both arm and wheel movements can be measured simultaneously; this allows reliable quantification of the amount of self-propelled wheelchair driving.
2.3. Accelerometry
Two ActiGraph GT3X+ accelerometers were used (Arnardottir et al 2013). The ActiGraph GT3X+ includes a 3D accelerometer. One accelerometer was worn at the dorsal side of the wrist using a wristband. The other accelerometer was attached to the spokes of the wheelchair (as close as possible to the axis) using a strong Velcro band allowing no undesired movements. A sample frequency of 30 Hz and an epoch time of 1 s was used for analysis of the ActiGraph data. We developed an algorithm in MatLab that differentiates between self-propelled wheelchair driving and other activities (figure 1). The algorithm was based on the vector counts of both ActiGraph accelerometers. Prior to the present study, we determined the settings for the algorithm based on several test measurements. These test measurements were performed with both wheelchair users and non-users and included activities like wheelchair driving at several speeds and manoeuvring.
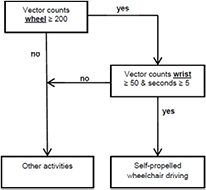
Figure 1. Flow diagram of the algorithm self-propelled wheelchair driving.
Download figure:
Standard image High-resolution image2.4. Protocol
In the rehabilitation centre participants were asked to perform a standard set of activities, partly in a movement laboratory and partly in a semi-natural setting (including a simulated apartment). The activity protocol consisted of several activities which were assumed to be representative for everyday life in people with SCI, including different types of self-propelled wheelchair driving, e.g. hand-rim wheelchair driving and hand biking (see table 1). In addition, some critical activities were added to the protocol, i.e. activities that are potentially vulnerable to be falsely detected, such as being pushed whilst making excessive arm movements. Participants only performed activities that they were able to execute.
Table 1. Performed activities and differences in duration of determined self-propelled wheelchair driving from video analysis and accelerometry.
| Activities | |||||
|---|---|---|---|---|---|
| Standard protocol | N | Total duration video analysis (s) | Total duration ActiGraph GTX3 + (s) | Absolute difference (s) |
Percentage difference (%) |
| 1 min wheelchair driving on a treadmill at 1 km h−1 | 9 | 546 | 469 | −77 | 14 |
| 1 min wheelchair driving on a treadmill at 2 km h−1 | 10 | 539 | 522 | −17 | 3 |
| 1 min wheelchair driving on a treadmill at 4 km h−1 | 10 | 528 | 514 | −14 | 3 |
| 1 min wheelchair driving on a slope on a treadmill at 4 km h−1: | 8 | 356 | 306 | −50 | 14 |
| Once round (gymnastic hall) at slow speed wheelchair driving on flat ground | 10 | 666 | 636 | −30 | 5 |
| Once round (gymnastic hall) at normal speed wheelchair driving on flat ground | 10 | 515 | 510 | −5 | 1 |
| Once round (gymnastic hall) rapidly wheelchair driving on flat ground | 10 | 385 | 382 | −3 | 1 |
| Once round (gymnastic hall) at slow speed hand cycling on flat ground | 4 | 187 | 179 | −8 | 4 |
| Once round (gymnastic hall) at normal speed hand cycling on flat ground | 4 | 159 | 154 | −5 | 3 |
| Once round (gymnastic hall) rapidly hand cycling on flat ground | 4 | 137 | 135 | −2 | 1 |
| Being pushed, with participant's arms hanging still (1 min) | 10 | 0 | 0 | 0 | |
| Being pushed while participant's hands are moving (1 min) | 10 | 0 | 258 | 258 | |
| Manoeuvring, e.g. turning around or changing from position in the area, (1 min) | 10 | 230 | 235 | 5 | −2 |
| Other (mainly sitting still between activities) | 6 | 98 | 108 | 10 | −10 |
| Semi-natural setting (activities performed in own manner and pace) | |||||
| Driving independently towards the practice apartment | 10 | 118 | 122 | 4 | −3 |
| Opening the door, driving through and closing the door | 9 | 134 | 140 | 6 | −4 |
| Transfer to bed | 6 | 0 | 1 | 1 | |
| Laying supine on bed | 6 | 0 | 1 | 1 | |
| Transfer back to wheelchair | 6 | 5 | 5 | 0 | 0 |
| Driving to the kitchen via elevator | 10 | 648 | 665 | 17 | −3 |
| Driving to a draining board; doing the dishes; cleaning up the dishes | 10 | 192 | 218 | 26 | −14 |
| Driving towards the hallway | 10 | 406 | 391 | −15 | 4 |
| Putting on a coat | 9 | 0 | 0 | 0 | |
| Wheelchair driving outdoors | 9 | 824 | 793 | −31 | 4 |
| Handbiking outdoors | 3 | 174 | 155 | −19 | 11 |
| Other (mainly sitting still between activities) | 6 | 7 | 10 | 3 | |
aActigraph GTX3 + minus video data. bPercentage differences are given if total duration of the video analysis is >50 s.
2.5. Reference method
During execution of the protocol, video recordings were made with a handheld digital video camera as reference to the ActiGraph data. The camera was focused on the plane of the wheel of the wheelchair. During the activities that were performed in the semi-natural setting the camera was not stopped, so that the time between the activities were also included in the analysis. All video recordings were analysed separately by two independent researchers. Activities were scored per second as self-propelled wheelchair driving, or other activities. 'Self-propelled wheelchair driving' was defined as: independently propel oneself to another location, while sitting in a wheelchair or hand bike, as a result of arm power. This definition also includes propelling oneself for smaller distances, such as manoeuvring. All other activities were defined as 'other activities'. In case of any disagreement, a third reviewer was included to achieve consensus.
2.6. Data analysis
The continuous outcome of the ActiGraph accelerometers was compared with the continuous outcome of the video analysis, both with a time resolution of 1 s. The following validity measures were calculated per measurement:
- Agreement: percentage of correct classification by the accelerometers;
- Sensitivity: percentage of correct classification of self-propelled wheelchair driving divided by time of actual self-propelled wheelchair driving;
- Specificity: percentage of correct classification of other activities divided by time of actual other activities.
In addition, the duration in seconds of self-propelled wheelchair driving as established by accelerometry and the video analysis were calculated for each measurement in total and for each activity of the protocol separately. Differences between accelerometry and the video analysis were provided in both seconds and percentages.
2.7. Statistical analysis
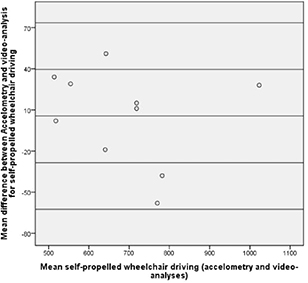
The individual and group mean for the total protocol was calculated for the sensitivity, specificity and agreement scores. The mean difference in duration of self-propelled wheelchair driving determined by accelerometry and video analysis was tested with a T-test. Statistical significance was set at a p-value <0.05. Differences between video analysis and accelerometry for duration of self-propelled wheelchair driving were also expressed in a Bland Altman plot.
3. Results
A total of 10 participants with SCI (10 males; mean age 44.8 ± 11.5 years) were included. Of all participants, 80% had a thoracic or low cervical lesion (C7 and below) and 20% had a high cervical lesion (C6 and higher). Table 2 presents the characteristics of the participants. Not all activities in the testing protocol could be performed by all the participants; table 1 presents an overview of the performed activities.
Table 2. Characteristics of the study participants.
| Participant number | Sex | Age (years) | Lesion level | Time since injury (years) | Complete/incomplete lesion |
|---|---|---|---|---|---|
| 1 | Male | 29 | T4 | 8 | Complete |
| 2 | Male | 60 | T10 | 12 | Complete |
| 3 | Male | 34 | T12 | 16 | Complete |
| 4 | Male | 48 | T7 | 12 | Complete |
| 5 | Male | 63 | T3 | 13 | Complete |
| 6 | Male | 40 | C7 | 13 | Incomplete |
| 7 | Male | 35 | T12 | 1 | Complete |
| 8 | Male | 45 | C4 | 14 | Incomplete |
| 9 | Male | 55 | T4 | 12 | Complete |
| 10 | Male | 39 | C5 | 0.5 | Complete |
Agreement between the video analysis between the two researchers was 95.6% (range 92.3–98.5%) per measurement per individual participant. Mean duration (SD) of the measurements was 21.7 (6.0) min per participant. According to the video analysis, 52.6% of the total measurement time was spent on self-propelled wheelchair driving.
3.1. Agreement between video data and accelerometry
The total agreement between the video analysis and the accelerometer data was 85.2%, with agreement per measurement ranging from 76.7% to 92.3% (table 3).
Table 3. Validity scores.
| Participant number | Sensitivity (%) | Specificity (%) | Agreement (%) |
|---|---|---|---|
| 1 | 87.8 | 91.2 | 89.3 |
| 2 | 86.3 | 82.4 | 80.7 |
| 3 | 83.1 | 78.5 | 76.7 |
| 4 | 87.4 | 86.1 | 86.6 |
| 5 | 86.1 | 85.1 | 84.8 |
| 6 | 90.0 | 88.0 | 87.7 |
| 7 | 91.6 | 79.1 | 87.2 |
| 8 | 88.5 | 72.6 | 80.9 |
| 9 | 93.0 | 84.5 | 92.3 |
| 10 | 89.3 | 85.4 | 85.7 |
| Group mean | 88.3 | 83.3 | 85.2 |
3.2. Sensitivity, specificity
The overall sensitivity for the detection of self-propelled wheelchair driving was 88.3% (range 83.1–93.0%). The overall specificity was 83.3% (range 72.6–91.2%) (table 3).
3.3. Duration
Based on the video analyses, the summed duration of self-propelled wheelchair driving was 6854 s, and 6182 s for other activities. According to accelerometry, these durations were 6909 s (+0.80%) and 6127 s (−0.90%), respectively. On average, per measurement the detection of self-propelled wheelchair driving was overestimated by 5.5 (SD 34 s) (p-value=0.60) (figure 2). Table 1 provides an overview of the duration of determined self-propelled wheelchair driving for each activity. The largest differences in the detection of self-propelled wheelchair driving between accelerometry and video analyses were found for being pushed while the arms were moving, wheelchair driving at low speed on a treadmill, and wheelchair driving on a slope on a treadmill.
{kind=link}
Figure 2. Difference between video analysis and accelerometry for self-propelled wheelchair driving.
Download figure:
Standard image High-resolution image{kind=link}
4. Discussion
In the present study, we assessed whether self-propelled wheelchair driving could be validly detected using two accelerometers; one attached to the wrist, the other to the spokes of a wheelchair wheel. The overall validity scores appeared to be adequate; these percentages were 85.2 (agreement), 83.3 (sensitivity), and 83.3 (specificity).
When looking at the results of specific activities of the protocol, it showed that disagreement between the accelerometer device and video analysis was larger in three activities. Two of them were wheelchair driving at a very low speed on a treadmill and wheelchair driving on a slope on a treadmill. Post-hoc analyses of the video recordings of these activities indicated that the movements made during these activities were somewhat abnormal. This was partly caused by the very slow speed on the treadmill, e.g. this speed was slower than the self-selected over ground speed. The unnatural character of wheelchair driving on a treadmill was most strongly expressed in these activities.
A third main source of disagreement was the activity in which the wheelchair was being pushed while the participants was asked to make arm movements. However, this instruction resulted in participants making excessive arm movements without any breaks. As a result, the vector counts of the accelerometer at the wrist exceeded the threshold of 50 counts s−1 and, therefore, self-propelled wheelchair driving was detected instead of other activities. Again, we feel that the way this activity was performed does not reflect normal daily behaviour. It can be assumed that in daily life wheelchair-bound individuals will make less extreme and less prolonged arm movements. As a result, the threshold for self-propelled wheelchair driving will not (or will seldom) be exceeded. Although these activities are not necessarily representative for real life, and thereby will only have a weak effect on daily life validity, they pointed out well where the algorithm may go wrong. This allows people considering using the device in the future to make an informed assessment of whether these activities are likely to compromise their study or not.
A strength of our study is that daily activities were partly performed in a natural setting that invited participants to perform the activities at their own pace and in their own way. Therefore, these activities were performed in the most natural way possible, which allows more easily generalization to a daily life setting. This part of the protocol showed one activity with a larger difference between accelerometry and video: while doing the dishes self-propelled wheelchair driving was overestimated from accelerometry (14%). Post-hoc analyses of the video recordings indicated that sometimes the wheelchair moved while participants were making arm movements at the same time; e.g. the participants reached out for a towel while the wheelchair was moving, or participants pushed themselves away from the sink. Despite the fact that these activities were different from self-propelled wheelchair driving, they were detected as such by accelerometry. However we do not believe this misclassification is undesirable for the analysis because the nature of the movements is similar to self-propelled wheelchair driving and therefore these activities can also be detected as physical activity.
Although our method does not differentiate between different types of self-propelled wheelchair driving (e.g. hand-cycling and hand-rim wheelchair driving), it was able to distinguish these types of self-propelled wheelchair driving as a class distinct from other activities. In this study, although no differences were found in the validity of the detection of these two types of self-propelled wheelchair driving, it should be noted that only 4 individuals performed hand-cycling. Further, persons with a cervical SCI use different wheelchair propulsion techniques (pulling movement) compared to individuals with a thoracic lesion (pushing movement) (Postma et al 2005). However, the present results do not suggest that validity depends on the level of the lesion (thoracic or cervical).
The method used in the present study is relatively simple; this applies to both the sensor configuration (only two sensor units) and the analysis algorithms. Moreover, the methodology can be used in other applications. In the present study we used the ActiGraph accelerometer and MatLab algorithms, but this approach can also be used with other brands of accelerometers and signal analysis software.
The use of only one accelerometer attached to the body implies minimal burden when worn compared with other instruments (Bussmann et al 2001, Postma et al 2005). Further, the two ActiGraph accelerometers can perform measurements for more than 1 week. Also, the ActiGraph accelerometers are water resistant (including rain and splashing water) and therefore can be used without any harm when people use their wheelchair outside.
In this study the ActiGraph accelerometer was placed close to the centre of the wheel in order to standardize the measurements, but the placement of the ActiGraph on the wheel should not affect the output. However, practical disadvantages can arise when individuals make use of several wheelchairs (then, the wheelchair accelerometer needs to be replaced) and when people are only partially wheelchair bound (because then walking, for example, will be less well detected).
4.1. Limitations
Although we aimed to make the measurement setting as natural as possible, the measurements were performed in a rehabilitation centre and not in the daily life setting of the participants; this may have influenced performance of the activities. We aimed to select activities that were as representative as possible, as well as activities expected to be potentially difficult to detect. Nevertheless, the final protocol is a limited selection, in which three of the activities were less representative for activities of normal daily life.
4.2. Future research
This study was performed in wheelchair-bound individuals with a spinal cord injury. Although our measurement method is probably also applicable in other populations (e.g. among individuals with multiple sclerosis or stroke) this has yet to be explored. As discussed, although the concept we used might be generalized to other synchronized accelerometers and analysis software, investigation of the most optimal thresholds is still required.
In this study, self-propelled wheelchair driving was the activity of interest. Therefore, we did not differentiate between different types of activities within the 'Other activities' category. For example, upper-limb movements not related to wheelchair driving might be an activity of specific interest. This activity may be partially detected by the original software of the accelerometers. Additional research is needed to explore the potential of these more detailed analyses.
5. Conclusion
This study shows that valid detection of self-propelled wheelchair driving is provided by two accelerometers (one attached at the wrist, the other to the spokes of a wheelchair wheel) and a simple algorithm. The method is able to differentiate between self-propelled wheelchair driving and other activities (e.g. being pushed, or arm movements not related to wheelchair driving). Disagreement with the video analysis was larger in three atypical activities performed by the participants.